
Abstract
BACKGROUND:
Described to be antithrombotic and antihypertensive, nattokinase is consumed for putative cardiovascular benefit. However, no large-scale, long-term cardiovascular study has been conducted with nattokinase supplementation.
OBJECTIVE:
To determine the effect of nattokinase on subclinical atherosclerosis progression and atherothrombotic biomarkers.
METHODS:
In this double-blinded trial, 265 individuals of median age 65.3 years, without clinical evidence of cardiovascular disease (CVD) were randomized to oral nattokinase 2,000 fibrinolytic units or matching placebo. Primary outcome was rate of change in subclinical atherosclerosis measured by serial carotid ultrasound every 6 months as carotid artery intima-media thickness (CIMT) and carotid arterial stiffness (CAS). Additional outcomes determined at least every 6 months were clinical parameters including blood pressure and laboratory measures including metabolic factors, blood rheology parameters, blood coagulation and fibrinolysis factors, inflammatory markers and monocyte/macrophage cellular activation markers.
RESULTS:
After median 3 years of randomized treatment, annualized rate of change in CIMT and CAS did not significantly differ between nattokinase supplementation and placebo. Additionally, there was no significant effect of nattokinase supplementation on blood pressure or any laboratory determination.
CONCLUSIONS:
Results of this trial show that nattokinase supplementation has a null effect on subclinical atherosclerosis progression in healthy individuals at low risk for CVD.
Keywords
Introduction
Nattokinase, prepared from soybeans fermented with the Bacillus subtilis, is a serine protease extracted from natto, a traditional Japanese food that has been consumed for more than 1,000 years [1]. Nattokinase has been described as a fibrinolytic enzyme with antithrombotic and antihypertensive effects [2, 3]. As such, nattokinase supplementation is growing in popularity with putative cardiovascular benefits. However, no large-scale, long-term study has been conducted to determine the cardiovascular effects of nattokinase supplementation. The Nattokinase Atherothrombotic Prevention Study (NAPS) was designed to study the effects of nattokinase supplementation on atherosclerosis progression and cognitive aging in healthy men and women. Atherothrombotic associated parameters including metabolic factors, hemorheological parameters, blood coagulation and fibrinolysis factors, inflammatory markers and monocyte/macrophage cellular activation markers were also studied.
Methods
Trial design
NAPS was a single-center, randomized, double-blinded, placebo-controlled clinical trial that tested whether daily nattokinase supplementation would reduce progression of subclinical atherosclerosis, measured by serial carotid ultrasound as carotid artery intima-media thickness (CIMT) and carotid arterial stiffness (CAS). Eligible participants included healthy men and women without clinical evidence of cardiovascular disease (CVD). Specific inclusion criteria were age 55 years and older and male or postmenopausal female (no uterine bleeding for > 6 months). Exclusion criteria included: clinical signs, symptoms or personal history of CVD; diabetes mellitus or fasting serum glucose > 140 mg/dL; plasma triglycerides > 500 mg/dL; uncontrolled hypertension (systolic blood pressure (BP) > 160 mmHg or diastolic BP > 110 mmHg); uncontrolled tachycardia or irregular heart rate (i.e., atrial fibrillation); untreated thyroid disease; renal insufficiency (serum creatinine > 2.0 mg/dL); life threatening illness with prognosis < 5 years; current use of lipid-lowering medication; current use of food supplements containing soy, soy protein, isoflavone or other phytoestrogens; sensitivity or allergy to soy or nuts; regular use of aspirin or other antiplatelet medication; use of anticoagulants; or, bleeding diatheses or tendencies. The trial was approved by the institutional review board of the University of Southern California and is registered on clinicaltrials.gov (NCT02080520). All participants provided written informed consent and an independent external data safety and monitoring board oversaw participant safety and trial conduct.
Random assignment to trial intervention
Eligible and consenting participants were randomized in a 1:1 allocation to receive oral nattokinase 2,000 fibrinolytic units daily or matching placebo. Blocked randomization (with a block size of 4) was further stratified on baseline CIMT (< 0.75 mm or ≥0.75 mm). The nattokinase supplement and matching placebo were provided gratis by Jarrow Formulas (Los Angeles, CA). Except for one member of the data coordinating center, all participants, trial investigators and staff were blinded to randomization assignments. No company had any role in the collection or analysis of data or in the preparation or review of the manuscript or the trial protocol.
Trial follow-up
Recruitment was based on a planned 5-year trial (2-year recruitment period and 3 years of randomized treatment). Following randomization, each participant was followed every month for the first 6 months, then every 3 months for 36 months. An optional visit at 1-week post-randomization was comprised of a blood sample for fibrinogen, ristocetin cofactor, factor VIII, von Willebrand factor (vWF) antigen, tissue plasminogen activator (tPA) antigen, plasminogen activator inhibitor-1 (PAI-1), D-dimers, red blood cell (RBC) aggregation (plasma), RBC aggregabiliity (polymer), erythrocyte sedimentation rate (ESR), whole blood viscosity and plasma viscosity. All screening and follow-up visits occurred at the USC Atherosclerosis Research Unit (ARU) research clinic.
Assessment of subclinical atherosclerosis progression
Primary trial outcomes were: 1) The rate of change of intima-media thickness of the far wall of the right distal common carotid artery (CIMT); and, 2) rate of change in CAS (measured as arterial distensibility and compliance) of the right distal common carotid artery. CAS measures were calculated from carotid artery lumen diameters measured at systole and diastole and systolic and diastolic BP. Specifically, two measures of CAS were computed as:
Arterial distensibility = [2 (D S - D D )/ - D D ]/ - PP
Arterial compliance =
Where DS and DD represent carotid lumen diameters at systole and diastole, respectively, and PP represents pulse pressure (systolic minus diastolic pressure). Lumen diameters were measured at the same site where CIMT was measured. CIMT and CAS measurements were obtained from high resolution B-mode ultrasonograms of the carotid artery that were obtained two times at baseline (at screening and randomization visits) and every 6 months during post-randomization follow-up. The ultrasound imaging and arterial measurements used an in-house developed protocol and software designed for longitudinal assessment of atherosclerosis [4–9]. Coefficients of variation using the two baseline ultrasound measurements were 0.43% for CIMT, 12.85% for arterial distensibility and 12.23% for compliance.
Other trial endpoints
Laboratory-based endpoints were determined at baseline and every six months and included measurement of metabolic factors [total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total triglycerides (TG), fasting glucose and insulin, hemoglobin A1c (HbA1c)], hemorheological parameters [RBC aggregation (in autologous plasma), RBC aggregability (in 3% isotonic solution of 70 kDa dextran), ESR, whole blood viscosity from 1 to 1,000 sec–1, plasma viscosity], blood coagulation and fibrinolysis factors [prothrombin time (PT), activated partial thromboplastin time (aPPT), fibrinogen, ristocetin cofactor, factor VIII activity, vWF antigen, tPA antigen, PAI-1, D-dimers, platelet aggregation-adenosine diphosphate (ADP), collagen], inflammatory markers [high sensitivity C-reactive protein (hsCRP), monocyte chemotactic protein-1 (MCP-1), placental growth factor (PGF), interleukin-8 (IL-8), tumor necrosis factor alpha (TNFα), interleukin-10 (IL-10)], cellular adhesion molecules [intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), E-selectin, P-selectin] and monocyte/macrophage cellular activation markers [cluster differentiation 11b (CD11b), CD14, very late antigen-4 (VLA-4, also known as CD49]. See Supplementary Appendix for methods.
Sample size estimation
As there were no human data relating nattokinase to atherosclerosis progression when designing this trial, we used: 1) The reported BP reduction with nattokinase [10]; and, 2) published associations of BP reduction with CIMT progression to estimate sample size for this trial. In the SECURE trial, the average level of systolic BP reduction (approximately 4.5 mmHg) was similar to that shown for nattokinase. In SECURE, the average treated group difference from placebo in CIMT progression was 0.0059 mm/yr [11]. Using the standard deviation (SD) of CIMT rate in clinical trials conducted by our research group of 0.015 mm/yr, a 2-sided alpha error of 0.05 and 80% power, 105 participants per treatment group were required. Inflating the number randomized to consider early dropouts of 5% per year yielded a sample size of 120 participants per group (240 total).
Statistical analysis
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the University of Southern California [12, 13]. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing: 1) An intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and, 4) procedures for data integration and interoperability with external sources.
To evaluate comparability between randomized groups at baseline, treatment arms were compared with respect to demographic variables (age, gender, race/ethnicity, education) and cardiovascular risk factors (smoking history, body mass index (BMI), BP, lipids). Baseline variables were summarized as median (interquartile range, IQR) for continuous variables and frequency (percent) for categorical variables. Baseline levels of each trial outcome variable were also compared between groups. Baseline comparisons were completed for the entire randomized study sample and for the group of participants with baseline and at least one follow-up carotid ultrasound.
Treatment group comparisons on the primary atherosclerosis trial outcomes included all 265 randomized participants. Participants who dropped from the trial prior to the first ultrasound examination at 6 months post-randomization were maintained in the analysis, contributing to the estimate of baseline mean values. Groups were compared on the rate of change in CIMT (and CAS), using linear mixed effects models for longitudinal data. Primary independent variables were randomized treatment group and time on-study (measured as years since randomization), with the randomization stratification variable (dichotomized baseline CIMT) used as a covariate. Random effects terms for the regression intercept and slope (change over time) were specified to allow for individual participant deviations from their group average in baseline CIMT and CIMT rate of change, respectively; an unstructured covariance matrix for the random effects terms was used. A treatment group by time on-study interaction term tested for differences in the CIMT rate by treatment group. A similar mixed effects model analysis was used to test for treatment group differences in changes in CAS (distensibility and compliance).
Comparison of on-trial levels in laboratory and clinical variables across treatment groups used linear mixed effects models. Independent variables included randomized treatment group and indicator variables for follow-up time at which the laboratory measure was obtained; covariates included the CIMT randomization stratification factor and the baseline value of the dependent laboratory variable. The main analysis for each laboratory variable estimated and compared treatment group means over the trial follow-up (i.e., the averaged treatment group mean over visits). Interaction terms of treatment group-by-study time period tested whether treatment group differences varied over the trial follow-up. Normalizing transformations (primarily natural log transformation) were completed for some laboratory measures; group comparisons were evaluated on these transformed variables. IL-8, TNFα and IL-10 were compared using ordinal logistic regression, comparing the groups on quartiles of these measures as no transformations achieved a normal distribution.
The following clinical events were tabulated and compared between treatment groups using Fisher’s exact tests: 1) Major cardiovascular events: Fatal/nonfatal myocardial infarction, sudden coronary death, hospitalization for unstable angina and revascularization procedures (coronary artery bypass graft surgery and percutaneous transluminal coronary angioplasty); 2) major cerebrovascular events: Transient ischemic attack, reversible ischemic neurological deficit, cerebrovascular accident; 3) deep vein thrombosis; 4) pulmonary embolism; 5) incident cancers; and, 6) all-cause mortality.
A two-sided significance level of 0.05 was used for all analyses.
Results
Trial flow
A total of 1189 persons were screened for trial eligibility (Fig. 1), with 332 passing telephone screening and attending in-clinic screening. A total of 281 clinic-screened participants met eligibility criteria and 265 were randomized (132 to nattokinase; 133 to placebo); 16 otherwise eligible individuals chose not to participate for personal reasons. Major reasons for ineligibility were use of ineligible medications (lipid-lowering, aspirin, anti-platelet, anti-coagulant), pre-existing cardiovascular disease or diabetes, bleeding diatheses or tendencies. A total of 234 randomized participants (88% of randomized) completed at least one carotid artery ultrasound follow-up visit (118 nattokinase, 116 placebo). Among the randomized participants the median (IQR) of trial follow-up was 36.1 (IQR 35.7, 36.3) months.
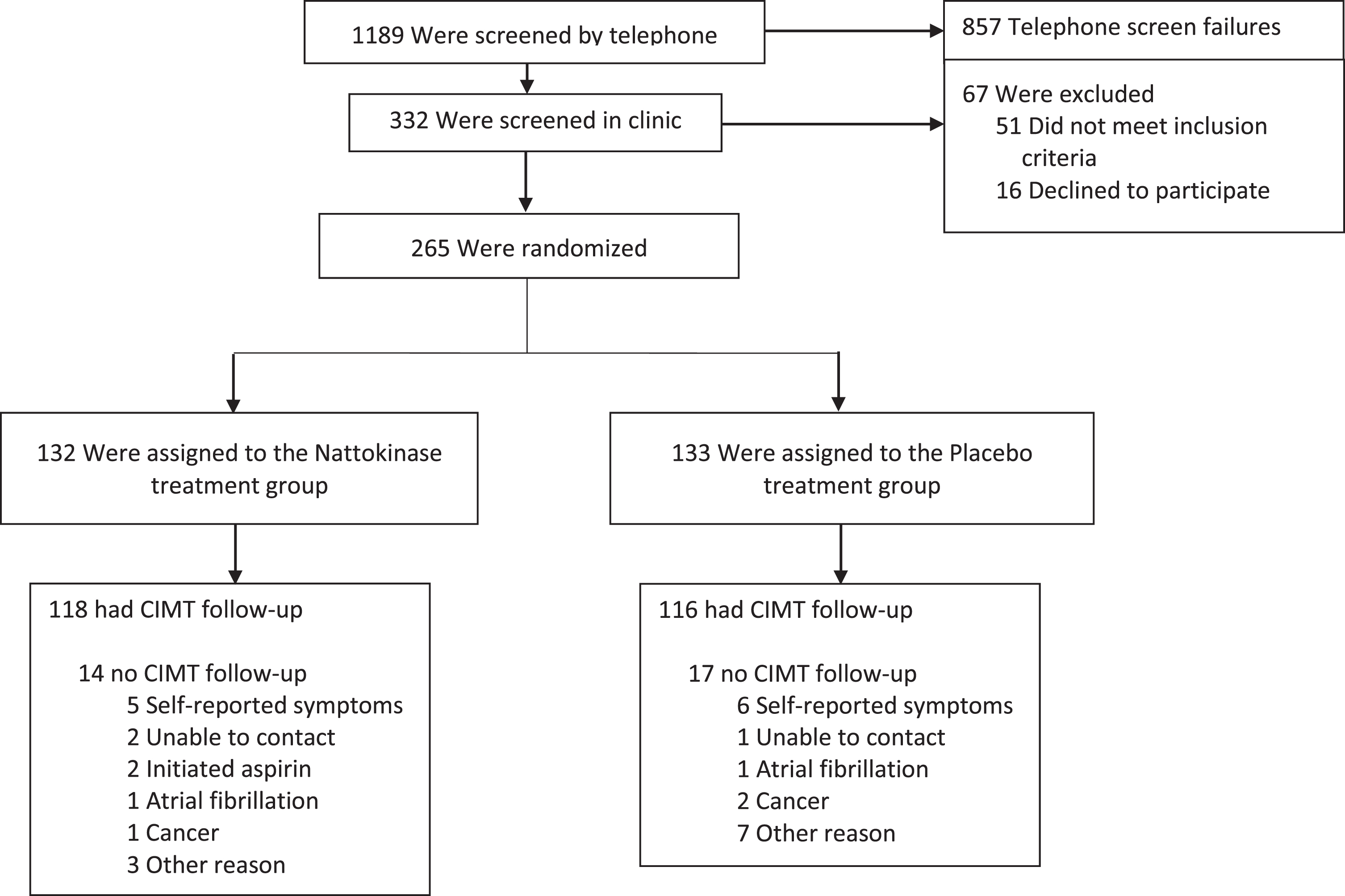
Nattokinase atherothrombotic prevention study Consort diagram. Telephone screen failures (not exclusive): Taking lipid lowering medications, aspirin or anti-platelet medications or anticoagulants (n = 461), cardiovascular disease (n = 107), bleeding diathesis or tendencies (n = 61), diabetes (n = 45), age < 55 years (n = 21), cancer (n = 16), not willing to stop taking soy supplements (n = 10), allergy to soy, soy protein or legumes (n = 6), cirrhosis, liver disease (n = 6), personal reasons (n = 318). Other reasons for no carotid artery intima-media thickness follow-up were the following: Active treatment, no carotid artery intima-media thickness follow-up (N = 3): Work related injury (1), no time (1), not interested in study (1); placebo treatment, no carotid artery intima-media thickness follow-up (N = 7): Personal reasons (3), too busy (1), not interested in study (3).
Characteristics of the NAPS sample by randomized treatment group are provided in Table 1 and Table S1 in the Supplementary Appendix. Table 1 details baseline characteristics among all 265 randomized participants, while Supplementary Table S1 details baseline characteristics in the 234 participants who contributed a baseline and at least one follow-up carotid artery ultrasound assessment for measurement of CIMT and CAS. The two study groups were well-matched on demographic characteristics (age, gender, race, education) and clinical characteristics related to vascular health (including smoking history, BMI, BP and lipid levels). The total sample of 265 randomized participants had a median (IQR) age of 65.3 (60.7, 71.9) years and BMI of 26.5 (23.7, 29.5) kg/m2. The sample was primarily female (62% female, 38% male), white (71% white, 29% non-white) and well-educated (69% reported a bachelor’s degree or higher). Average BP and lipid levels reflected the recruitment of healthy individuals without pre-existing cardiovascular disease or diabetes.
Demographic and baseline characteristics of randomized participants, N = 265
Demographic and baseline characteristics of randomized participants, N = 265
IQR, interquartile range; N, number.
At each clinic visit, participants returned their unused study pills to count the number of pills consumed since the prior clinic visit. Pill compliance was calculated as a percentage of the number of pills that should have been consumed between clinic visits (i.e., number of days between visits). Among the 249 participants who had at least one post-randomization clinic visit, adherence to the study product was excellent, with a median (IQR) percent compliance of 95.8% (91.2, 98.8) in nattokinase and 95.7% (92.3, 98.3) in placebo participants (Wilcoxon rank sum p-value = 0.98).
Subclinical atherosclerosis progression
Results of the linear mixed effects analysis for the primary atherosclerosis outcomes are presented in Table 2. The analysis included the entire sample of 265 randomized participants (1,591 ultrasound assessments). At baseline, the mean arterial compliance was slightly although not significantly higher in the nattokinase compared to placebo group (p = 0.06); CIMT and distensibility were well balanced at baseline. The primary outcomes of annualized rate of change in each measure did not significantly differ between nattokinase and placebo groups. For example, the mean (95% confidence interval, CI) in the rate of CIMT progression was 0.013 (95% CI 0.010, 0.015) mm/year in the nattokinase group, and 0.011 (95% CI 0.009, 0.013) mm/year in the placebo group (p = 0.31). Table S2 in the Supplementary Appendix displays results for treatment group comparisons of CIMT progression by pre-specified subgroups of participants (gender, BMI, systolic BP, age, baseline CIMT and use of BP medications). There was no indication that nattokinase effects on CIMT progression differed by subgroup (all 3-way p-values for interaction ≥0.37), and nattokinase and placebo groups did not differ on CIMT progression within any subgroup (all within-subgroup p > 0.18).
Baseline and progression of carotid artery intima-media thickness and measures of arterial wall stiffness by treatment group (N = 265)
Baseline and progression of carotid artery intima-media thickness and measures of arterial wall stiffness by treatment group (N = 265)
All participants: 133 placebo, 132 nattokinase. Numbers in table are estimated mean (95% confidence interval). CIMT, carotid artery intima-media thickness. One missing observation for measures of stiffness due to missing blood pressure measurement.
Nattokinase did not significantly affect BP compared to placebo (Fig. 2; Table S3 in the Supplementary Appendix). The average on-trial systolic BP (95% CI) was –1.0 (–3.2, 1.2) mmHg lower in nattokinase compared to placebo treated participants (p = 0.36). Average on-trial diastolic BP was –0.4 (–1.9, 1.1) mmHg lower in nattokinase compared to placebo (p = 0.57).
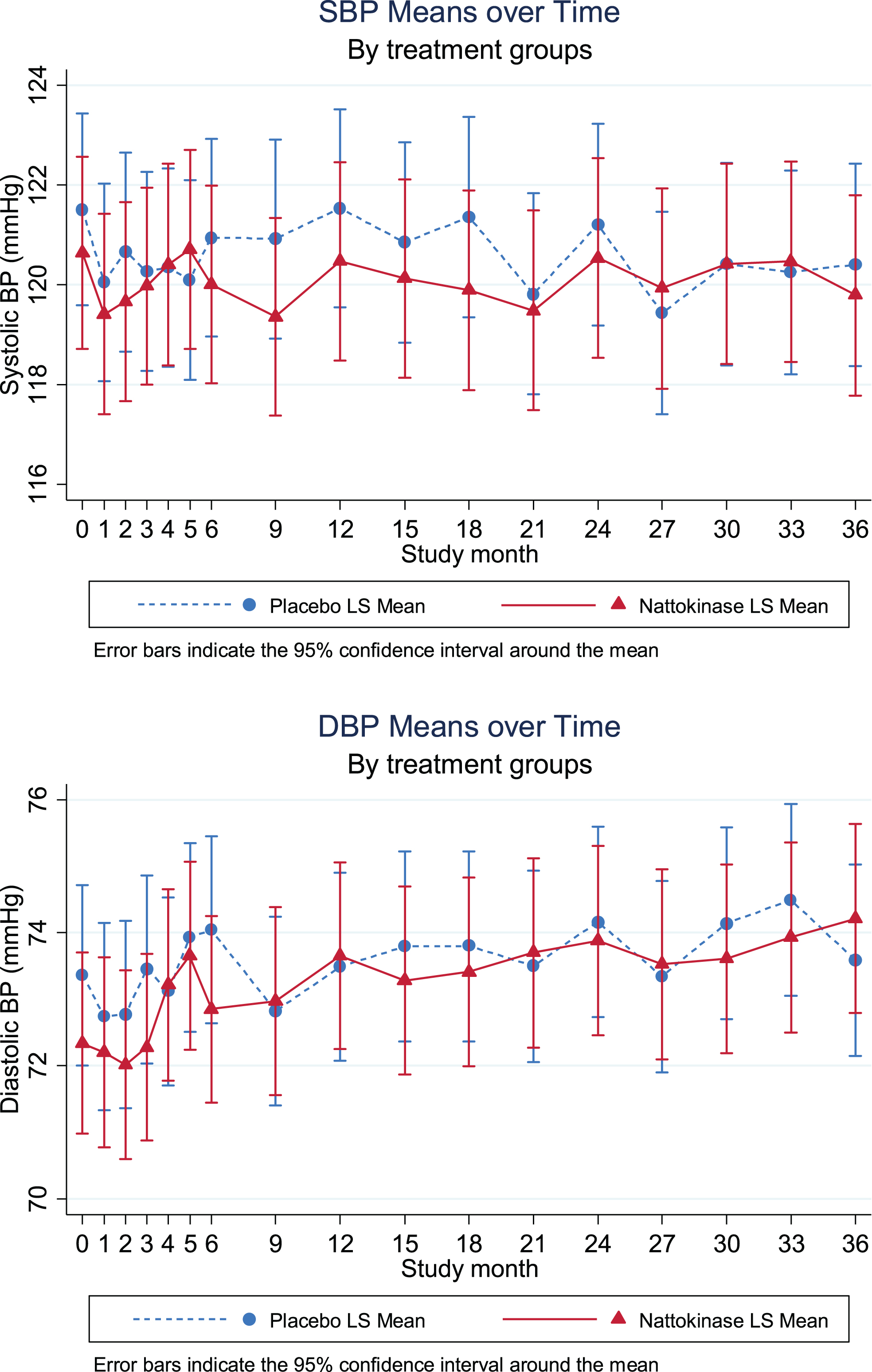
Systolic and diastolic blood pressure means over time by treatment group. Mean systolic and diastolic blood pressure by treatment group and trial visit (study month). Data include 249 total participants with 3,535 trial visits. Error bars represent the 95% confidence interval around the mean.
Treatment group comparisons on laboratory-based trial outcomes are presented in Tables 3–5 and Tables S4–S8 in the Supplementary Appendix. Each table presents the average on-trial measure by treatment group, along with the mean (95% CI) and test for difference between placebo and nattokinase groups. Results are presented by category of measure: metabolic factors (Table 3), blood coagulation and fibrinolysis factors (Table 4), blood rheology (Table 5), whole blood viscosity at native hematocrit and “corrected” to expected value for 0.45 L/L hematocrit at shear rates from 1 sec–1 to 1,000 sec–1 (Table 5 and Table S4 in the Supplementary Appendix), inflammatory markers (Table S5 in the Supplementary Appendix), cellular adhesion molecules (Table S6 in the Supplementary Appendix) and monocyte/macrophage cellular activation markers (Table S7 in the Supplementary Appendix). Other than nominally higher levels of IL-10 in nattokinase compared to placebo (Table S5 in the Supplementary Appendix), there were no treatment group differences in any other laboratory variable. Considering the large number of statistical tests performed, this sole statistically significant finding is likely a result of random chance; control for false discovery rate showed no statistically significant associations. Treatment group comparisons of blood coagulation and fibrinolysis factors and blood rheology after 1 week of randomization are presented in Table S8 in the Supplementary Appendix. Although nattokinase increased RBC aggregability at stasis and decreased tPA antigen (p-values < 0.05) at 1 week on trial, the significance of these treatment group differences at 1 week is unclear as comparisons at all subsequent trial visits for these variables shows no difference between treatment groups (Table 4 and Table 5).
Nattokinase effects on metabolic factors: Average on-trial
Nattokinase effects on metabolic factors: Average on-trial
1Sample size: N1 = Number of participants, N2 = Number of visits. 2Linear mixed effects model, specifying random effect for participant, fixed effects for treatment and assessment time (as indicator variables), and adjustment for randomization stratification factor. 3Log transformed variables: back transformed mean (95% confidence interval) are shown below the mean (standard error) by treatment group. SE, standard error; CI, confidence interval; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, hemoglobin A1c.
Nattokinase effects on blood coagulation and fibrinolysis factors: Average on-trial
1Sample size: N1 = Number of participants, N2 = Number of visits. 2Linear mixed effects model, specifying random effect for participant, fixed effects for treatment and assessment time (as indicator variables), and adjustment for randomization stratification factor. 3Log transformed variables: back transformed mean (95% confidence interval) are shown below the mean (standard error) by treatment group. 4Platelet aggregation. SE, standard error; CI, confidence interval; vWF, von Willebrand factor; tPA, tissue plasminogen activator; PAI-1, plasminogen activator inhibitor-1; ADP, adenosine diphosphate.
Nattokinase effects on blood rheology: Average on-trial
1Sample size: N1 = Number of participants, N2 = Number of visits. 2Linear mixed effects model, specifying random effect for participant, fixed effects for treatment and assessment time (as indicator variables), and adjustment for randomization stratification factor. SE, standard error; CI, confidence interval; M, aggregation at stasis; M1, aggregation at low shear. Whole blood viscosity estimated (i.e., “corrected”) to 0.45 L/L hematocrit via method of Matrai, et al. [22].
Serious adverse events occurred in 15 participants who were randomized to placebo and in 13 participants who were randomized to nattokinase (Table S10 in the Supplementary Appendix). The incidence of major clinical events did not differ (p = 0.84) between placebo and nattokinase participants. One death from pancreatic cancer occurred in a placebo participant. Incidence of cardiovascular events did not differ between groups (p = 1.00). Major cardiovascular events included non-fatal myocardial infarction (2 placebo, 0 nattokinase), chest pain (0 placebo, 2 nattokinase) and coronary artery bypass graft surgery (1 placebo, 1 nattokinase). Other cardiovascular events did not differ between groups; arrhythmias including atrial fibrillation (2 placebo, 1 nattokinase), supraventricular tachycardia (0 placebo, 1 nattokinase) and ventricular extrasystoles (0 placebo, 1 nattokinase), cardiomyopathy (1 placebo, 0 nattokinase), left ventricular failure (1 placebo, 0 nattokinase) and palpitations (1 placebo, 0 nattokinase). Major cerebrovascular events included cerebrovascular accident (1 placebo, 1 nattokinase) and transient ischemic attack (1 placebo, 0 nattokinase) (p = 1.00). Thromboembolic events included deep vein thrombosis (1 placebo, 2 nattokinase) (p = 0.62) and pulmonary embolism (2 placebo, 0 nattokinase) (p = 0.50); deep vein thrombosis and pulmonary embolism combined (3 placebo, 2 nattokinase) (p = 1.00). Malignancies (13 placebo, 16 nattokinase) (p = 0.56) were comprised of basal (10) and squamous (3) cell cancers, malignant skin neoplasm otherwise unspecified (1), breast (2), colon (1), follicular lymphoma (1), lung (1), osteochondroma (1), pancreatic (2), papillary thyroid (1), prostate (5) and rectal (1) cancers. Cancers excluding basal cell (9 placebo, 10 nattokinase) also did not differ between groups (p = 0.82). Incidence of bleeding events did not differ between groups.
Discussion
These NAPS trial results showed a null effect of nattokinase supplementation on the progression of atherosclerosis measured anatomically as arterial wall thickness and measured physiologically as arterial stiffness. Additionally, nattokinase supplementation showed null effects on BP, BMI, lipids, blood rheology, coagulation and fibrinolytic factors, platelet aggregation, inflammatory markers, cellular adhesion molecules and monocyte/macrophage cellular activation.
Although in-vitro and animal studies support a fibrinolytic and thrombolytic potential for nattokinase, less than one-dozen human studies have been conducted. Nattokinase supplementation has been reported to reduce coagulation factors in humans, but these limited studies have been of short duration (2 to 8 weeks), small sample size, single-dose or open label in design with changes mostly occurring within the normal range [14–17]. After a median treatment of 3 years, nattokinase supplementation had no detectable effect on coagulation factors, fibrinolytic factors and platelet aggregation relative to placebo in NAPS. Additionally, at no time point, including early time points of 1 week and 1, 3, and 6 months post-randomization, did nattokinase supplementation have a detectable treatment effect on any coagulation factor, fibrinolytic factor or platelet aggregation relative to placebo.
In a randomized, double-blinded, placebo-controlled trial of 86 participants with mean BP of 145/95 mmHg at baseline, nattokinase was reported to reduce on average systolic BP by 5.55 mmHg and diastolic BP by 2.84 mmHg relative to placebo after 8 weeks of treatment (10). In NAPS, BP was essentially no different between the placebo and nattokinase supplementation treatment groups at all visits. The mean BP at baseline in NAPS was 120/70 mmHg and may account for the difference in BP effects of nattokinase across trials. A subgroup analysis among 24 NAPS participants (with 300 on-trial blood pressure measurements) with baseline blood pressure greater than 120/80 showed on-trial mean systolic and diastolic blood pressures that were 3.7 mmHg (95% CI –9.5–2.1; p = 0.21) and 2.1 mmHg (95% CI –6.6–2.4; p = 0.37) lower in nattokinase compared to placebo participants, respectively.
Although femoral arterial wall thickness was shown to be reduced with nattokinase in Sprague-Dawley rats following non-mechanical arterial wall intimal denudation, no mechanism of action for the reduction in arterial wall thickness was identified [18]. In NAPS, the null effect of nattokinase supplementation on major factors that drive arterial wall thickness and stiffness in humans is consistent with the null effects of nattokinase supplementation on atherosclerosis progression.
Natto intake was significantly associated with a decreased risk of stroke and ischemic heart disease mortality in a prospective community-based cohort of 29,079 Japanese men and women [19]. However, the findings of association may be biased since this community-based study was not a randomized trial. Although nattokinase is the major active component of natto, other fibrinolytic constituents such as dipicolinic acid are present in natto and isolation of a single pure component from natto may not be as effective in reducing atherosclerosis compared to the combination of the individual constituents.
Generalizing results
The results from NAPS may not be generalizable to the population at large. NAPS was a trial conducted in healthy men and women selected without pre-existing cardiovascular disease or diabetes. The inclusion criteria resulted in a healthy cohort of participants with a low cardiovascular risk. It is feasible that higher cardiovascular risk may be required to determine potential preventive effects of nattokinase and to detect treatment effects on intermediary markers.
Limitation of study
Although the selection of the nattokinase dose used in NAPS was based on the most commonly studied dosage reported in the literature, a limitation of this study includes use of a single dose of nattokinase supplementation. Consistent with the literature concerning natto and nattokinase, no major adverse effects of nattokinase supplementation were reported with the dosage used in NAPS over the mean treatment period of 3 years [20]. However, bleeding risk with nattokinase supplementation has been reported when taken concomitantly with other anti-platelet and anti-coagulant agents [21]. Participants using antiplatelet and anticoagulant agents were excluded from the NAPS trial. Higher dosages of nattokinase supplementation, natto itself or an isolate of all the active constituents of natto, including vitamin K2 and dipicolinic acid may be required to demonstrate efficacy in reducing atherosclerosis progression in humans.
Conclusion
In conclusion, in this randomized, double-blinded, placebo-controlled trial of healthy men and women, 3 years of intervention with nattokinase supplementation had a null effect on subclinical atherosclerosis progression that was consistent with the null effect on major risk factors that drive atherosclerosis progression as well as a null effect on cognitive aging.
Footnotes
Acknowledgments
The authors thank the Nattokinase Atherosclerosis Prevention Study participants for their commitment to the Nattokinase Atherosclerosis Prevention Study as well as the external data, safety and monitoring board for their oversight, guidance, advice and expertise.
Conflicts of interest
The authors do not have conflicts of interest related to the submitted work. The funding sources had no role in study design, collection, analysis, interpretation or decision to submit this manuscript. The authors have full access to data generated from the Nattokinase Atherosclerosis Prevention Study and the corresponding author had final responsibility for the decision to submit the work for publication.
Funding
The Nattokinase Atherosclerosis Prevention Study was funded by the Helen Diller Family Foundation. Jarrow Formulas manufactured and donated the active and placebo capsules. Japan Bio Life Sciences donated the ingredient used in the active capsules. REDCap is supported by UL1TR001855 and UL1TR000130 from the National Center for Advancing Translation Science (NCATS) of the National Institutes of Health.