
Abstract
OBJECTIVE:
The aim of this study was to investigate the role of cerebroplacental ratio (CPR) in the final prenatal care for neonatal respiratory diseases and to analyze the risk of relevant factors associated with neonatal respiratory disorders.
METHODS:
A prospective cohort study of 795 singleton pregnancies was conducted. The pulsatility indices (PI) of the umbilical artery (UA) and the middle cerebral artery (MCA) were measured, and the MCA to UA ratio (CPR) was determined. The severity of the case is determined by whether or not the newborn has respiratory problems. Compare the CPR correlation between the two groups and examine the illness prediction factors through a binary logistic regression method.
RESULTS:
Of the 795 participants, 124 had neonatal respiratory disorders. The mean values of CPR between neonatal respiratory diseases group and control group were 1.78±0.6, 1.97±0.9, respectively (P < 0.001). Maternal age, abortion history, cesarean section history, placental thickness, placental maturity, and amniotic fluid index (AFI) were determined to have no significant link between the two groups after comparison analysis (P > 0.05). It could be found that compared with the control group, CPR MoM indicators of neonatal respiratory distress syndrome, neonatal pneumonia and wet lung disease all show significant decreases. In binary logistic regression analysis, among the variables included in the model, CPR (OR:2.90, P = 0.015), fetal heart monitoring (OR:5.26, P < 0.001), delivery mode (OR:2.86, P < 0.001) and gestational age of delivery (OR:0.92, P < 0.001) were statistically significant in both groups.
CONCLUSION:
The findings of this study showed that infant respiratory problems were substantially related to CPR value. The correlation indicates that CPR was a powerful reference marker for respiratory disorders.
Keywords
Introduction
Neonatal respiratory disorders include wet lung disease, neonatal pneumonia, and respiratory distress syndrome. Respiratory distress syndrome, which occurs in approximately 7% of infants [1], is a major cause of morbidity and mortality associated with preterm birth [2]. These diseases are often caused by an apparent lack of alveolar surfactant, accompanied by the immature development of the lungs [3].
Certain indicators, including pulmonary permeability, edema, and inflammation, cannot be routinely measured in a clinical setting. The experience in predicting fetal respiratory disorders is limited because the diagnoses rely on clinical features and imaging as alternatives [4, 5]. Doppler ultrasonography is an important technique in prenatal diagnosis [6]. Furthermore, Doppler ultrasonography makes examining the circulation of the fetal heart, fetal lung, and placenta more easier and it can be used to indirectly evaluate the function of these organs and the relationships between them [6].
The cerebroplacental ratio (CPR) is an important indicator for evaluating the occurrence and development of diseases during pregnancy [7]. In earlier research, Arbeille et al. [8, 9] showed that the CPR, which characterizes the fetal flow redistribution between the placenta and brain, enables a fast and real-time imaging of the changes in hemodynamics and oxygen partial pressure. The adaptive redistribution of fetal blood flow further affects the growth and development of the fetal organs, such as the fetal pulmonary maturity. Neonatal respiratory diseases is often a consequence of prematurity or maldevelopment of the fetal lung. Therefore, the purpose of this study is to discuss whether the the CPR is a sensitive indicator for neonatal respiratory diseases.
Materials and methods
A prospective cohort study was conducted at our institution. A total of 867 singleton pregnancies with a gestational age of 30–41 weeks between November 2020 and March 2021 were included. The study was approved by the Institutional Review Committee of our hospital, and patients gave their informed consent to participate in the research. Subjects were excluded if they have the following conditions: a) incomplete prenatal clinical data or not delivered in our hospital; b) multiple gestations; c) a malformed or chromosomally abnormal fetus; and d) blood flow parameters of the middle cerebral artery (MCA) cannot be measured. The demographic data were collected from the cases in our hospital’s building card, while the clinical data were collected during subsequent prenatal visits and from discharge records. Maternal age, gravidity, parity, history of abortion, cesarean section history, gestational age at the time of ultrasound and delivery, results of non-stress tests, amniotic fluid index (AFI), placental maturity and thickness, and pregnancy complication were recorded for each woman. The Apgar score at the first minute, birth weight, umbilical artery resistance index (UA-PI), MCA resistance index (MCA-PI), and admission to the Neonatal Intensive Care Unit (NICU) were recorded for each fetus.
Both UA and MCA hemodynamics were performed during the patient’s routine prenatal examination. The ultrasonic examinations were performed using Philip EPIQ 5C ultrasound diagnostic system (EPIQ Elite W, Philips, The Netherlands) with a frequency of the C5-1 probe (the centre frequency was 3.2 MHz). A sonographer who had more than 5 years of experience in obstetrics and gynaecology ultrasound imaging performed all the examinations. Doppler examinations were performed with the fetus in a quiet state in absence of fetal movements. First, the position of the MCA was located. Upon identification of the standard plane of the fetal double parietal diameter, it was then translated to clearly show the fetal basilar ring (Willis). The sampling volume in the middle segment of the fluctuating blood vessels was located. The angle between the direction of the ultrasound beam and the blood flow was less than 30 degrees. Three complete and clear pulse Doppler flow images of the proximal field MCA were obtained. After the placenta position was determined, the free segment of the UA was explored. With detection of the typical umbilical cord blood flow waveform, the instrument automatically could show the image of the UA blood flow (Fig. 1). Each data was measured three times, and the mean value was identified as the final data. The CPR was calculated as a simple ratio of MCA-PI divided by UA-PI. In view of eliminating the influence of gestational age factors on the absolute value of MCA-PI and UA-PI, both of them were expressed as multiples of the median (MoM) when analyzing the correlation. The judgment standard of the reference value was adopted from the Fetal Medicine Foundation [10].
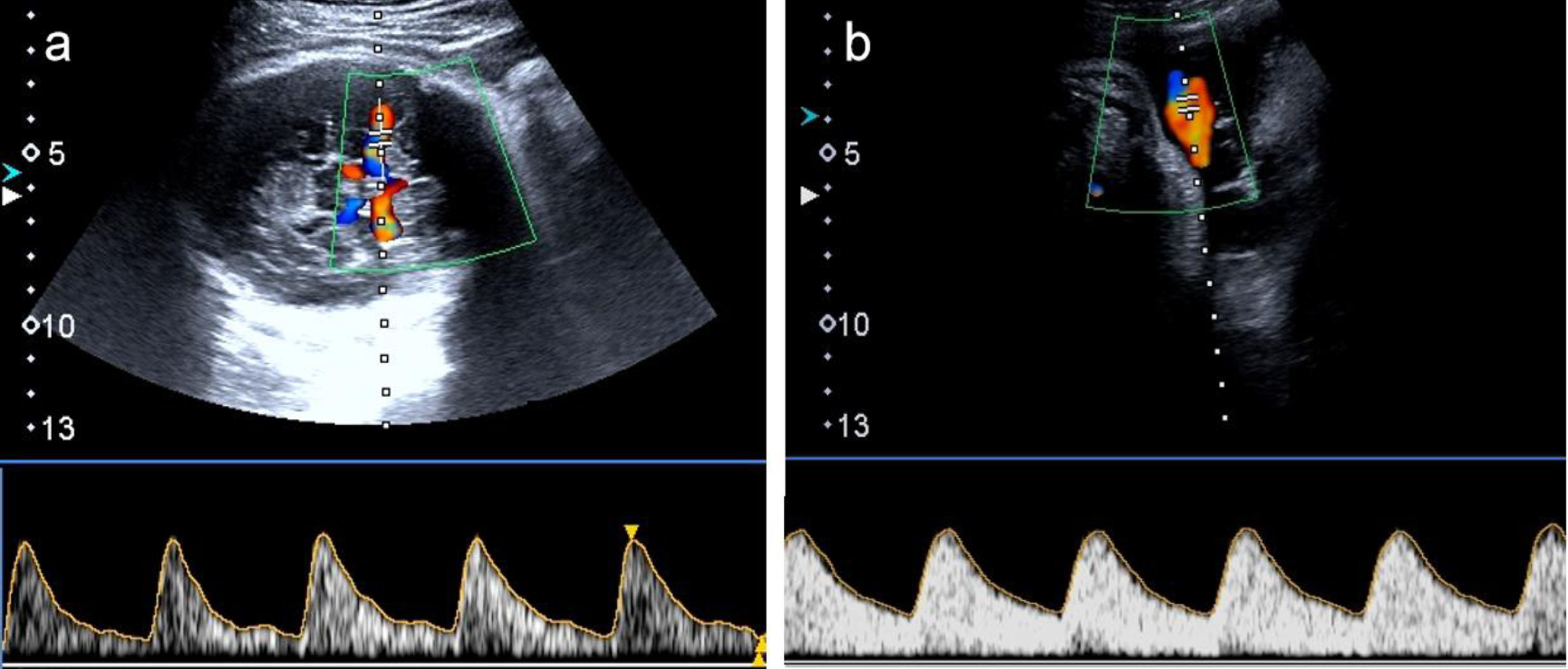
The color Doppler ultrasonography of middle cerebral artery and umbilical artery. a: The color Doppler ultrasonography of the middle cerebral artery of fetus; b: The color Doppler ultrasonography of the umbilical artery.
Examples of neonatal respiratory diseases include wet lung disease, neonatal pneumonia, respiratory distress syndrome, and so on. The clinical data collection and analysis of the cases included in this study were performed by a neonatologist. The disease was diagnosed on the basis of the clinical findings, laboratory results, chest X-ray/chest CT examination, and neonatal pulmonary ultrasound [11]. No special concomitant care or intervention was included during the perinatal period.
The diagnosis of preeclampsia (PE) was based on the recognized criteria for the PE, as revised in 2014 by the International Society for Pregnancy-Induced Hypertension [12]. The diagnosis of gestational diabetes mellitus (GDM) was based on the diabetes diagnostic and therapeutic criteria developed by the American Diabetes Association in 2010 [13]. The diagnosis of fetal intrauterine growth restriction (FGR) was based on consensus definition of fetal growth restriction (a Delphi procedure) in 2016 [14]. The setup entailed a randomized, blinded, controlled clinical trial that focused on the maternal characteristics.
Statistical analysis was performed using SPSS (IBM SPSS 20.0, SPSS Inc.) and GraphPad Prism 8.0.2 (Graphpad software Inc. San Diego,CA, USA). For the continuous variables, t-test and/or Mann Whitney U test were/was used, and Chi-square for finding the trend and the Spearman rank correlation coefficient were used for the categorical variables. A binary logistic regression analysis model was used to assess the CPR and other related factors to predict the neonatal respiratory diseases. P values less than 0.05 were considered statistically significant.
For the study period, among the 867 pregnant women enrolled in our institution for antenatal examination, 47 of them (5.4%) were excluded from the study due to the absence of delivery record in our institution or fetal malformation data. Then, 25 women (2.9%) were excluded due to incomplete clinical data. Finally, 795 cases were considered for analysis. A comparison of the main characteristics is presented in Table 1. Among the 795 participants, 124 experienced neonatal respiratory diseases. No significant difference was obtained between the normal and neonatal respiratory diseases groups in terms of maternal and obstetrics characteristics, including maternal age, abortion history, cesarean section history, and gestational age at ultrasound.
Maternal and obstetrics characteristics, Doppler ultrasound characteristics and pregnancy outcome in neonatal respiratory diseases and control groups
Maternal and obstetrics characteristics, Doppler ultrasound characteristics and pregnancy outcome in neonatal respiratory diseases and control groups
Data are presented as Mean±SD or n (%). UA-PI = Umbilical artery pulsatility index, MCA-PI = Middle cerebral artery pulsatility index, CPR = MCA-PI/ UA-PI; AFI = Amniotic Fluid Index.; Placental maturity (III): Grannum placental grading, Grade III indicates that the placenta has been senescent; GDM = Gestational Diabetes Mellitus, FGR = Fetal Growth Restriction, PE = preeclampsia; NST: Non-stimulation test; BW = Birth Weight. NICU = Neonatal Intensive Care Unit.
The key indicators of MCA and UA were evaluated on the basis of standard ultrasound examination for each enrolled patient. A significant difference was found between the neonatal respiratory diseases and normal groups in terms of MCA-PI MoM (P < 0.001) and CPR MoM (P = 0.016) but not for UA-PI MoM. Compared with the normal pregnancies, the pregnancies resulting in neonatal respiratory diseases had a higher proportion of low amniotic fluid volume (AFI < 80, 20% vs. 12%, P = 0.014), which may cause massive loss of oxygen. However, major complications, such as GDM and FGR, should not be ignored as they play a crucial role in fetal prognosis. In addition, abnormal fetal heart monitoring and unnatural delivery also play a significant role in the occurrence of diseases (P < 0.001). Obviously, a fetus affected by neonatal respiratory diseases typically manifests a lower Apgar score (neither 1-minute APGAR nor 5-minute APGAR) (P < 0.01).
Of the 124 newborns with respiratory disorders, 9 were diagnosed with neonatal respiratory distress syndrome (NRDS), 34 with neonatal pneumonia, 105 with wet lung, and 2 with pneumothorax (Table 2). It can be found that compared with the control group, CPR MoM indicators of NRDS, neonatal pneumonia and wet lung disease all show significant decreases. At the same time, the incidence of wet lung disease and pneumonia showed obvious correlation with CPR MoM indicators (Table 2, Fig. 2).
The detailed analysis of neonatal respiratory disorders with CPR indicators
Data are presented as Mean±SD; NRDS: Neonatal Respiratory Distress Syndrome; *P < 0.05, compared with the control group; r: Pearson correlation coefficient, **P < 0.05, there was a significant correlation with CPR MoM.
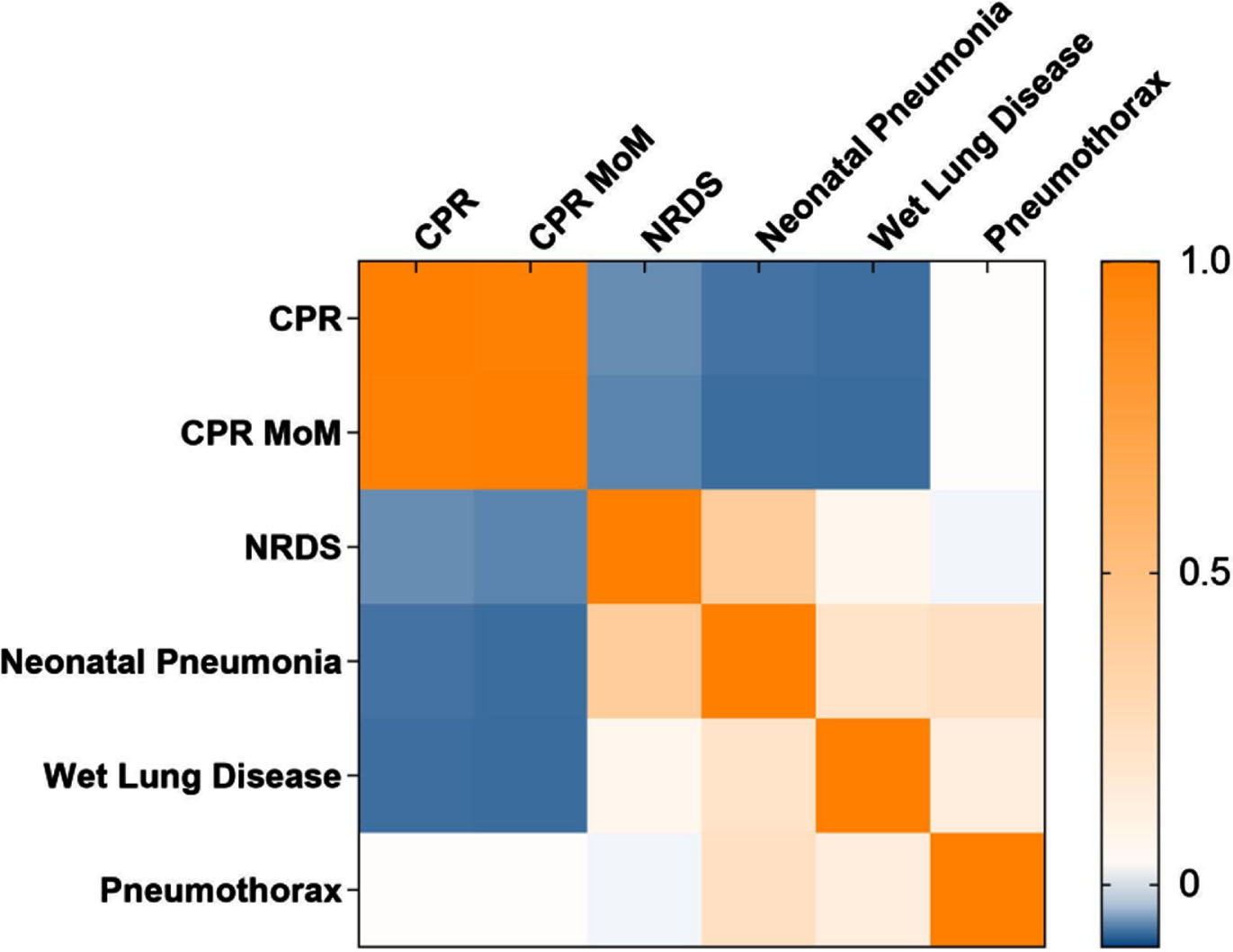
Heat map of the coefficient of correlation between respiratory disorders and CPR indicators. Each cell represents the correlation coefficient r, which is between –0.1 and 1 in this study.
The binary logistic regression analysis was performed with neonatal respiratory diseases as the dependent variable, fetal heart monitoring, delivery mode, Apgar score, MCA-PI MoM and CPR MoM as the independent variables. Among the variables included in the model, MCA-PI MoM (OR: 0.09, P = 0.002), fetal heart monitoring (OR: 6.07, P < 0.001), delivery mode (OR: 2.74, P < 0.001), and Apgar score (OR: 0.10, P < 0.001) were statistically significant in both groups, classifying them as independent risk factors of neonatal respiratory diseases. The results of this analysis are reported in Table 3. However,CPR MoM was not significant in predicting neonatal respiratory diseases outcome(OR: 0.58, P = 0.265). We compared the model’s performance with and without CPR MoM to further assess the significance of this variable. It showed that the value of –2Log likelihood in the analysis data without CPR MoM (570.75) was higher than that with CPR MoM (562.15). Meanwhile, The Area under the Curve of ROC (AUC:0.771, Fig. 3, Table 4) with CPR MoM was also higher than that without CPR MoM (AUC:0.763). In addition, We found that the Akaike information criterion (AIC) value with CPR MoM was lower than not (589.2 vs. 595.5). By measuring these criteria for the excellence of statistical model fitting, We’ve established the non-negligible nature of CPR. The results showed that the model was more optimized with the acceptance of CPR.
Predictors of neonatal respiratory diseases in binary logistic regression model
Odds Ratio (OR), regression coefficient (B), 95% confidence intervals (CI) and P-values were obtained by Binary Logistic Regression analysis.
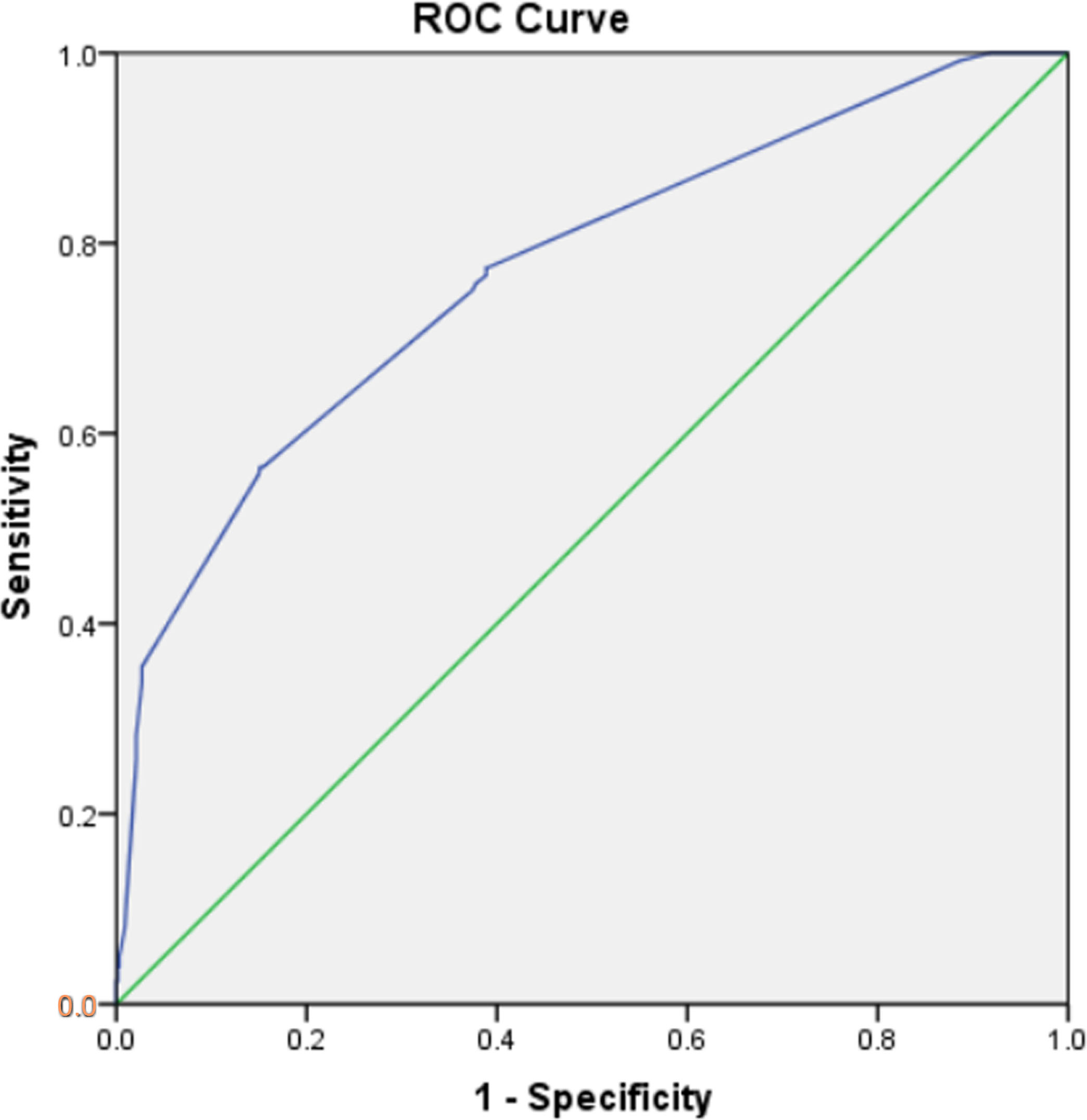
ROC curve in binary logistic regression model with CPR MoM.
Area under the curve in binary logistic regression model with CPR MoM
Cochrane trials have shown that observations via Doppler ultrasound can improve perinatal outcomes in cases of high-risk pregnancies [15]. Since its successful introduction in 1992 [16], CPR has been considered an independent predictor of intrapartum fetal compromise and neonatal unit admission [17]. Specifically, is CPR indicative of neonatal respiratory disease? In this study, We came to a conclusion that CPR parameters play a significant role in predicting the risk of neonatal respiratory disease. As a sensitive indicator following the changes in acute pO2, CPR plus MCA has been validated as having a valuable function in the prediction of neonatal lung disease.
Compelling evidence has shown that UA mirrors placental vascular insufficiency and thus can be considered a risk-discriminator tool to avoid adverse perinatal outcomes, further resulting in much fewer obstetric interventions [15, 19]. As for neonatal morbidity, CPR and MCA-PI have a good predictive ability for adverse pregnancy, especially imminent fetal hypoxia in the third trimester, but they do not perform satisfactorily in UA hemodynamics [20, 21]. Among researchers involved in animal experiments, an accepted view is for the placenta to have a large compensatory capacity [22]. As a surrogate marker of hypoxia, the MCA is a high-risk predictor of emergency cesarean during fetal distress in cases of SGA fetuses [23]. Nonetheless, MCA alteration may be a late manifestation for countering the status of the fetus. Therefore, as demonstrated by our results, the performance of CPR (calculated using the ratio of MCA to UA Doppler) risking for neonatal morbidity is promising. Previous systematic reviews also revealed that the prognostic accuracy of CPR is statistically superior to that of MCA or UA Doppler for emergency deliveries due to fetal distress and complex adverse outcomes [24, 25]. In a review, Erkan et al. [25] described that CPR appears to be a useful surrogate of suboptimal foetal growth and intrauterine hypoxia and it is associated with a variety of perinatal adverse events.Therefore,with this assessment tool, the mild changes in the chemoreceptors and baroreceptors in the blood flow can be sensitively and accurately perceived.
Neonatal respiratory diseases management in current practice is aimed at monitoring the fetal condition as a means of optimally and timely inducing delivery. The development of the fetal lung is a highly regulated process [26]. Alveolation starts after 24 weeks of gestation. Synchronously, type II pneumocytes begin to produce pulmonary surfactant, and the phosphatidylinositol and sphingomyelin gradually increase from 28 weeks of gestation. Therefore, late pregnancy is an important stage in fetal lung development. However, placental dysfunction and fetal hypoxia could contribute to the healthy growth and development of fetuses. Past studies have shown that fetal hypoxemia results in increased blood flow to the brain and heart, which then reduces the fetal lung blood supply, consequently delaying fetal development [25, 27]. This scenario is called the brain-sparing effect, i.e., the redistribution of fetal blood flow with the decrease in PO2 is aimed at safeguarding vital functions. At this time, hemodynamic monitoring is particularly important for normal pregnancy. MCA, which reflects fetal adaptation to hypoxia, combined with CPR has an important reference value for fetal lung development. Many studies in the literature proved that CPR is a notable predictor of adverse neonatal outcomes [17, 28–32], such as intrapartum fetal compromise, poor acid base status at birth, and neonatal unit admission at term pregnancies. Greggory et al. [33] also confirmed the discovery through research that an abnormal CPR could be a strong predictor of poor prenatal and postnatal outcomes in fetuses with early-onset SGA and should be included in the prenatal ultrasonography. Unsurprisingly, abnormal Doppler parameters for CPR are independently associated with fetal respiratory disorders. From the perspective of pathophysiology, fetal hypoxia may be one of the factors of lung dysplasia, and the cerebroplacental hemodynamics index is a reference marker of fetal lung maturation.
In conclusion, CPR could be an indispensable indicator in the Doppler parameters assessing the healthy development of the fetal respiratory system. Further studies are required to prove whether CRP is an early independent predictive marker of this disease, and numerous data and sufficient positive cases are needed as proof. The CPR predictive cutoff value can also be explored. We hope that CPR can help to identify fetal hypoxia at a much earlier time, assess fetal lung development, and provide support to clinical decision making.
Footnotes
Acknowledgments
We acknowledge with gratitude the women and children who participated in this study.
Conflict of interest
None of the authors have any conflict of interest to declare.