
Abstract
OBJECTIVE:
To investigate the added value of contrast-enhanced ultrasound (CEUS) and superb microvascular imaging (SMI) to the conventional ultrasound (US) in the diagnosis of breast lesions.
METHODS:
PubMed, EMBASE, Web of Science, Chinese national knowledge infrastructure databases, Chinese biomedical literature databases, and Wanfang were searched for relevant studies from November 2015 to November 2021. The quality of the included studies was evaluated using the Quality Assessment of Diagnostic Studies (QUADAS) tool. Meta-Disc version 1.4 was used to calculate sensitivity (SEN), specificity (SPE), positive likelihood ratio (LR+), negative likelihood ratio (LR–), area under curve (AUC), and diagnostic odds ratio (DOR). Meta-regression analysis was performed using STATA 16.0 software to compare the diagnostic accuracy of the two techniques.
RESULTS:
In the five studies included, 530 patients were eligible for this meta-analysis. For SMI, the pooled SEN and SPE were 0.75 (95% confidence interval [CI]: 0.69–0.91) and 0.88 (95% CI: 0.83–0.91), respectively, LR+ was 5.75 (95% CI: 4.26–7.78), LR– was 0.29 (95% CI: 0.23–0.36), DOR was 21.42 (95% CI, 13.61–33.73), and AUC was 0.8871. For CEUS, the pooled SEN and SPE were 0.87 (95% CI: 0.82–0.91) and 0.86 (95% CI: 0.82–0.89), respectively, LR+ was 5.92 (95% CI: 4.21–8.33), LR– was 0.16 (95% CI: 0.11–0.25), DOR was 38.27 (95% CI: 18.73–78.17), and AUC was 0.9210.
CONCLUSIONS:
Adding CEUS and (or) SMI to conventional US could improve its diagnostic performance in differentiating benign from malignant solid breast lesions.
Introduction
Breast cancer is the most common malignant tumor in women worldwide [1]. Early diagnosis and treatment can significantly improve the survival rate and prolong the disease-free survival time. Ultrasound (US) is an important diagnostic tool widely used in clinical settings. The emergence of new US techniques, such as ultrasonic elastography, contrast-enhanced US (CEUS), and superb microvascular imaging (SMI), can improve the diagnostic efficiency of US in differentiating between breast lesions [2, 3]. Conventional US uses the breast imaging report and data system (BI-RADS) lexicon developed by the American College of Radiology (ACR) in 2013 to guide US diagnosis in describing the ultrasonic signs of breast lesions. It is widely used and provides a standardized explanation for the determination of treatment recommendations. The BI-RADS dictionary contains a detailed description of the morphological features of US, but lacks the description of vascular features. According to the BI-RADS score, the vascular morphology and distribution of solid breast masses were closely related to their properties [4, 5]. Conventional Doppler imaging with Adler classification improves the value of US in the diagnosis of breast lesions [6]. However, its disadvantage is that it is not sensitive to small containers (diameter < 200 mm). CEUS could clearly display the microvessels (7–10 um) in the lesion by using the harmonic technique and lipid microbubbles. The vascular perfusion pattern was observed and the time-intensity curve was recorded by analysis software, and the related parameters were obtained [7]. SMI (Toshiba Medical Systems, Tokyo, Japan) applies a multi-dimensional filter to effectively separate low-flow signals from overlaying tissue motion artifacts, preserving even the subtlest low-flow components with unmatched detail and definition, which provides high-resolution details of vascular branches, evaluates the vascular index (VI) and vascular configuration (VA) of the breast lesions in monochromatic and color modes [8, 9], and makes semi-quantitative and qualitative diagnoses [10]. The two techniques have excellent ability to detect more microvessels and describe their morphological details. Different studies have investigated the application of CEUS and SMI in the diagnosis of breast lesions, and have concluded that CEUS and SMI are very effective in the diagnosis of breast lesions. However, recent studies have not directly compared the two technologies or pooled them in different ways [11–13]. Therefore, it is necessary to review the literatures in order to provide substantial evidence for their clinical application. The Cochrane team developed a meta-analysis of diagnostic test accuracy (DTA) to summarize and compare the accuracy of the tests. This study aims to summarize the benefits of merging the two methods and compares the diagnostic effectiveness of SMI and CEUS.
Methods
This study did not require the approval of the institutional review committee, as the study type does not require approval in the author’s institution.
Search strategy
We searched PubMed, EMBASE, Web of Science, Chinese national knowledge infrastructure databases, Chinese biomedical literature databases, and Wanfang for relevant studies published between November 2015 and November 2021. The references of the articles were also retrieved manually. The search strategy included the following terms: (“enhanced ultrasound” or “CEUS”) combination (“breast”) and (“SMI” or “microflow imaging”) combination (“breast”). Two examiners searched the databases to obtain original data; any differences in opinion were resolved mutually through discussion.
Eligibility criteria
Studies were included in this meta-analysis if they fulfilled the following criteria: (1) studies on the diagnostic performance of SMI and CEUS; (2) studies providing true positive (TP), false positive (FP), false negative (FN), true negative (TN) results or key information for calculation; and (3) the breast lesions were obtained by surgery or biopsy and were identified by histopathological examination.
Data extraction and quality assessment
Eligible full-text study data were extracted by two researchers (Z.Y. and G.X.F). Disagreements were resolved through discussion and consensus. The following data were collected: first author, year of publication, number of patients, number of lesions, mean age, lesion diameter, CEUS, diagnostic criteria, diagnostic thresholds, TP, FP, TN, FN, and a QUADAS-2 score for the literature.The QUADAS scoring tool was used to assess the quality of the studies included in this meta-analysis and the assessment was performed by two independent investigators (L.J.J. and G.Q.). Each trial was rated as high risk, low risk, or unclear risk. Bias was rated based on the following aspects: patient selection, indicator test reference, standard procedure, and timing; each was rated as: yes (1 point), no (–1 point), or unclear (0 points).
Statistical analyses
Cochran’s Q test and Higgins I-squared statistic were applied to evaluate the heterogeneity among the studies. Heterogeneity was defined as p < 0.10 or I2 > 50% [14], and a random-effects model (DerSimonian–Laird method) was used as the pooling method if heterogeneity existed [15]. Otherwise, the fixed-effects model (Mantel–Haenszel method) was applied. Subgroup analyses were performed based on contrast dose assessment method and patient’s age. Heterogeneity due to a threshold effect was tested using visual assessment and the calculation of the Spearman correlation coefficient. The existence of a typical shoulder-arm pattern and a Spearman correlation coefficient of > 0.6 were considered as the presence of the threshold effect. The pooled estimates of SEN and SPE were summarized using bivariate modelling and hierarchical summary receiver operating characteristic modelling. The test accuracy was assessed using meta-regression by adding test type as a covariate in a hierarchical model, for which the Cochrane Collaboration was recommended. Deeks’ funnel plot and Deeks’ asymmetry test were used to assess publication bias. All of the p-values were two-sided, with p > 0.05 considered statistically significant. All analyses were performed using Meta-Disc version 1.4 and Stata version 16.0 (Stata Corp, Madrid, Spain).
Results
Literature search
As shown in Fig. 1, an initial search yielded 200 records, with four reviews from the referenced literature. Twenty-one records were excluded after removing duplicates and 179 records were excluded after screening titles and abstracts. Eight articles were identified as eligible for inclusion. After reviewing the full text, two studies were removed because the authors compared the added value of CEUS with shear wave elastography (SWE) conventional US, and one study was removed because the authors compared the added value of SMI with SWE conventional US. Finally, five studies from five articles were considered for this meta-analysis.
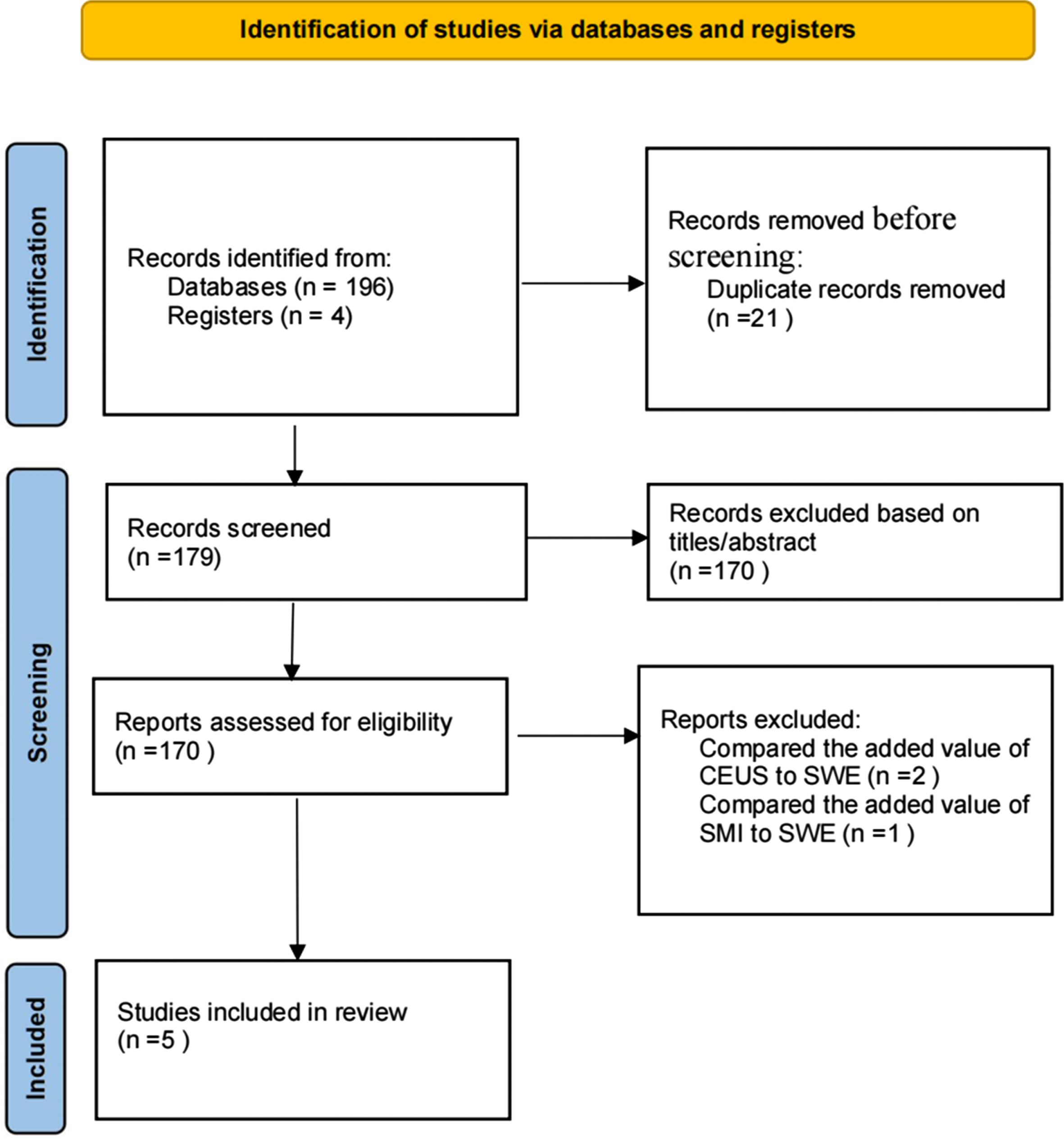
Flow diagram of study selection.
Details of the eligible studies are summarized in Table 1. All of these studies were diagnostic studies published from 2016 to 2020 and provided sufficient information for the calculation of TP, FP, FN, and TN. In all five studies, the diagnostic performance of SMI and CEUS was compared. All studies used SonoVue (Bracco, Milan, Italy) as the contrast agent; in four of these studies, a dose of 4.8 ml was used, and in one study, a dose of 3.6 ml was used. All studies included women with a mean age of 40–55 years, and a total of 530 patients and 553 lesions were included in the meta-analysis; 238 (43.04%) lesions were malignant and 315 (56.96%) were benign.
Characteristics of included studies
Characteristics of included studies
aVascular Patterms.
The quality of the included studies was evaluated as shown in Table 2. All included studies met the index trial criteria and used pathological evaluation as a reference standard; four studies were blinded to US examiners for pathological findings. In terms of patient selection bias, four of the five studies were low risk. One study reported that they excluded three patients because of unsatisfactory images, which was considered to be a potential source of bias. Overall, none of the five studies were excluded from the meta-analysis because of methodological flaws.
Quality assessment of the included studies using QUADAS-2 tool
Quality assessment of the included studies using QUADAS-2 tool
Key: +, low risk; –, high risk; ?, unclear risk.
Results of subgroup analyses
The pooled SEN and SPE of SMI for the diagnosis of breast lesions obtained from the preliminary analysis were 0.75 (95% CI: 0.69–0.91) and 0.88 (95% CI: 0.83–0.91), respectively; SEN (I2 = 0.0%, p = 0.4604) and SPE (I2 = 0.0%, p = 0.4535), with no heterogeneity; pooled LR+ of 5.75 (95% CI: 4.26–7.78) and pooled LR– of 0.29 (95% CI: 0.23–0.36) (Fig. 2). The pooled SEN and SPE of CEUS for the diagnosis of breast lesions were 0.87 (95% CI: 0.82–0.91) and 0.86 (95% CI: 0.82–0.89), respectively; SEN (I2 = 17.5%, p = 0.3033) and SPE (I2 = 0.0%, p = 0.4430) with no heterogeneity; LR+ 5.92 (95% CI: 4.21–8.33) and LR– 0.16 (95% CI: 0.11–0.25) (Fig. 3). DOR of SMI was 21.42 (95% CI: 13.61–33.73) with AUC 0.8871 and a Q* value of 0.8177; DOR of CEUS was 38.27 (95% CI: 18.73–78.17) with AUC 0.9210 and a Q* value of 0.8546 (Fig. 4).
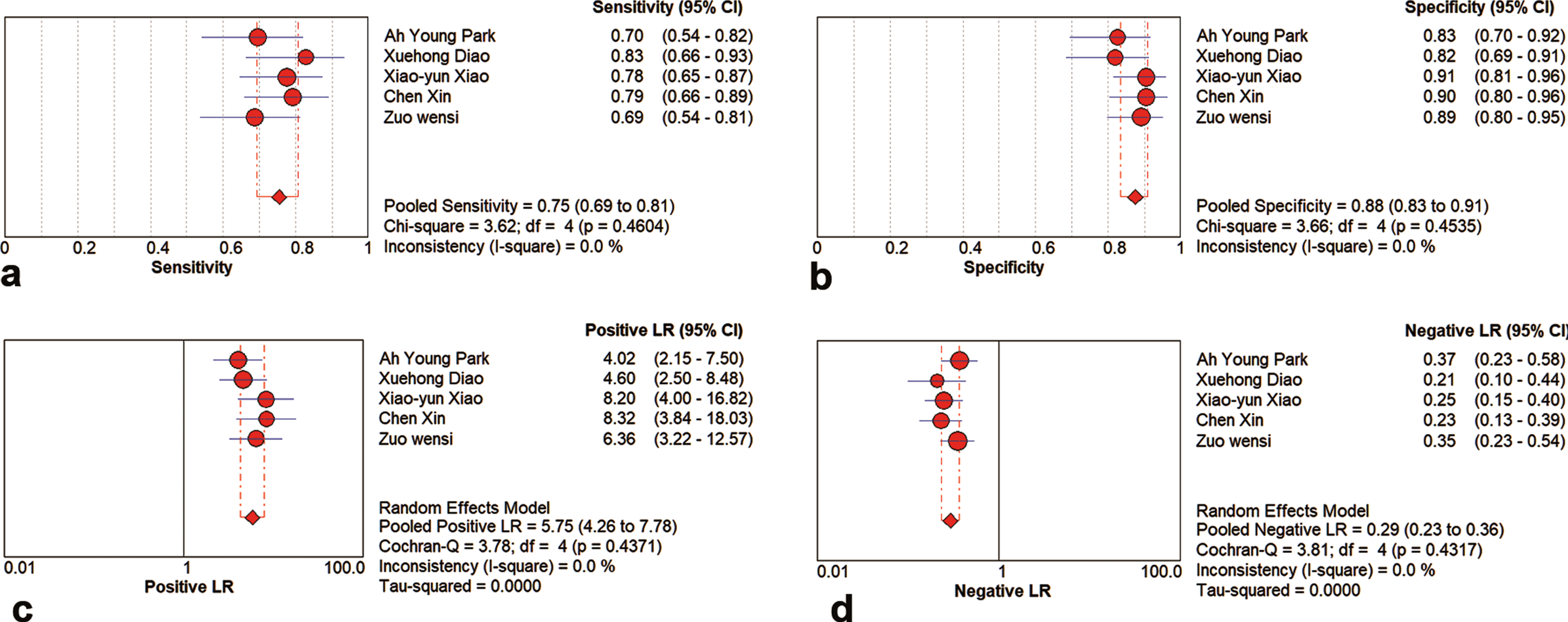
Forest plot for a: Sensitivity, b: specificity, c: PLR, d: NLR of eligible studies using SMI.
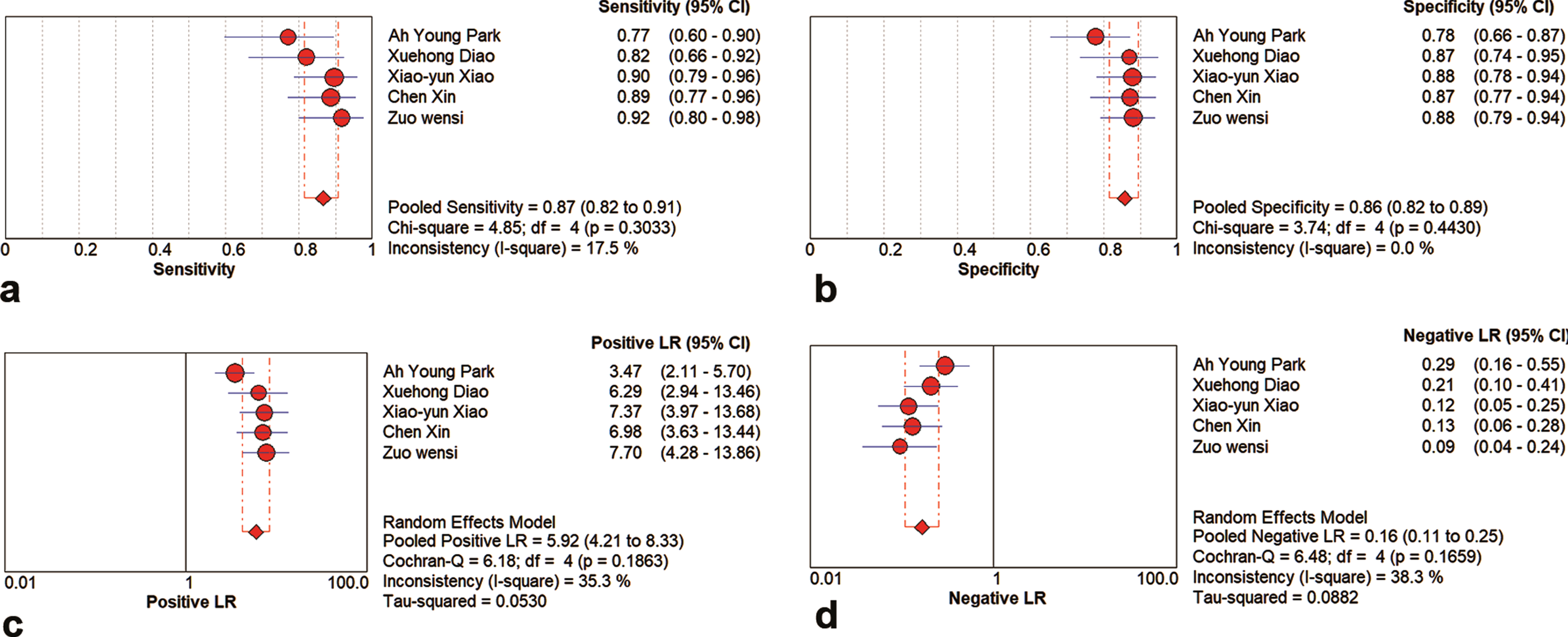
Forest plot for a: Sensitivity, b: specificity, c: PLR, d: NLR of eligible studies using CEUS.

DOR and SROC curves of using CEUS and SMI for breast lesions. a: DOR of using SMI for breast mesions, b: DOR of using CEUS for breast lesions, c: SROC curves of using SMI for breast lesions, d: SROC curves of using CEUS for breast lesions.
Pooled AUC and 95 % CI after omitting each trial in the meta-analysis (sensitivity analysis)
The differences in SEN and SPE between the two diagnostic methods, SMI and CEUS, and AUC were not statistically significant (p < 0.05).
In this meta-analysis, the results of the five studies we included clearly show that the addition of CEUS and SMI to conventional US BI-RADS classification can improve the ability of US to distinguish solid breast lesions. A meta-analysis of 1545 patients and 1609 breast masses showed the accuracy of CEUS in the diagnosis of breast lesions. The pooled SEN and SPE were 0.93 (95% CI: 0.91–0.95) and 0.86 (95% CI: 0.84–0.88), respectively. The pooled LR+ and LR were 6.43 (95% CI: 5.14–8.04) and 0.07 (95% CI: 0.03) [16]. In a meta-analysis of 15 studies, SMI estimated that in 955 patients with malignant breast lesions and 1116 patients with benign breast lesions, the pooled SEN and SPE were 0.81 (95% CI: 0.78–0.83) and 0.71 (95% CI: 0.68–0.73), respectively; the pooled LR+ was 3.24 (95% CI: 2.27–4.64) and the pooled LR– was 0.25 (95% CI: 0.18–0.34), whereas the AUC was 0.87 (95% CI: 0.84–0.90) [17]. All the above studies are consistent with the conclusions of this meta-collection.
In this meta-analysis, subgroup analysis was carried out according to different age groups and contrast doses. The age group, different diagnostic cut-off points of benign and malignant lesions, and dose of the contrast agent did not play an important role in the production of heterogeneity for the conventional SMI- or CEUS-related US methods. There is a certain heterogeneity in the diagnosis of different benign and malignant lesions. Previous studies have found that different patterns of CEUS enhancement can lead to a high degree of heterogeneity. The contrast medium qualitatively and quantitatively analyzed the changes of blood perfusion in the region of interest [7, 18]. The benign lesions were usually the same size as the grayscale image, with uniform centripetal enhancement mode, clear boundary, and regular shape. The malignant lesion image is usually larger than the grayscale image, the enhancement order is centrifugal, the edge has no boundary, is crab-shaped, has perfusion defects, and penetrates the blood vessels. The enhancement degree of malignant lesions was significantly higher than that of benign lesions and the enhancement speed was faster. However, different contrast agent doses, US machines and analysis software, inconsistency among observers, and the proportion of different pathological types included in the study of breast cancer can lead to a high degree of heterogeneity in the study [19, 20]. In previous studies, the microvascular morphology of breast tumors on SMI was divided into nonvascular patterns, linear-like patterns, dendritic patterns, root hair-like patterns, and crab claw-like patterns. The first three are common in benign lesions, and the latter two are common in malignant lesions [10, 21]. When root hair-like and crab-claw-like blood flow patterns are used as diagnostic criteria for malignant tumors, SMI and CEUS have similar diagnostic ability. Studies have shown that increasing blood flow patterns in conventional US BI-RADS classification can reduce heterogeneity. Thus, when analyzing the main position of BI-RADS in breast diagnosis, CEUS and SMI techniques can be used to add value, but cannot replace BI-RADS entirely [22].
In this meta-analysis, it was found that the ultrasonic BI-RADS classification with CEUS and SMI has high SEN and SPE, which can provide more guidance for clinical work. However, some limitations were observed: (1) in the inclusion study, CEUS and SMI were added to conventional US, using their own standard additions, or only the malignant characteristics of CEUS and SMI were used for diagnosis, which could have led to a high degree of heterogeneity [22]; (2) lesion size is an important part of the study, but the studies included in this meta-analysis had major differences in the definition and data on lesion size; hence, it was impossible to carry out a quantitative or subgroup analysis. However, some studies have confirmed that SMI technology can make a more accurate diagnosis of small breast cancer [23]; (3) the use of BI-RADS 4a or CEUS and / or SMI malignant vascular features as the diagnostic cutoff point has an important impact on the diagnostic performance, and a unified diagnostic cutoff point is helpful to compare with other literature; (4) CEUS has contraindications when evaluating pregnant women, breast-feeding women, and patients with cardiopulmonary insufficiency. Moreover, CEUS needs an intravenous contrast medium. SMI has no contraindications, does not need contrast agent, and allows multi-angle observation of single focus and multiple lesions. From the simplicity of operation, SMI is more suitable for daily use [13], but the two techniques lack consensus on acquisition techniques and interpretation methods.
Some studies have discussed the correlation between ultrasonic BI-RADS signs and the molecular subtypes of breast cancer, but the conclusion is not clear [20, 25]. The evaluation of intratumoral blood flow with the US imaging parameters of CEUS and SMI not only improves the diagnostic efficiency of US, but also changes the US evaluation of breast cancer from a level of simple morphology to a more functional level, and even can be compared with the application of enhanced magnetic resonance imaging in the diagnosis and treatment of breast cancer, which is of great clinical significance. However, further studies are needed to verify its significance [26, 27].
Conclusion
The addition of CEUS and / or SMI on the basis of the conventional USBI-RADS classification can improve the diagnostic efficiency of US in the differential diagnosis of solid breast lesions. However, further large-scale research is needed to standardize image acquisition and interpretation methods of these two US techniques and to reach a consensus with the clinical diagnostic criteria of breast cancer.
Footnotes
Acknowledgments
This study was supported by the Wuhan Central Hospital Research Project.