
Abstract
BACKGROUND:
The aim was to retrospectively analyze the ultrasonographic and clinical characteristics of focal inflammatory masses and malignant masses of salivary gland by using B-mode ultrasound (US) and contrast-enhanced ultrasound (CEUS) for differential analysis.
METHODS:
The features of US and CEUS were retrospectively analyzed for 19 cases of focal salivary inflammatory masses and 45 cases of malignant salivary masses. All cases were confirmed by pathohistological examination.
RESULTS:
On B-mode US, the incidence of expansive growth patterns of malignant salivary masses (44.4%, 20/45) was significantly higher than that of focal salivary inflammatory masses (15.8%, 3/19) (p = 0.029). The rate of lymphadenopathy surrounding salivary glands of malignant salivary masses (42.2%, 19/45) was significantly higher than that of focal salivary inflammatory masses (15.8%, 3/19) (p = 0.042). On CEUS, clear enhancement margins were more common in malignant salivary masses (44.4%, 20/45) compared to focal salivary inflammatory masses (15.8%, 3/19) (p = 0.029); Rapid washout was more common in malignant salivary masses (82.2%, 37/45) than focal salivary inflammatory masses (31.6%, 6/19) (p < 0.001). Rapid washout on CEUS and craniocaudal diameter were independent predictive factors in differentiating salivary inflammatory masses and malignant masses according to binary logistic regression analysis. US and CEUS achieved a sensitivity of 80.0%, a specificity of 78.9% and an accuracy of 80.0% for discrimination between salivary inflammatory masses and malignant masses.
CONCLUSION:
Therefore, a multimodal ultrasonographic pathway combining clinical manifestations, B-mode US and CEUS was needed to differentiate between salivary focal inflammatory masses and malignancies to avoid unnecessary biopsies.
Introduction
B-mode US and color Doppler flow imaging (CDFI) are useful in differentiating benign and malignant salivary masses [1–5]. US can provide detailed morphological features of the salivary masses such as size, shape, margin and echogenicity, while CDFI can display the vascularity in the masses. Contrast-enhanced ultrasound (CEUS) can easily and effectively provide an accurate depiction of micro-vascularity by using microbubble-based contrast agents that has widely been used in dynamic evaluation of microvascularization in hepatocellular carcinoma [6, 7], which also plays an important role in identifying benign and malignant masses in the salivary gland [1, 8–10]. Previous studies have concluded that unclear delineation of the gland, inhomogeneous structure, presence of cervical lymphadenopathy, and inhomogeneous vascularization are strong criteria for the diagnosis of malignancy. While clear delineation, moderately inhomogeneous structure, lack of cervical lymphadenopathy, and homogeneous vascularity are the criteria for the diagnosis of benign masses [1]. Some studies classified CEUS imaging of the salivary gland lesions into three types according to the morphologic and distribution features of micro-vascularity: type 1 of diffuse homogeneous enhancement and type 3 of no enhancement and iso-enhancement are suggestive of benign lesions, while type 2 of heterogeneous enhancement with ill-defined margin indicates suspicious malignancy [8]. Area under the time-intensity curve (AUC) and mean transit time (MTT) showed significantly higher values for malignant parotid gland tumors in CEUS quantitative analysis [10]. However, when salivary inflammatory diseases present with focal or nodular lesions that appear as a discrete, painless mass, it becomes difficult to differentiate salivary focal inflammatory masses from salivary malignant masses because with inflammation, the edematous blurred lesional borders and diffuse involvement of the salivary gland mimic malignant tumor in radiological assessment [2, 11–17]. To date, there are few reports about the differential diagnosis of focal salivary inflammatory masses and malignant salivary masses [16]. CT and MRI techniques can gauge the extent and invasion of the tumor, which can be additionally used for diagnosis [18, 19]. Irregular tumor margins or invasion into adjacent structures on CT suggests malignancy [20]. Contrast-enhanced CT is particularly useful when there is an associated abscess and Sjögren’s syndrome [14]. Low signal intensity (SI) on T2-weighted images and postcontrast ill-defined margins of parotid tumors are highly suggestive of malignancy, while inflammatory diseases display high SI on T2-weighted images, though chronic stages may have a somewhat lower SI [17]. 18F-FDG PET/CT detected surveillance for recurrent disease or assessed distant metastases and restaging of malignant salivary gland tumors with high sensitivity and specificity [21, 22]. Moreover, an accurate diagnosis is essential for clinical management. Therefore, this study analyzed the differences in sonographic features and clinical manifestations between the two masses for differential diagnosis. By comparing the features of B-mode US and CEUS in 19 cases of focal salivary inflammatory masses and 45 cases of malignant salivary masses, this study aimed to summarize the differences between these two diseases and help avoid unnecessary medical interventions.
Patients and methods
Study design
This retrospective study was approved by the Human Research Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (No. 2021-0242) and was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. Patients have provided informed consent for publication of the study.
From September 2018 to July 2020, 109 patients with unilateral salivary solid masses who underwent core needle biopsy or surgery were enrolled in this study. The inclusion criterions were as follows: informed consent was obtained; unilateral parotid or submandibular gland solid masses were detected by B-mode US; malignancy or inflammation was confirmed with pathological examination. The exclusion criteria were the followings: patients refused to sign the informed consent; diffuse performance of salivary glands or bilateral nodules of salivary glands were detected by B-mode US; benign masses confirmed by pathology. 39 cases of benign salivary tumors confirmed by pathology and 6 cases of diffuse performance of salivary glands on US were excluded. A total of 64 cases were analyzed which included 19 cases of focal salivary inflammatory masses (13 cases of parotid gland masses and 6 cases of submandibular gland masses) and 45 cases of malignant salivary masses (37 cases of parotid gland masses and 8 cases of submandibular gland masses). All cases were studied using US and CEUS along with the patients’ clinical presentation. Clinical parameters included time interval (time from symptom onset to initial medical evaluation), erythema, warmth, pain, numbness, lesion size increase in less than one month and previous history of malignancy.
B-mode US and CEUS
A Mindray Resona 7 ultrasound diagnostic instrument (Mindray, Shen-zhen, China) equipped with a L11-3 probe was used for B-mode US and CEUS examination. Frequency of the probe ranged from 4–15MHz. The salivary gland was initially scanned with B-mode US to identify the mass and number of masses. The largest mass was then selected for analysis. The size (the anteroposterior diameter and craniocaudal diameter), shape, orientation, boundary, margin, internal and posterior echo, cystic change, calcifications, peripheral lymphadenopathy around tumor side of the gland (locoregional lymph nodes of the neck zone I and II, and lymph nodes within the salivary gland) and vascularity of the mass were then recorded. This procedure was followed by real-time CEUS imaging using a low mechanical index ranging between 0.06 and 0.08. Then, 2.4 mL of the microbubble contrast agent (SonoVue, Bracco, Italy) was administered via the antecubital vein and followed by a 5 mL of 0.9% sodium chloride as a flush. Images were recorded with a clip function for 120 seconds after administration of the contrast agent while the probe was stabilized with minimal pressure. A qualitative evaluation of the mass enhancement pattern was then performed for each mass.
Imaging analysis
US images and CEUS dynamic images of each case were retrospectively analyzed by two radiologists with 15 years and 10 years of experience in salivary US. The evaluation was done before the pathohistological result was obtained. They blinded with each other at the first time and they arrived at a consensus by joint review and discussion of disagreements at the second time. Observation parameters of the masses included: (1) number of masses: single or multiple; (2) mass size: anteroposterior diameter and craniocaudal diameter; (3) shape: regular or irregular; (4) orientation: parallel growth (the long axis of the mass parallels to the skin line) or expansive growth (the long axis of the mass not parallel to the skin line); (5) boundary: clear or not clear; (6) margin: circumscribed or not circumscribed (indistinct, angular, microlobulated, spiculated, etc.); (7) internal echo: homogeneous or heterogeneous (honeycomb, no echo); (8) posterior features: enhancement, shadowing, no posterior features; (9) cystic change in the mass: yes or no; (10) calcifications: yes or no; (11) peripheral lymphadenopathy (irregular cortical thickness greater than 3 mm, longest/shortest axes ratio < 2 or absence of fatty hilum): yes or no; (12) vascularity: grade 0, grade 1, grade II, grade III. The classification of vascularity is based on Adler’s system [23]: grade 0 describes a total absence of blood flow within the mass; grade I describes a small amount of blood flow, with one or two spots of thin rod-shaped tumor vessels; grade II describes medium blood flow with three to four punctate blood vessels or a longer vessel which penetrates into the mass. The length of the vessel can approach or exceed the radius of the mass; grade III describes copious vascularity, with more than five punctate blood vessels or two longer blood vessels. The enhancement pattern of CEUS was qualitatively analyzed from the following aspects: (1) enhancement order: centripetal enhancement, centrifugal or diffuse enhancement; (2) unenhanced area within the mass: yes or no; (3) enhancement degree (compared with the normal gland): hyper-, hypo- or isoenhancement; (4) peripheral enhancement (high brightness continuous enhancement around the mass during wash-in process): yes or no; (5) enhancement margins: clear margins (greater than 50% of enhanced areas with well-defined margins) or blurred margins (less than 50% of enhanced areas with well-defined margins or ill-defined margins) [1]; (6) size expansion after enhancement: yes or no; (7) rapid washout/early washout of the lesion (contrast agent washed out from the mass within 30 seconds from the time of injection): yes or no.
Statistical analysis
The data was analyzed by using SPSS 17.0 statistical software. Quantitative data was expressed as the mean with standard deviations (anteroposterior diameter, craniocaudal diameter) or median with interquartile range (time interval). Count data comparison was performed using a χ2 test and continuous correction χ2 test (when the sample content was > 40, 1≤expected frequency < 5); the quantitative data was compared using an independent T-test; the rank variable and non-normal distributed variable were compared using Mann-Whitney rank-sum test. Binary logistic regression was used to identify the independent risk factors for salivary inflammatory masses and malignant masses. Factors that were significantly less than 0.1 in the univariate analysis were included in the multivariate regression analysis. Probability values of p < 0.05 were considered to be statistically significant.
Results
Clinical manifestations
The age of the 19 patients with focal salivary inflammatory masses ranged from 22 to 84 years old, with an average age of 55.21±15.88 years old. The age of the 45 patients with malignant salivary masses ranged from 26 to 92 years old, with an average age of 61.38±15.07 years old.
The proportion of malignant salivary masses with a previous malignancy history (33.3%, 15/45) was higher than that of focal salivary inflammatory masses (5.3%, 1/19) (p = 0.040). There were no statistically significant differences in age, gender, time interval from the initial onset of symptoms to the first medical evaluation, and related symptoms between the two diseases (p = 0.146, 0.621, 0.087, 0.338 respectively). The clinical manifestations between the two groups were compared and summarized in Table 1.
Clinical manifestations of focal inflammatory masses and malignant masses of salivary gland
Clinical manifestations of focal inflammatory masses and malignant masses of salivary gland
*p < 0.05. Continuous correction χ2 test; ‡: Mann-Whitney rank-sum test; †: independent T-test; §: χ2 test.
The 19 cases of focal salivary masses included 11 cases of chronic sialadenitis of the salivary gland (Fig. 1), four cases of chronic granulomatous sialadenitis (Fig. 2) and four cases of Mikulicz disease. 45 cases of malignant salivary masses included eight cases of lymphoma (Fig. 3), six cases of metastatic carcinoma, six cases of adenoid cystic carcinoma (Fig. 4), five cases of malignant tumors of salivary origin (pathological results from core needle biopsy failed to clarify the specific pathological type), four cases of salivary ductal carcinoma, four cases of squamous cell carcinoma, four cases of poorly differentiated carcinoma, two cases of acinar cell carcinoma, two cases of mucoepidermoid carcinoma, one case of adenocarcinoma, one case of eosinophilic carcinoma, one case of carcinoma in pleomorphic adenoma, and one case of lymphoepithelial carcinoma. The detailed pathological results were shown in Table 2.
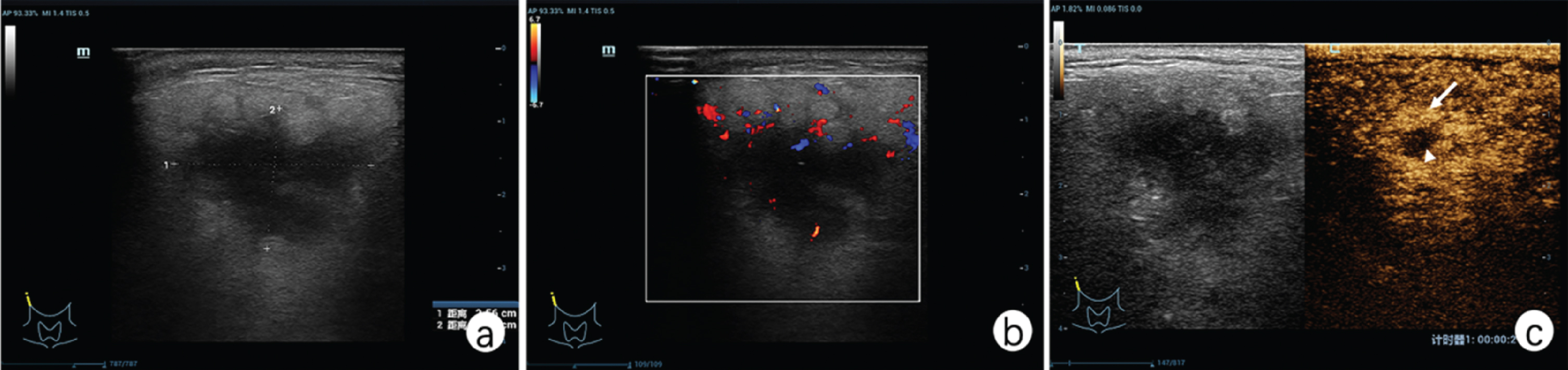
Chronic sialadenitis of the right parotid gland. Patient was a 68-year-old male, presenting with swelling in the right ear for 2 weeks. a) Ultrasound showed an irregular mass (2.56*1.91 cm) with spiculate margin and parallel growth. b) Color Doppler image showed grade I intralesional vascularity.
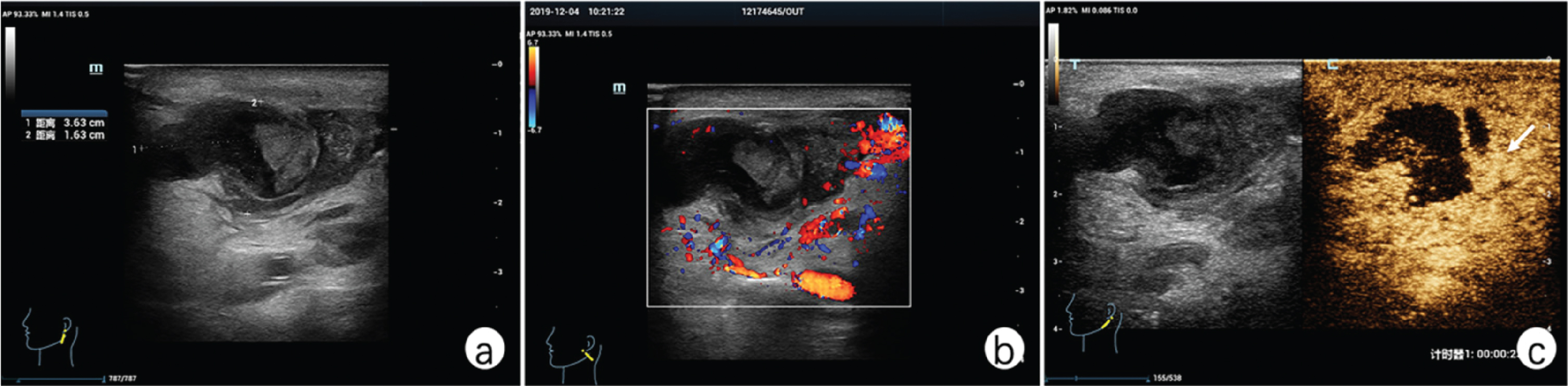
Chronic granulomatous sialadenitis of the left parotid gland. Patient was an 84-year-old male, presenting with a left parotid mass for 1 week. a) Ultrasound showed the mass (3.63*1.63 cm) with an irregular shape, distinct margin, posterior enhancement, a sonolucent fluid area within the mass, and parallel growth. b) Color Doppler showed grade 0 intralesional vascularity. c) CEUS showed peripheral hyperenhancement with unclear enhancement margin around the mass (white arrow) and there was no rapid washout in first 30 seconds.

Diffuse large B cell lymphoma of right parotid gland. A 58 years old male patient, found painless masses in the right parotid gland with mass size increasing rapidly for more than one month. a) Ultrasound showed ill-defined mass (3.0*2.7 cm) with indistinct margin, posterior echo enhancement and expansive growth. b and c) CEUS showed diffuse rapid hyperenhancement with unclear enhancement margin and rapid washout in 20 seconds (white arrows).

Adenoid cystic carcinoma of left parotid gland. 48 years old female reported discomfort in the left parotid area for more than half a year. a) Ultrasound imaging showed a well-defined mass (1.2*1.4 cm) with circumscribed margin, posterior echo enhancement and expansive growth. b and c) CEUS showed centrifugal rapid hyperenhancement with clear enhancement margin and rapid washout in 23 seconds (white arrows).
Pathological results of focal inflammatory masses and malignant masses of salivary gland
B-mode US characteristics of the 19 focal salivary inflammatory masses and 45 malignant salivary masses were compared and summarized in Table 3. The average craniocaudal diameter of malignant salivary masses (26.63±15.65) mm was significantly larger than that of focal salivary inflammatory masses (14.92±5.57) mm (p < 0.001) (Table 1). The incidence of expansive growth pattern of malignant salivary masses (44.4%, 20/45) was significantly higher than that of focal salivary inflammatory masses (15.8%, 3/19) (p = 0.029). The rate of lymphadenopathy around the salivary gland of malignant salivary masses (42.2%, 19/45) was significantly higher than that of focal salivary inflammatory masses (15.8%, 3/19) (p = 0.042). There were no significant differences in characteristics such as mass shape, boundary, margin, internal echo, posterior echo, cystic change, calcifications or vascularity between the two mass types (p > 0.05).
Sonographic characteristics of focal inflammatory masses and malignant masses of salivary gland
Sonographic characteristics of focal inflammatory masses and malignant masses of salivary gland
*p < 0.05. ¶: Continuous correction χ2 test; ‡: Mann-Whitney rank-sum test; †: independent T-test; §: χ2 test.
This study found that focal salivary inflammatory masses typically displayed hyperenhancement (78.9%, 15/19). However, hypo- or isoenhancement can also be seen in some cases (21.1%, 4/19). While a large majority of malignant salivary masses showed hyperenhancement (93.3%, 42/45), few cases showed hypoenhancement (6.7%, 3/45). A comparative analysis of qualitative features of CEUS findings from focal salivary inflammatory masses and malignant salivary masses were shown in Table 4. The result showed that the rate of clear enhancement margins in malignant salivary masses (44.4%, 20/45) was significantly higher than that of focal salivary inflammatory masses (15.8%, 3/19) (p = 0.029). The incidence of contrast agents demonstrating a rapid washout pattern in malignant salivary masses (82.2%, 37/45) was significantly higher than that of focal salivary inflammatory masses (31.6%, 6/19) (p = 0.000). However, there were no significant differences in the enhancement order, unenhanced area within the mass, enhancement degree, size expansion after enhancement and peripheral enhancements between focal salivary inflammatory masses and malignant salivary masses (p > 0.05).
Contrast-enhanced ultrasound characteristics of focal inflammatory masses and malignant masses of salivary gland
Contrast-enhanced ultrasound characteristics of focal inflammatory masses and malignant masses of salivary gland
*p < 0.05. ¶: continuous correction χ2 test; ‡: Mann-Whitney rank-sum test; †: independent T-test; §: χ2 test.
The independent risk factors selected for univariate analysis were orientation, lymphadenopathy, enhancement margin, rapid washout, craniocaudal diameter and previous tumor history. All these factors were entered for logistic regression analysis, and two variables were identified as the significant factors in the final step: rapid washout and craniocaudal diameter. Rapid washout on CEUS and craniocaudal diameter were meaningful independent predictive factors in differentiating salivary inflammatory masses and malignant masses (Table 5).
Logistic regression analysis of risk factors for focal inflammatory masses and malignant masses
Logistic regression analysis of risk factors for focal inflammatory masses and malignant masses
*p < 0.05.
Descriptive statistical analysis (sensitivity, specificity, accuracy) of the masses revealed that US and CEUS achieved in our study a sensitivity of 80.0%, a specificity of 78.9% and an accuracy of 80.0% for discrimination between salivary inflammatory masses and malignant masses (Table 6).
Assessment of focal inflammation masses and malignant masses of salivary gland
Assessment of focal inflammation masses and malignant masses of salivary gland
To our knowledge, there was no study to investigate the differential diagnosis of salivary inflammatory masses and malignant masses. With histopathologic examination as a reference standard in our study, some parameters on US and CEUS were meaningful indicators to distinguish focal salivary inflammatory and malignant masses, including craniocaudal diameter, orientation of masses and lymphadenopathy surrounding the salivary gland on US; mass enhancement margin and rapid washout pattern on CEUS. Rapid washout on CEUS and craniocaudal diameter were meaningful independent predictive factors in differentiating salivary inflammatory masses and malignant masses based on the binary logistic regression analysis. US and CEUS combination showed good diagnostic performance with sensitivity of 80.0%, specificity of 78.9% and accuracy of 80.0% for discrimination between salivary inflammatory masses and malignant masses.
Causes of sialadenitis include acute or chronic infective, obstructive, immunoglobulin G4-related sialadenitis (IgG4-RS), lympho-epithelial, granulomatous and post-treatment sialadenitis [14]. Chronic sialadenitis of the salivary gland is a common clinical condition characterized by recurrent, diffuse or localized salivary enlargement, usually with painful swelling, with or without discharge of pus [11, 24]. Most cases of chronic sialadenitis is the result from repeated infections with subsequent glandular destruction [11]. According to the scope of the inflammatory mass, it may manifest as focal or diffuse lesions. Salivary focal inflammatory diseases have many similarities in clinical and imaging manifestations with malignant masses of the salivary gland such as discrete and painless masses with blurred margin, irregular shape and hypervascularity [2, 11–16], it remains difficult to differentiate between the two clinically. Mikulicz disease is now considered to be a part of the spectrum of IgG4-related disease which is frequently associated with elevated serum IgG4 levels to have effective response to corticosteroid therapy. Mikulicz disease often presents as a hypoechoic, poorly demarcated mass [14].
On B-mode US, malignant salivary tumors usually show hypoechoic and heterogeneous characteristics with an irregular shape, instinct margins, infiltration of surrounding soft tissues, and pathological lymphadenopathy [1–3]. Our study found that there were no significant differences in characteristics such as mass shape, boundary, margin, internal echo, posterior echo, cystic change, calcifications or vascularity between the two mass types. However, expansive growth of malignant masses was more common compared with that of focal salivary inflammatory masses with statistical significance. It was suspected that the malignant salivary masses often grow and invade along anatomical structures such as vessels or pores, which can then extend into their adjacent tissue space, while the extent of inflammation is relatively limited in the focal salivary inflammatory masses, and causes thickening and edema of the surrounding soft tissues. These changes appear as hypoechoic streaky bands in the surrounding fascia and parallel in orientation [25, 26]. Meanwhile, this study also showed that the presence of large cervical lymphadenopathy in malignant masses (19/45, 42.2%) was significantly more common than that of inflammatory masses (3/19, 15.8%). Inflammatory disease usually causes a reactive enlargement of the lymph node, which was different from lymph node mediated metastasis in malignant masses [26–28]. CEUS can help differentiate the two by their centripetal or centrifugal enhancement patterns.
CEUS has important value in distinguishing focal inflammatory masses from malignant masses of the salivary gland. Although benign and malignant masses of the salivary gland have been identified on US and CEUS in some previous reports [1, 29], literature reports regarding the differential diagnosis of focal salivary inflammatory masses and malignant salivary masses are rare. In this study, some CEUS characteristics were common in both focal salivary inflammatory masses and malignant salivary masses, such as centripetal enhancement, hyper-enhanced areas, unenhanced area, or lack of peripheral enhancement, and there were no significant differences between the two. Our study found that clear enhancement margins were more common in malignant salivary masses (44.4%, 20/45) on CEUS compared with focal salivary inflammatory masses (15.8%, 3/19). Factors such as inflammatory responses around the inflammatory masses and edema of the surrounding soft tissue can lead to unclear margins. On the contrary, some well-differentiated malignant tumors or early stages of malignant tumors often appear similar to benign tumors with clear enhancement margins [2, 26]. Rapid washout pattern on CEUS can be found in 82.2% cases of malignant salivary masses (37/45), but only in 31.6% cases of focal salivary inflammatory masses (6/19). The abnormal and chaotic vessel structure with irregular and disrupted vessels in cancer tissue leads to formation of arteriovenous fistulas, which causes a hypervascularized vessel network and rapid washout [10]. Inflammatory masses in general show slow washout as a result of their regular vessel structure [1, 7].
The performance of US in diagnosis of salivary masses in previous studies was not satisfactory, because diagnostic sensitivity and specificity were not well compromised. It is important to select independent risk factors and diagnose salivary masses using multimode method. The logistic regression analysis for US combined with CEUS and clinical manifestations provided a more objective and accurate method for the differentiation of salivary masses. And finally, rapid washout on CEUS and craniocaudal diameter were meaningful independent predictive factors in differentiating salivary inflammatory masses and malignant masses.
There are certain limitations to this study. Firstly, this study is a retrospective single-center study and there is confounding bias in the evaluation of US and CEUS parameters. Secondly, some parameters such as calcifications in the mass (malignant masses vs focal inflammatory masses, 22.2% (10/45) vs 0% (0/19), p = 0.063) had certain clinical value, but did not reach the test threshold of 0.05, which may be related to insufficient sample size in this study. The sample size needs to be further expanded for more conclusive results. Lastly, only qualitative parameters were used in B-mode US and CEUS without quantitative indicators such as CEUS time-intensity curve parameters, or semi-quantitative analysis with ultrasound elastography. Follow-up studies could benefit from applying more novel technologies and quantitative parameters.
Conclusions
In conclusion, a multimodal ultrasonographical pathway combining clinical manifestations, B-mode US and CEUS was needed to differentiate between salivary focal inflammatory masses and malignancies to avoid unnecessary interventions. The craniocaudal diameter and orientation of masses on US are meaningful indicators to distinguish focal salivary inflammatory and malignant masses, as well as lymphadenopathy surrounding the salivary gland. The mass enhancement margin and rapid washout pattern on CEUS are important features to aid in the diagnosis of salivary masses. Additionally, previous tumor history also provides important clues for differential diagnosis. Rapid washout on CEUS and craniocaudal diameter were meaningful independent predictive factors in differentiating salivary inflammatory masses and malignant masses. Radiologists should closely combine clinical and imaging data to improve the diagnostic accuracy of salivary masses.
Footnotes
Acknowledgments
We thank Yik Ning Wong for language support for this study.
Funding
This work was supported by Key Research and Development Program of Zhejiang Province (2019C03077), National Natural Science Foundation of China (82030048, 81901871, 82001818), Natural Science Foundation of Zhejiang Province (LQ19H180004, 2019C03077, LQ20H180009, LQ20H180011, LQ21H180007).
Conflicts of interest
The authors have no conflicts of interest to declare.