
Abstract
BACKGROUND:
Negative pressure wound therapy (NPWT) has been established over years for treatment of chronic and complex wounds.
OBJECTIVE:
Aim of this study was to investigate the effect NPWT on the microperfusion.
METHODS:
Prospective single centre analysis of patients treated with NPWT due to acute (ACUTE) wounds after fasciotomy or patients with chronic wounds (CHRONIC) due to a chronic limb threatening ischemia was performed. NPWT was conducted through a three days sequence with a negative pressure of –120 mmHg. Before after and during the entire period of therapy the microperfusion was assessed (O2C™, LEA Medizintechnik).
RESULTS:
Comparison of the perfusion values of 28 patients (CHRONIC/ACUTE 5/23, women/men 8/20) before and after the NPWT sequence showed a non-significant improvement in the CHRONIC group (supine position: p = 0.144, elevated position p = 0.068) and a significant decrease in the ACUTE group (supine position p = 0.012, elevated position p = 0.034). This effect could also been demonstrated during the NPWT over time (CHRONIC: supine position: p = 0.320, elevated position: p = 0.053, ACUTE: supine position: p = 0.021, elevated position: p = 0.012).
CONCLUSION:
Microperfusion measurements showed alterations and differences in wound bed perfusion of acute and chronic wounds; acute wounds tended to a decrease of blood flow, whereas this effect was not seen in chronic wounds in peripheral artery disease.
Introduction
Negative pressure wound therapy (NPWT) has been established over years for treatment of chronic and complex wounds [1]. Its clinical effects mainly include reduction of edema and promotion of granulation at the wound‘s bed, whereas the exact alterations on the level of the microcirculation and their influence on the healing process remain under debate [2, 3].
Pilot studies could demonstrate an improved wound healing rate and wound depth after NPWT compared to conventional dressings, but failed to show significant differences in terms of tissue perfusion in vascular compromised patient sample [4]. With respect to tissue perfusion changes during NPWT literature reports inconclusive results with increased or diminished perfusion and the value of laser Doppler for measurement of microperfusion alteration itself is questioned [5, 6].
However, despite of a considerable number of published literature, evidence of benefit by NPWT remains low due to high risk of bias in existing randomized trials, as stated in a recent meta-analysis [7]. In addition, present studies predominantly analyzed point-to-point tissue perfusion before and after NPWT [8, 9], whereas the direct zone of interest is naturally covered by the NPWT dressing (when the suction is applied) and is therefore under suction inaccessible to most measurement tools. To this date, this allowed mainly evaluation of surrounding tissue under ongoing suction [5, 10]. In order to clarify perfusion patterns during ongoing NPWT, we performed a prospective evaluation of wound bed microperfusion directly below the NPWT dressing with newly developed laser Doppler probes under suction; to address different wound aetiology we separated between acute wounds and chronic wounds in vascular compromised patients.
Patients and methods
Patients
A prospective single centre analysis of patients treated with NPWT due to acute wounds after fasciotomy or patients with chronic wounds due to a chronic limb threatening ischemia was performed. All patients between the 1st April 2017 and the 31st January 2019 treated with NPWT were screened for study inclusion. The study was conducted in congruence with the declaration of Helsinki, adhered to the STROBE guidelines and was further approved by the local ethics committee (number 157_17 B) [11]. Written informed consent was obtained from all patients.
Study design
In this prospective study, the influence of NPWT on two different types of wound beds was assessed. Therefore, two different groups were investigated: Patients with chronic wounds of the lower leg due to a chronic limb threatening ischemia (group: CHRONIC) and patients with wounds of the lower leg due to a fasciotomy after compartment’s syndrome (group: ACUTE). In the ACUTE group a coexisting peripheral arterial disease was excluded by Doppler measurements (ankle-brachial index > 0.9). All wounds were conditioned by a three days sequence of NPWT (continuous therapy of negative pressure of –120 mmHg) before they either were finally closed by a secondary suture or split thickness skin graft.
After the wound debridement, the probes from the O2C™ (LEA Medizintechnik, Giessen, Germany) device were placed directly on the wound bed under the foam for the NPWT (compare Fig. 1 A and B). Perfusion measurements were then performed in the supine position (SUPINE) as well in an elevated leg position (ELEVATION, at a height of 68 cm). During the entire study period both study groups were not bed ridden, however before perfusion assessments, the patients were kept in a resting supine position for at least 20 minutes. The first assessment was conducted without negative pressure (BASELINE measurement), then after starting the NPWT therapy perfusion measurements were performed twice daily (morning and evening, in total six measurements under continuous suction). After the 3 days sequence of therapy, a completion assessment without negative pressure (turned off 30 minutes before) was conducted (COMPLETION) (compare Fig. 2). Therefore, the effect of the NPWT could be investigated. Additionally, the patients’ comorbidities (arterial hypertension, diabetes mellitus, dyslipidaemia, current smoker, mean ankle brachial index) were recorded.
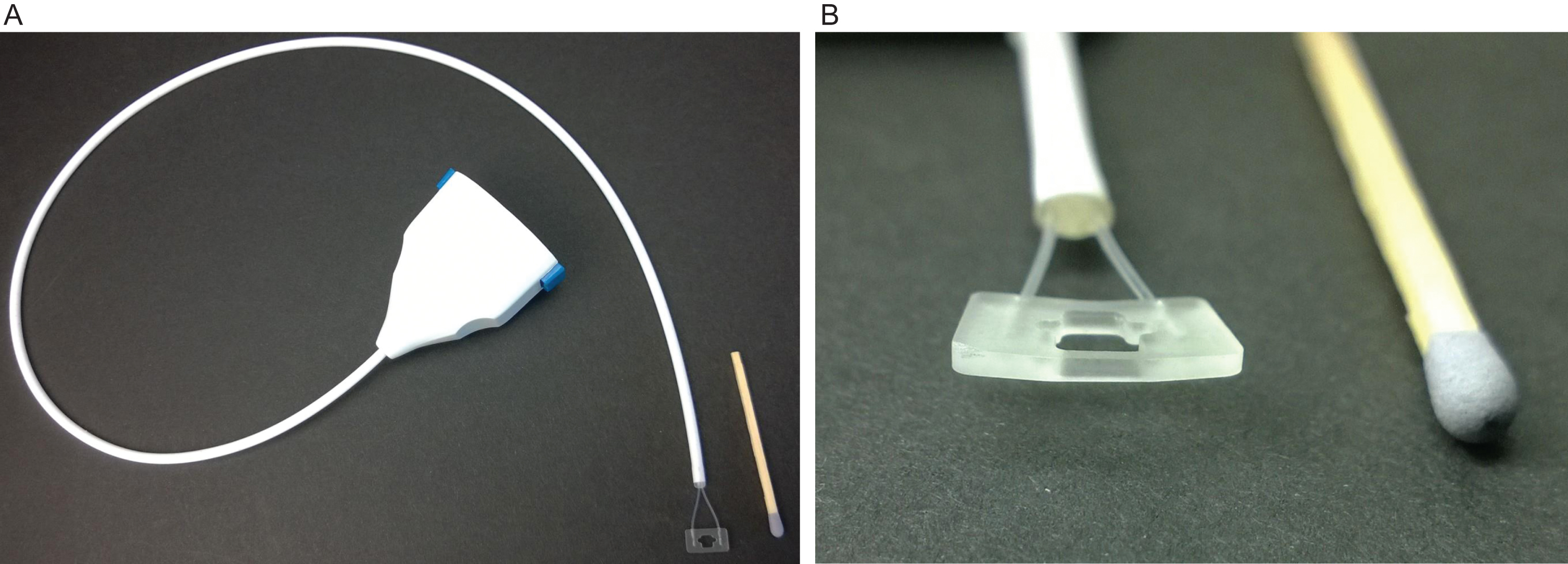
A and B.

Study setting.
The O2C device is a combined method of laser-Doppler flowmetry and white light tissue spectrometry. It uses white light of 500–630 nm wavelength as well as laser light of 830 nm wave length. The white light registers the hemoglobin oxygen saturation and relative hemoglobin amount (sO2 and rHb). The emitted laser light, detects the parameter flow which is caused by a Doppler shift by the erythrocytes on the level of microcirculation. This principle has been reported in detail before [12–14]. Due to the study’s setting and the probe configuration, we focused on the parameters flow for the evaluation of the wound bed (given in arbitrary units, A.U.).
Probes specially designed and approved (CE mark) for the application in a sterile setting on the wound bed were used (probe type LFX-69, compare Fig. 1 A and B).
Statistical analysis
All statistical calculations were performed using SPSS 21 (SPSS Inc., Chicago, IL, USA). In case of normal distribution, the mean and standard deviation (SD) was used, in cases of skewed distribution median values together with range were used. The comparison of two independent groups was performed using the chi-squared test, Fisher’s exact test, the Mann-Whitney U test, or a two-sample t-test, as appropriate. For the comparison of dependent groups the Wilcoxon test or the Friedman test was used. For all statistical tests, p < 0.05 was set to show a statistically significant difference
Results
Patients
28 patients (women 8, men 20; mean age 67.6, SD 10.6 years) were prospectively included in this study. The patients’ comorbidities are displayed in Table 1. The test for differences between the group CHRONIC and ACUTE revealed no significant differences, except for diabetes mellitus which was more often found in the CHRONIC group, and the ankle-brachial index that was significantly lower in the CHRONIC group.
Comorbidities
Comorbidities
For the assessment of the wound bed perfusion, it was necessary to place the probes directly on the wound. The probes were therefore licensed and sterilized. This was possible in nearly all cases except for two. In two cases there was a fracture of the probe line that led to an abruption of the measurement. These patients were excluded from the study.
Perfusion assessments during NPWT
The perfusion assessments were conducted during the entire sequence of the NPWT of three days. Firstly, the median BASELINE (before starting NPWT) values were compared to the COMPLETION (after finishing NPWT) values, both without suction. The CHRONIC group showed an improvement of the FLOW values, whereas on the contrary, the ACUTE group yielded reduced perfusion values after the suction sequence (CHRONIC: SUPINE: BASELINE: 217.0 range 484 A.U., COMPLETION: 341.5 range 250.0 A.U., p = 0.144; ELEVATION: BASELINE: 101.0 range 357 A.U., COMPLETION: 329.0 range 191 A.U., p = 0.068; ACUTE: SUPINE: BASELINE: 217.0 range 338 A.U., COMPLETION 172.0 range 256 A.U., p = 0.012; ELEVATION: BASELINE: 215.0 range 399 A.U., COMPLETION 209.5 range 435 A.U., p = 0.034).
Additionally, the entire period of the negative pressure therapy was investigated. The results are displayed in Figs. 3 A/B and 4A/B Further testing over time showed a significant reduction of the FLOW values in the ACUTE group (SUPINE: p = 0.021, ELEVATION: p = 0.012). In the CHRONIC group non-significant elevation of the perfusion values was recognized (SUPINE: p = 0.320, ELEVATION: p = 0.053).
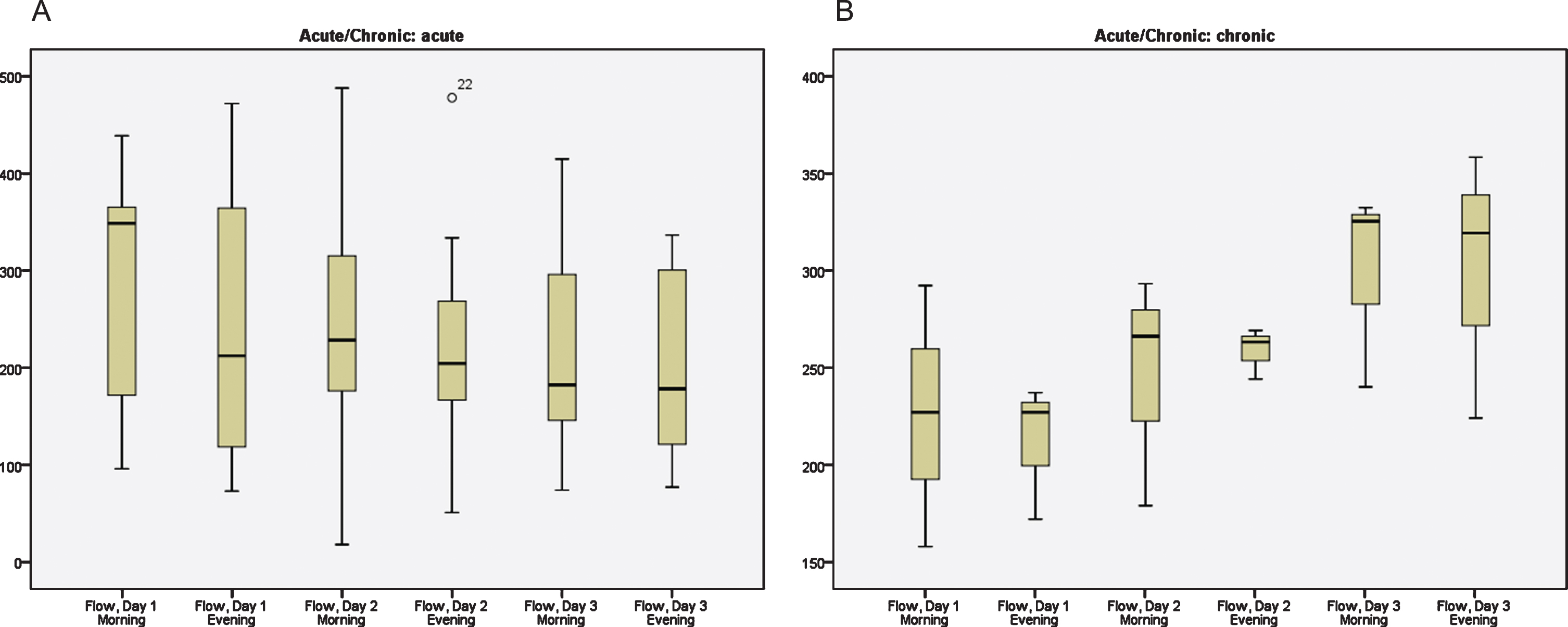
Distribution of the median flow values during the negative pressure wound therapy in the ACUTE (A) and CHRONIC (B) group in the position SUPINE; y-axis: FLOW in A.U.; x-axis: time point of measurement.

Distribution of the median flow values during the negative pressure wound therapy in the ACUTE (A) and CHRONIC (B) group in the position ELEVATION; y-axis: FLOW in A.U.; x-axis: time point of measurement.
Further comparison of the absolute values between the groups ACUTE and CHRONIC before and after NPWT was conducted. Before NPWT there were no significant differences found between both groups (CHRONIC vs. ACUTE: SUPINE p = 0.954, ELEVATION p = 0.215). However, after a three day sequence of NPWT a tendency for improved FLOW values in the CHRONIC group was found (CHRONIC vs. ACUTE: SUPINE p = 0.011, ELEVATION p = 0.099).
Discussion
Since more than 20 years, vacuum-assisted closure has been shown to promote wound healing by increasing rates of wound bed granulation tissue [15, 16]. The specific effects of NPWT application as to (micro-)perfusion of wounds however remain undisclosed to this date [6]. A widely discussed concept postulated an increase of blood flow within the wound, caused by the NPWT pressure gradient [17, 18]. However in most current literature, blood flow was only measured by flow meter probes in terms of macroperfusion [17] or indirectly with laser Doppler probes of wound‘s edge [10] or under suction on intact skin [19].
Due to these heterogeneous study protocols in terms of analyzed tissues and measuring methods, inconclusive results have been described [20]: Increase of perfusion parameters was found in NPWT on closed incisions [9] and healthy skin [20], whereas reduction of blood flow was seen in open abdomen at the intestinal wall in an animal model [21]. Another confounding factor regarding the transfer of those NPWT microperfusion changes to a clinical wound setting is the vascular compromise of oftentimes diabetic patients with foot wounds [22]. Against this background we developed a two-armed study design for evaluation of immediate microperfusion alterations during ongoing vacuum assisted close therapy. The first arm comprised of patients without any macroperfusional vessel disease, particularly absence of peripheral artery disease was defined as inclusion criteria in this subgroup; these patients were recruited after performance of fasciotomies due to compartment’s syndrome; fasciotomy wounds received temporary NPWT before secondary closure or split-skin grafting. To account for the confounder of impaired macrocirculation, we included a control group of patients with chronic wounds due to peripheral artery disease. For continuous measurements below the NPWT dressing we used a new kind of laser Doppler probes, specifically designed and sterilized for this purpose, which could be placed directly on the wound under the polyurethan foam and fastened by the adhesive foil. We could demonstrate in our perfusion assessments, that blood flow was reduced after NPWT in the acute group with absence of vascular disease compared to baseline values, whereas blood flow showed a tendency of rise after NPWT in case of chronic wounds. This difference between the two groups was also confirmed by analysis over time in continuous measurements and baseline flow values did not show any significant difference as to both subgroups.
These findings do on the one hand underline the distinct aetiology and healing process of both analyzed wound types and on the other hand may give a possible explanation of the conflicting evidence of NPWT effects on tissue microperfusion, which have been published to this date. Increased microperfusion in the area of chronic wounds as consequence of NPWT, detected by the present study, is supported by a recent case series, where histopathological examination of chronic wounds was performed. Wound bed environment was found to be facilitated by angiogenesis after a one week treatment [23] and capillary dilation has been proposed as an additional factor [15, 24]. The increase in microperfusion by promotion of angiogenesis in those wounds was confirmed on a molecular level as well [25]. On the contrary, in vitro experiments detected a temporary decreased flow in vessel imitations by NPWT [26] which has also been seen in studies evaluating NPWT effects on skin, where perfusion decrease dependent on suction pressure increase was found [27]. Based on these findings, our clinical conclusion is therefore to promote the use of NPWT in chronic limb ischemia; in this context, the combination of macrovascular vessel revascularization (either by endovascular or surgical means) and NWPT might be the most beneficial treatment option for ischemic wounds in these patients.
However, in our view there is a considerable distinction in terms of local environment between application of NPWT on open wounds and intact skin in healthy volunteers; this protective intact epidermis is of course absent in a wound situation, which precludes transfer of intact skin perfusion measurements to analysis of microperfusion of the wound’s bed especially in vascular compromised patients.
The reason for observed temporary decrease of microperfusion in acute wounds might be determined by the different tissue on which the probe is placed. Fasciotomy wounds in patients with absence of vascular disease expose well vascularized lower leg muscle tissue; in these cases, wound environment might be comparable to measurements in healthy volunteers where perfusion reduction is well documented in literature [19, 28]. There is some evidence that increased tissue pressure may be the driving factor for wound healing in this aetiology [19] and might be also true for wound closure by means of skin grafting after fasciotomy; reduction of edema and creation of close contact between split skin graft and wound bed might by NPWT be of higher relevance in relation to temporarily decrease blood flow in our view. Based on these results we might hypothesize that microperfusion under NPWT is dependent on wound aetiology and concomitant factors as for example vascular impairment due to peripheral artery disease.
Limitations of present study include the limited sample size of patients in evaluated subgroups, which was designed and conducted as a pilot study. Secondly, influence of measured results by suction pressure on laser Doppler probes cannot be excluded. It’s findings however must be confirmed by upcoming analyses with controlled evaluation of intact skin, acute and chronic wounds with application of separate measuring methods.
Conclusion
Microperfusion measurements by laser Doppler probes beneath NPWT is feasible. It showed significant alterations and differences in wound bed perfusion of acute and chronic wounds; acute wounds tended to a decrease of blood flow, whereas an increase was seen over time in chronic wounds in peripheral artery disease; wound bed perfusion might be dependent on wound etiology and presence of macrovascular disease.
Footnotes
Acknowledgments
None.
Funding
None.
Conflicts of interest
None.