
Abstract
BACKGROUND:
Tumor angiogenesis plays a critical role in the growth and metastasis of breast cancer. Evaluating the added value of vascular features to Breast Imaging Reporting and Data System (BI-RADS) in differentiating malignant masses from benign ones is essential. Micro-flow Imaging (MFI) is a promising noninvasive diagnostic method for the microvessels in breast tumors, but its precise value is still uncertain.
OBJECTIVES:
Understanding whether malignant tumor vascular characteristics by MFI are associated with breast cancer and whether the diagnostic efficiency varies by age.
MATERIALS AND METHODS:
B-mode ultrasound and MFI were performed for 153 solid breast lesions. The vessels images by MFI were reviewed and assessed by two investigators, respectively. Then the diagnostic efficacy of different vascular features combined with BI-RADS was evaluated in different age groups.
RESULTS:
The mean size of lesions is 19.4 (range 18–78) mm. There were 94 breast masses in benign, while 59 breast masses in malignant by pathology. III Adler classification, penetrating vessels, and complex flow pattern showed a positive association with a high risk of malignant breast lesions (p < 0.05). BI-RADS combined with vessel characteristics show better improvement of diagnostic performance of breast lesions in the elderly group than in the young group.
CONCLUSIONS:
Vascular features by MFI contribute to malignant breast masses’ diagnosis, and the association might be modified by age.
Introduction
Tumor angiogenesis plays a critical role in the growth and metastasis of breast cancer [1]. Vascularization between benign breast mass and malignant breast mass differs by angiogenic factors from the tumor cell [2]. Therefore, malignant lesions exhibit a higher blood flow classification, more frequent penetrating and central vessels, and more complex vessel morphology, which are considered malignant vascular features [3, 4]. And the evaluation of the tumor vascularization is mentioned in the Breast Imaging Reporting and Data System (BI-RADS; American College of Radiology, 2013).
High-resolution ultrasound is a widely available technique imaging for evaluating the vascularity of tumors, which is repeatable and safe. However, the vascular features were still hard to play a pivotal role in diagnosing malignant mass. One of the obstacles might be the poor agreement between the vascular features on traditional Doppler ultrasound and the microvessel density [5, 6]. Color Doppler Flow Imaging removes clutter and motion artifacts wall filter, resulting in a loss of low-flow components [7]. Power Doppler Imaging could display penetrating vessels and partly vessel pattern with greater sensitivity than Color Doppler Flow Imaging [8]. Recently, some new techniques for detecting microvessels have been introduced, such as Micro-flow Imaging (MFI) and Superb Microvascular Imaging, distinguishing flow signals from overlaying artifacts due to tissue motion and preserving the actual blood flow. These technologies apply a novel spatial-temporal filter to improve spatial resolution, reduce noise, and present tiny blood vessels, making the images closer to actual blood flow [9–11]. According to some published studies, MFI is superior in detecting tiny blood flow signals and showing up vascular architecture than Power Doppler Imaging, performing a higher coincidence rate to contrast-enhanced ultrasound [4, 10].
As mentioned above, the contribution of microvessel assessment by MFI in distinguishing malignant breast masses from benign lesions is highly significant. But the usefulness of using vessel assessment to differentiate malignant breast mass is inconsistent. Neovascularization may appear in malignant and benign lesions, causing the overlapping vascular image feature in ultrasound [12]. Moreover, some benign breast masses showed a penetrating vascular pattern, and a richer blood flow signal resembled breast cancer, especially in cases that multiply quickly [3].
Age is one of the established breast cancer risk factors, suggesting that tumor biological characteristics are partly differed by age [13, 14]. Although several studies have examined the association between vascularity and breast cancer, participants’ age was in little attention. According to the known differences in the tumor biology of younger and older women diagnosed with breast cancer, this prospective study aims to understand whether vessel features are a potential risk factor for malignant breast lesions and whether the associations are consistent at different ages.
Materials and methods
Patients
The Institutional Review Board for Ethical Issues in Clinical Research approved this prospective study, and all patients have provided written informed consent. From December 2020 to June 2021, 153 solid breast masses on the conventional ultrasound classified as category 3, 4, or 5 in 152 females (mean age 45.2±13.5 years, range 18–78 years) were included in this study. We excluded the patients who had been treated with radiation or breast surgery within two years. All individuals underwent excision (146) or biopsy (7) within one week after the ultrasound and had histological confirmation.
Ultrasound examinations
Ultrasound examinations were performed using an eL18-4 linear transducer and a Philips EPIQ7 (Philips Medical Systems, Bothell, WA, USA), equipped with MFI software. After identifying the focal breast lesion, the sonographer with 5 years of experience in ultrasound breast examination first scanned the mass in gray-scale ultrasonography with transverse and sagittal views. The BI-RADS (2013) assessment and maximum cross-section of lesions were recorded. Then MFI was performed sequentially, and dynamic images (3 seconds) with maximum color signals but no diffuse artifacts were saved. The sampling window was set to an adequate size to include the lesion and necessary surroundings during the testing process, and no pressure should be applied with the ultrasound probe to avoid loss of the microflow signal. The MFI dynamic images were reviewed respectively by two other sonographers with 2 and 10 years of experience in ultrasound diagnosis. The experimental plane with the most luxuriant vessels but the minor background color interference was chosen for evaluation as the representative image. Both of them were blinded to patient identification, clinical history, and pathology results. The initial assessments of vascularity features from two sonographers were recorded respectively for the interobserver consistency test. The evaluations to be used for the final statistical analysis were a consensus after discussion. Based on previous studies, the diagnostic criteria of parameters are as follows: (1) The penetrating vessels were defined as a corresponding blood flow signal extending from outside the mass to inside, and stable arterial signals could be detected. (2) The complex vessel pattern means the thick and twisted vessels. (3) The central flow distribution means more flow signals in the lesion than around the lesion. (4) The Adler classification method: Grade 1: one or two dot-like or short line blood vessels within the lesion; Grade 2: three or four dot-like or one long line blood vessels within the lesion; Grade 3: more than five dot-like or two long line blood vessels within the lesion [8, 15]. (5) The BI-RADS (2013): Category 3: probably benign; Category 4a: low suspicion for malignancy; Category 4b: reasonable suspicion for malignancy; Category 4c: high suspicion for malignancy; Category 5: highly suggestive of malignancy. According to BI-RADS, breast masses classified as category 4a and above are suggested to take a needle or surgical biopsy. Thus, in this study, the breast mass as category 3 was assumed to be negative, and category 4 or 5 to be positive.
Corrected BI-RADS classification based on different vascular characteristics
Grade 3 Adler classification, penetrating vessels, central vessels, or complex vessel morphology was defined as a positive finding. A vessel parameter with a statistically significant difference would be used for the correction of BI-RADS subcategorization. In view of a grade down from BI-RADS category 4b, 4c and 5 would not transform the final suggestion (needle or surgical biopsy), we performed the correction as follows: (1) A breast lesion of BI-RADS category 3 with one or more positive finding would be upgraded to 4a. (2) A breast lesion of BI-RADS category 4a with no positive finding would be downgraded to 3. (3) A breast lesion of BI-RADS category 4b, 4c and 5 would not be adjusted.
Statistical analyses
The maximum diameter and age were disposed of as continuous variables, while other variates were disposed of as categorical variables. Continuous variables were expressed by mean (SD), while categorical variables by proportions. The initial assessment of vessels from two sonographers was compared by Cohen’s kappa coefficient analysis.
All the cases were stratified into two groups based on the pathology results, benign lesions and malignant lesions. The student’s t-test and the chi-square test were used to examine the differences among the different groups. The vascular characteristics that differ significantly between groups will be used for downgrading or upgrading. Then all the participants were stratified into two groups based on age (≤45 or > 45 years old), and the receiver operating characteristic (ROC) curve analysis was used to compare the diagnostic performance among the original BI-RADS assessment and BI-RADS assessment plus one of the significant vessel parameters respectively under two age groups. The area under the ROC curve (AUC), sensitivity, specificity, and accuracy were calculated.
All the analyses were performed by SPSS version 26.0 software (SPSS, Chicago, IL, USA). And a two-sided p value < 0.05 was considered statistically significant.
Results
Interobserver agreement of MFI
The Cohen’s kappa coefficient for penetrating vessels, vessel pattern, flow distribution, and Adler classification from two radiologists are 0.87, 0.75, 0.77, and 0.81, respectively, manifesting a solid interobserver consistency.
Basic information and flow signal characteristics by MFI
A total of 153 breast masses (94 in benign, 59 in malignant) in 152 women were confirmed by pathology. The characteristics and the detailed histological results of cases are shown in Tables 1 2 respectively. The mean age of the participants is 45.2 (±13.5, range 18–78) years old, and 49.7%of them are older than 45 years old. The average size of the benign lesions is smaller than the malignant lesions (p < 0.05). And no difference was found in the lesion size between the two age groups (18.5 mm vs. 20.2 mm, p > 0.05). For vessel characteristics on MFI in all participants, malignant masses show a greater percentage of Grade 3 Adler classification (78.0% vs. 46.8%, p < 0.05), penetrating vessels (76.3% vs. 42.6%, p < 0.05), and complex vessel pattern (78.0% vs. 26.6%, p < 0.05) (Fig. 1). No significant results in the association by central flow distribution versus cancer.
Baseline characteristics and vascular features of 153 breast lesions
Baseline characteristics and vascular features of 153 breast lesions
Number of positive vascular characteristics in different pathological lesions
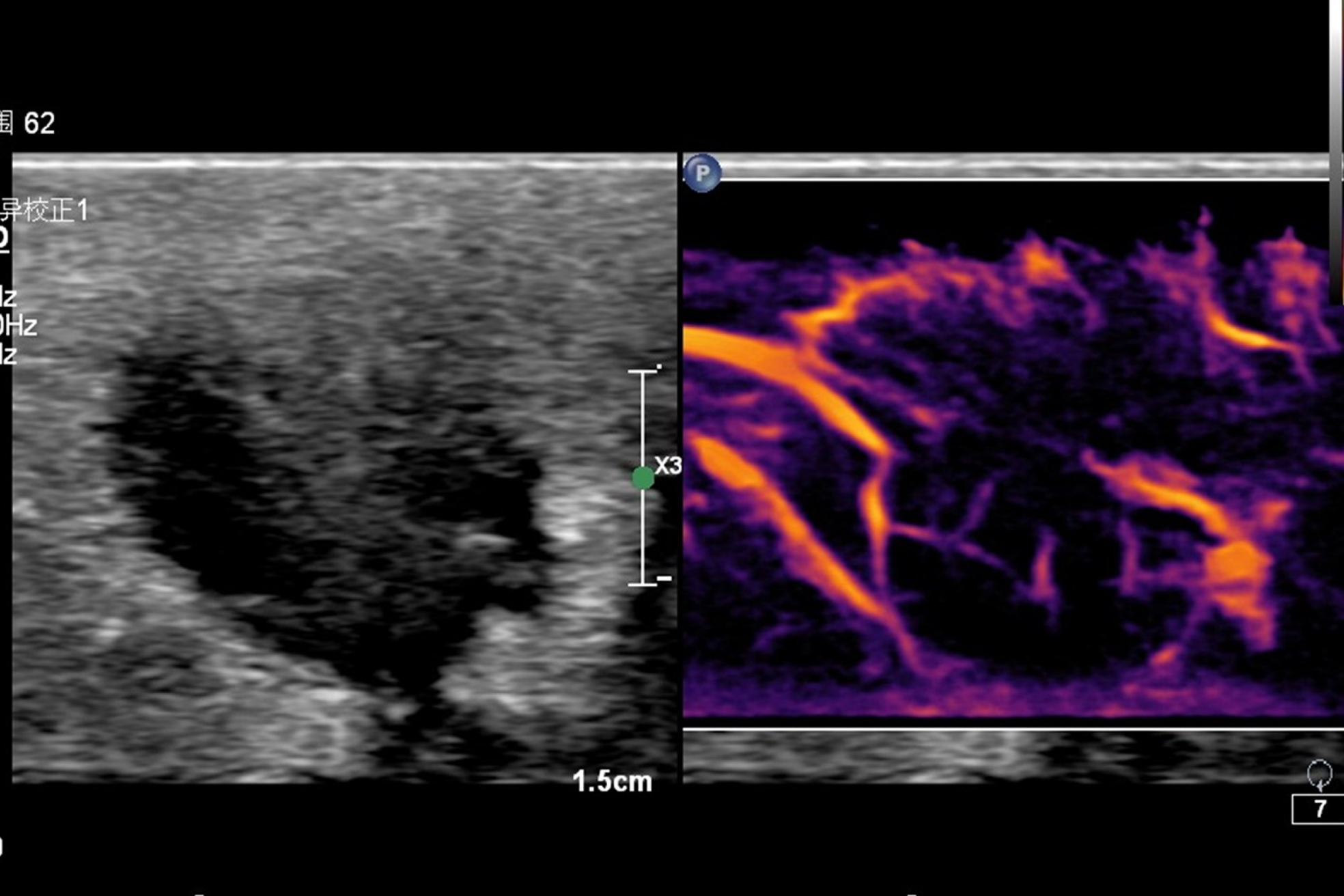
A 55-year-old female with invasive ductal carcinoma. Left: The gray-scale ultrasound image. Right: The micro-flow imaging (MFI) image shows penetrating vessel, complex vessel pattern, and III Adler classification.
For Adler classification, 28 breast masses were adjusted from category 3 to 4a while 17 breast masses from category 4a to 3. For penetrating vessels, 26 breast masses were adjusted from category 3 to 4a while 18 breast masses from category 4a to 3. For vessel pattern, 17 breast masses were adjusted from category 3 to 4a while 25 breast masses from category 4a to 3.
Diagnostic value of different vascular characteristics in different age groups
The diagnostic value of breast lesions in participants aged 45 and below is shown in Table 3. The specificity and accuracy of BI-RADS combined with complex vessel pattern are superior to BI-RADS alone (p > 0.05). And compared with before the correction, BI-RADS combined with penetrating vessels or Adler classification would lower the specificity and accuracy (p < 0.05). The AUC is 0.777 for BI-RADS alone, 0.676 (p < 0.05) for combined with Adler classification, 0.718 (p < 0.05) for combined with penetrating vessels, and 0.803 (p > 0.05) for combined with vessel pattern (Fig. 2).
Diagnostic performance in differentiating malignant from benign masses in young group
Diagnostic performance in differentiating malignant from benign masses in young group
PPV = Positive Predictive Value; NPV = Negative Predictive Value; BI-RADS = Breast Imaging Reporting and Data System; AUC = Areas Under the ROC curves. *p < 0.05, versus BI-RADS.

The Receiver Operating Characteristic (ROC) curve for various vascular features plus BI-RADS for the participants of 45 years old and below.
The diagnostic value of breast lesions in participants older than 45 years old is shown in Table 4. The sensitivity, specificity, and accuracy of BI-RADS combined with vessel pattern, penetrating vessels, or Adler classification is all significantly superior to BI-RADS alone (p < 0.05). The AUC is 0.723 for BI-RADS alone, 0.831 (p < 0.05) for combined with Adler classification, 0.814 (p < 0.05) for combined with penetrating vessels, and 0.876 (p < 0.05) for combined with vessel pattern (Fig. 3).
Diagnostic performance in differentiating malignant from benign masses in elderly group
PPV = Positive Predictive Value; NPV = Negative Predictive Value; BI-RADS = Breast Imaging Reporting and Data System; AUC = Areas Under the ROC curves. *p < 0.05, versus BI-RADS.

The Receiver Operating Characteristic (ROC) curve for various vascular features plus BI-RADS for the participants over 45.
According to this research, higher blood flow classification, penetrating vessels, and complex flow pattern are associated with a higher risk of malignant breast lesions. And there is no apparent difference in the risk of cancer by central flow distribution in all ages. Different from previous studies, this study result indicated that differentially diagnostic value of varying vessel characteristics is defined by age. The accuracy of BI-RADS combined with penetrating vessels or Adler classification is raised in the elderly group while decreased in the young group. And BI-RADS combined with flow pattern shows the most significant improvement of accuracy than others in all age groups. A similar result was observed in the ROC curves analysis. These findings point to possible heterogeneity in tumor vascular characteristics and underscore the importance of examining age-specific associations.
Several previous studies have reported hypervascularity, complex vessel pattern, central flow distribution, and penetrating vessels can help discriminate breast cancer from benign tumors [16]. In comparison, our study result suggests that central flow distribution is helpless. Angiogenic factors, especially vascular endothelial growth factors, are highly expressed in malignant breast tumors, which directly stimulate the growth of new blood vessels [1]. The rapid genesis of tumor vascularity leads to an anarchical structure, which could be observed as higher vessel classification, penetrating vessels, and complex flow pattern. However, at the center of the malignant breast tumors, the microvessel density would decrease partly because of the necrosis, which had been confirmed by contrast-enhanced ultrasound and immunohistochemical analysis [17–19]. Most previous studies reported that penetrating vessels in the breast mass was one of the diagnostic criteria for malignancy [20, 21]. In contrast, others indicated that flow pattern analysis is more reliable than the vascular semiquantitative evaluation and detection of penetrating vessels in differentiating malignant breast lesions [4, 22]. Our research provides new insight that the different vascular parameters in the magnitude of diagnostic value with breast cancer significantly variation across age groups. For the lesions in participants aged 45 and below, 47.5%of benign lesions were detected with penetrating vessels, and 57.6%of benign lesions were detected in the Grade 3 Adler classification. It suggests that using penetrating vessels or semiquantitative vascular evaluation for upgrading BI-RADS in youth patients might lead to a higher misdiagnosis rate. For lesions in participants older than 45 years old, the sensitivity, specificity, and accuracy of combining penetrating vessels, flow pattern, or semiquantitative flow grading with BI-RADS are significantly higher than those of BI-RADS alone. These partly because the physiology of the breast is associated with women’s age, menopausal status, parity, and others [23]. The higher hormonal level in young women leading the breast mass shows more long line blood vessels, making it difficult to differentiate between malignant lesions and benign lesions by penetrating vessels or Adler classification. Indeed, flow pattern plus BI-RADS is in higher specificity, sensitivity, and accuracy in all ages. It suggests that radiologists should remain vigilant with the breast mass detected a complex vessel pattern, even though it was in category 3.
To our knowledge, this study is the first to propose the relationship between age and the vessel’s feature of breast cancer. As a morphologic characteristic, interobserver variability is of great concern. In this study, we evaluated the assessments of the vascular features on senior and junior radiologists and found that a good consistency. In addition, we classified only two vascular morphologic features (complex vessel and linear vessel) for strong practicality in clinical application.
MFI is a noninvasive and reproducible vascular imaging technology with high diagnostic reliability of breast cancer when combined with conventional ultrasound in our study. It is implementable to be performed after adequate training and takes only a few minutes after the B-mode ultrasound examination. Other perfusion imaging methods, such as contrast-enhanced ultrasound and enhancement MR imaging, were reported that in good diagnostic performance but with considerable external cost in economy and imaging time [19, 24]. Also, B-mode integrated with other ultrasound techniques like B-Flow and elastography, were reported could improve the diagnostic accuracy of tumors. And other research has noted that the help which elastography contributed to BI-RADS was greater for small breast lesions and lesions in elderly patients [25]. Thus, the differences in specific added value, suitable applying conditions, advantages, and disadvantages among these new techniques is worth to concern.
Some limitations to this study are worth noting. First, the acquisition of high-quality MFI is operator-dependent, and only a few ultrasonic scanners allow for this examination currently. Second, the diagnosis for small breast lesions is a difficult subject in this field, especially the tumors which were hard to be detected by ultrasound, but detectable by MRI or mammography [26]. It deserves further investigation in a larger sample size. Furthermore, our analysis was performed in a single center. A large-scale, multi-center prospective study is required.
Conclusions
We thought that using vascular features by MFI as an additional diagnostic criterion for malignant breast masses was a reliable and reproducible modality. Furthermore, incorporating the age of patients when considering vascular features might allow clinicians to identify the breast mass at an increased risk of cancer more keenly and accurately.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflictss of interest
None.