
Abstract
AIM:
To evaluate the additive clinical value of endoluminal contrast enhanced ultrasound (CEUS) after interventional placement of drainages in abdominal fluid collections.
MATERIAL/METHOD:
Examination of 30 patients using a 1–6 MHz convex probe (Resona 7, Mindray) to locate the fluid collection in B-Mode. Additionally, dynamic endoluminal CEUS with 1 ml sulphur-hexafluoride microbubbles was performed to measure the extent of the percutaneously drained abscesses. Independent assessment of dynamically stored images in PACS in DICOM format. Correlation to reference imaging using computed tomography (CT).
RESULTS:
A total of 30 patients were examined (17 m, 19–78 years, mean 56.1 years). Drainages were positioned in the liver in 15 cases, in the pelvis after kidney transplantation in 4 cases, close to the spleen in 1 case, and in the abdomen in 10 cases. In all cases abscesses showed marginal hyperaemia with reactive septations in CEUS. The drainage position was assessed by means of B-mode in all cases first and then by CEUS. In 4 cases CEUS showed a fistula to the pleura, in 5 cases to the peritoneum, in 2 cases to the intestine, in 5 cases to the biliary tract, corresponding to the CT. In 2 cases there was a hint of an anastomotic leakage after intestinal anastomosis, which was reliably detected by CT. The drainage was removed in 11 cases within a period of 2 to 5 days after CEUS control, in 9 cases within a period of 5 to 10 days. Another operation was necessary in 3 cases. A new drainage was placed in 2 cases. The required amount of ultrasound contrast medium is 1 ml endoluminally diluted to 9 ml sodium chloride.
CONCLUSION:
CEUS facilitates the exact localization and characterization of inflammatory abdominal fluid collections. Furthermore, possible fistulas can be detected that cannot be seen with conventional ultrasound.
Keywords
Introduction
Inflammatory fluid collections and abscesses in the abdomen are frequent complications in infectious and post-operative patients. If untreated the hospitalisation of patients is prolonged and it might result in serious deterioration of the patient's health or might even be fatal [1]. Especially in post-operative patients, a percutaneous drainage is the therapy of choice in inflammatory fluid collections since it has proven to be safe and effective as well as less traumatic than a re-operation [2].
CEUS offers many possibilities to assess inflammatory processes and micro-circulation [3–5]. CEUS can also be used as an imaging guiding method for interventions and is mostly used for percutaneous ablations for liver tumors [6, 7]. It can also be used intraoperatively for diagnostics and image-guided ablations [8, 9]. Additionally, CEUS can be used for percutaneous drainage placement in inflammatory fluid collections. However, according to the EFSUMB guidelines for non-hepatic applications, CEUS for follow-up of inflammatory fluid collections is still deemed off-label use [10]. The importance of CEUS has been shown for inflammatory processes and changes of the biliary system. The dynamic quantification of CEUS is especially important for inflammatory conglomerates in inflammatory bowel disease [11].
Fluid collections can either be displayed with contrast-enhanced CT or with ultrasound diagnostics and various therapeutic measures can be monitored in the course of the process. Abscesses typically show air pockets and hyperaemia in the marginal area. They can also appear cystic in B- Mode imaging. Color Coded Doppler Sonography (CCDS), can detect the marginal hyperaemia with different colors.
Ultrasound is widely available around the world, does not apply radiation, is fast and painless. Furthermore, ultrasound offers real time bedside imaging, so critically-ill patients do not have to be transferred for imaging. Thus, ultrasound opens the possibility of real-time ultrasound-guided interventions and their follow-up monitoring.
With ultrasound, the drainage can also be introduced into the collections in a targeted manner. Alternatively, the drainage system can also be placed using computed tomography with fluoroscopy. Studies have already been published about the usefulness of diluted contrast media in the follow-up of percutaneously placed drainages in CT [12]. However, only a little has been published about CEUS in drainage placement [13, 14].
The aim of this study was to evaluate the additive clinical value of endoluminal contrast enhanced ultrasound (CEUS) after interventional placement of drainages in abdominal fluid collections.
Material and methods
This retrospective study was waived by the local ethical committee. The patients were transferred to the Department of Radiology or the Interdisciplinary Department for Ultrasound from any of the wards at a maximum care hospital.
The patients then either received a contrast-enhanced abdominal CT in portal venous phase (Siemens Flash, 70 ml Accupaque® 350 i.v) or conventional ultrasound (Resona 7, Mindray). If fluid collections were found, an interdisciplinary consensus on the treatment was formed with the referring physician. If a drainage was indicated the patient’s written informed consent was obtained whenever possible. In intubated patients on ICU the written informed consent of the respective caretaker was obtained. All drainages in CT and by ultrasound guidance were placed using the Seldinger technique.
All ultrasound examinations were carried out on a high-performance ultrasound device (Resona 7, Mindray) and carried out by an experienced examiner (more than 3000 examinations for more than 20 years). The abdominal fluid collections were scanned with a convex probe (SC 6-1 U with 1–6 MHz), if necessary superficial abscesses were scanned with a linear probe (L 9-3 U with 3–9 MHz) and measured in three planes. The extent of the drained collection and the collection that has yet to be drained was shown in the picture and measured in three planes as well. A possible hypervascularization in the marginal area was assessed with CCDS. In addition, possible vascular changes and thromboses were taken into account as well as fistulas and other complications arising from the inflammation.
For the exact drainage assessment, CEUS was then performed dynamically with a contrast-media injection into the drainage. For this purpose, 1 ml of sulphur hexafluoride microbubbles (SonoVue®, Bracco, Milan/ Italy) diluted with 9 ml sodium chloride was injected into the drainage. There was continuous documentation with Cine Loops recording the spread of the microbubbles in the drainage and the remaining abscess. The abscess was then measured again in three planes. In addition, particular attention was paid to the spread of the microbubbles into adjacent structures such as bile ducts, the intestines or vascular structures as a hint for fistulas. The findings were documented digitally in PACS (picture archiving and communication system). The retrospective reading was performed by two radiologists in consensus.
Results
The drainages were placed in CT in 13 cases and with ultrasound guidance in 17 cases. No complications occurred due to the drainage placement. Drainages were positioned in the liver in 15 cases, in the pelvis after kidney transplantation in 4 cases, close to the spleen in 1 case, and in the abdomen in 10 cases. The drainage position was assessed by means of B-mode in all cases first and then by CEUS. In all cases abscesses showed marginal hyperaemia with reactive septations in CEUS. In 4 cases CEUS showed a fistula to the pleura, in 2 cases to the intestine, in 5 cases to the biliary tract. Those fistulas could also be seen in the subsequent CT. In 2 cases there was a hint of an anastomotic leakage after intestinal anastomosis, which was reliably detected by CT. The drainage was removed in 11 cases within a period of 2 to 5 days after CEUS control, in 9 cases within a period of 5 to 10 days. Another operation was necessary in 3 cases. A new drainage was placed in 2 cases. The required amount of contrast medium is 1 ml endoluminally diluted to 9 ml sodium chloride. Drainages between 6–12 F were used. No contrast-media intolerances were noted. No iatrogenic SIRS (systemic inflammatory response syndrome) was documented caused by the flushing of the drainage. The fistulas could not be seen in B-Mode and were only seen on CEUS (Table 1).
Sex and age of the patients. Localisation of the drainage placement, method of placement. Size of drainage and complications seen on CEUS during the follow-up. Comparison between size in CT, B-Mode and CEUS. (TX = Transplantation)
Sex and age of the patients. Localisation of the drainage placement, method of placement. Size of drainage and complications seen on CEUS during the follow-up. Comparison between size in CT, B-Mode and CEUS. (TX = Transplantation)
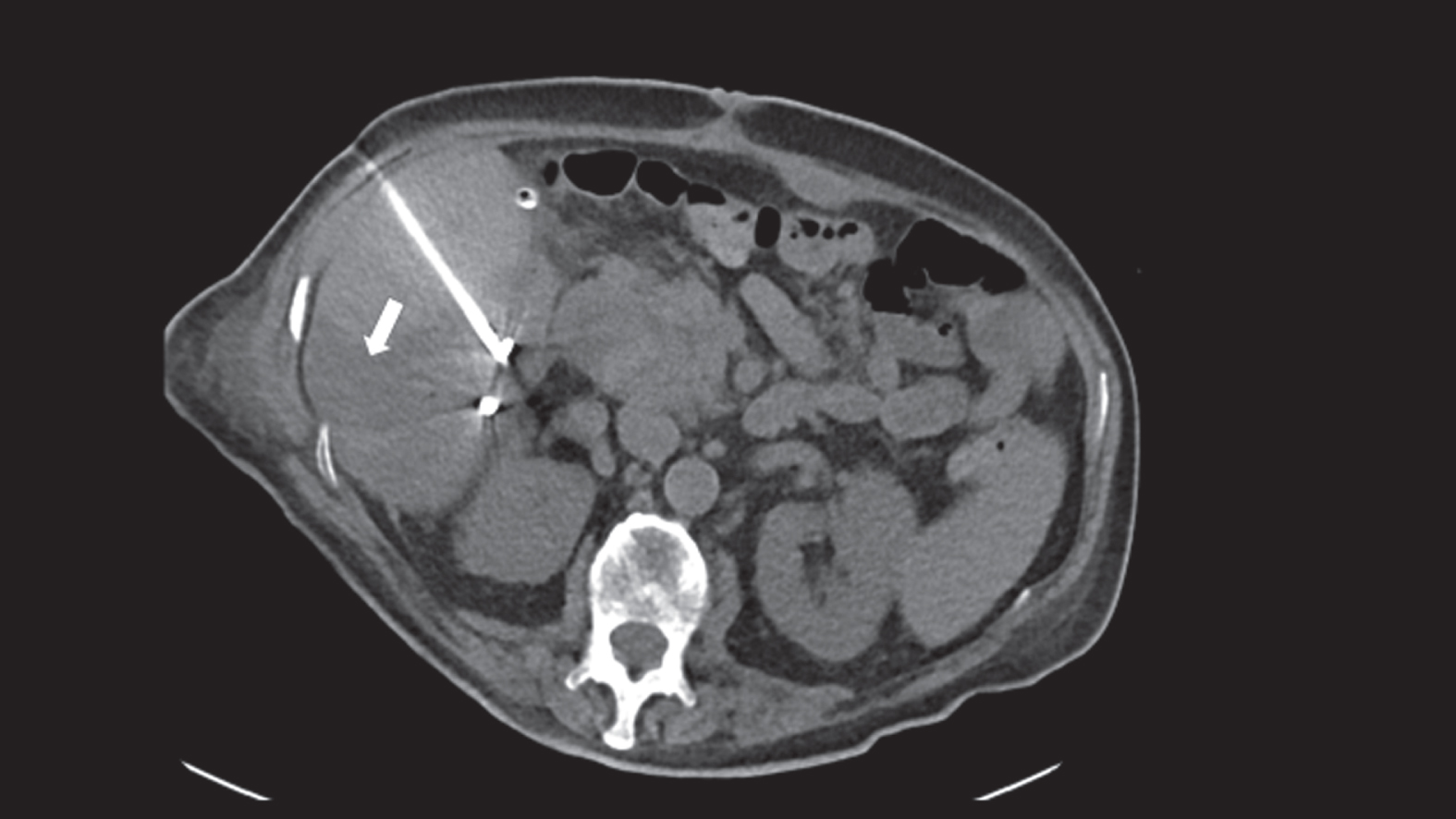
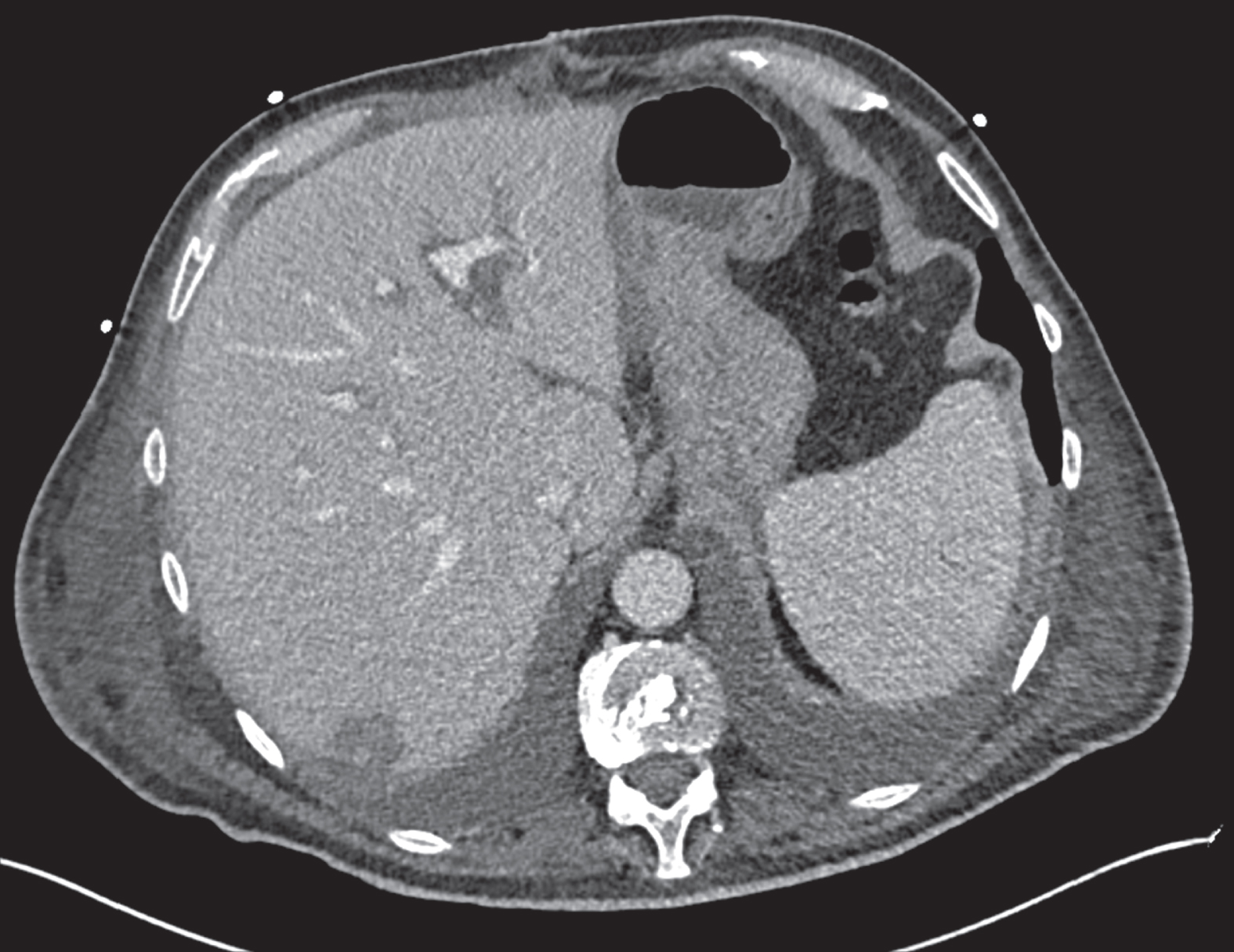
Transhepatic CT-guided drainage placement into the perihepatic inflammatory fluid collection.
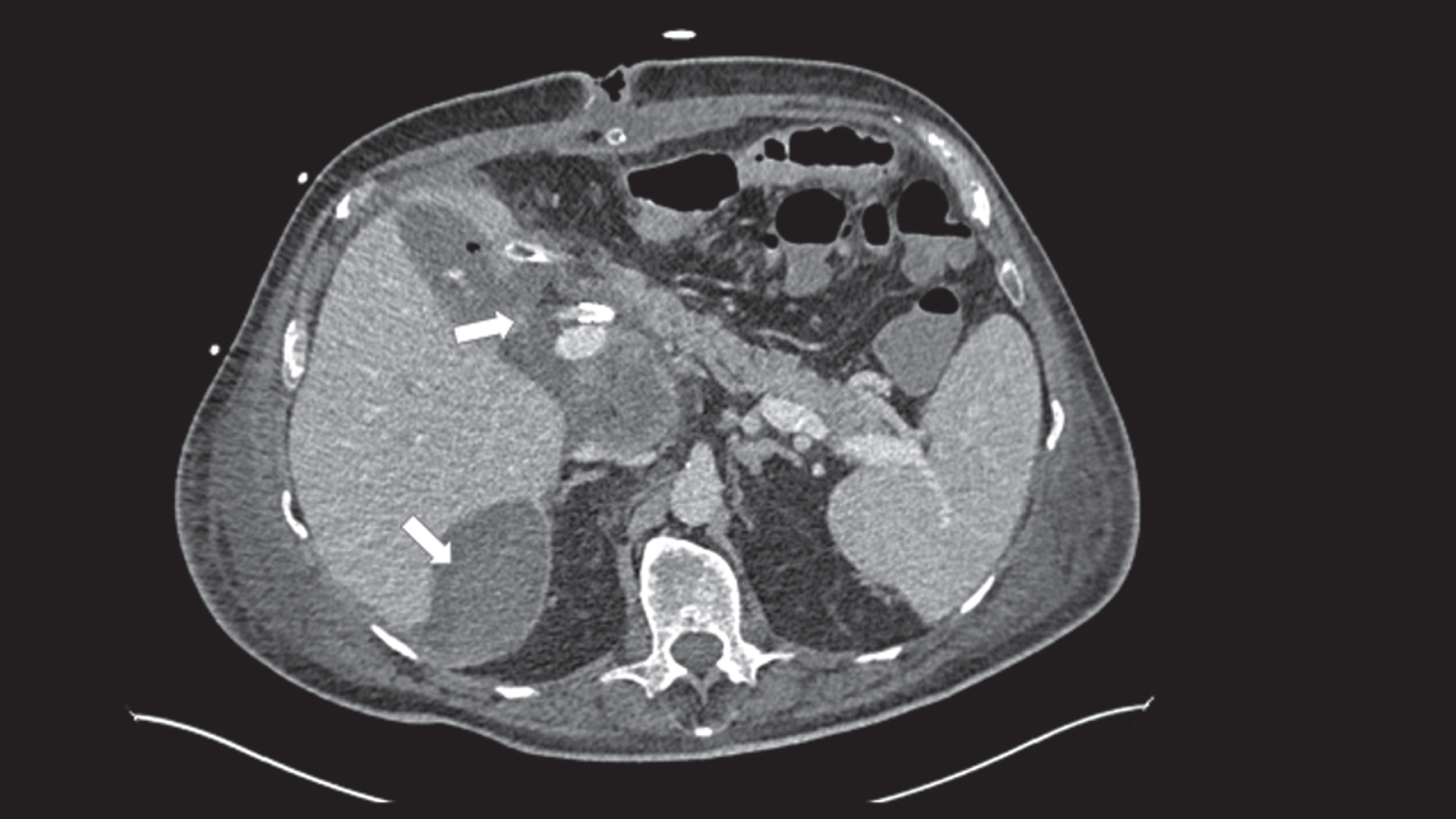
CT scan of the liquid perihepatic formation as well as an intrahepatic fluid collection after drainage.
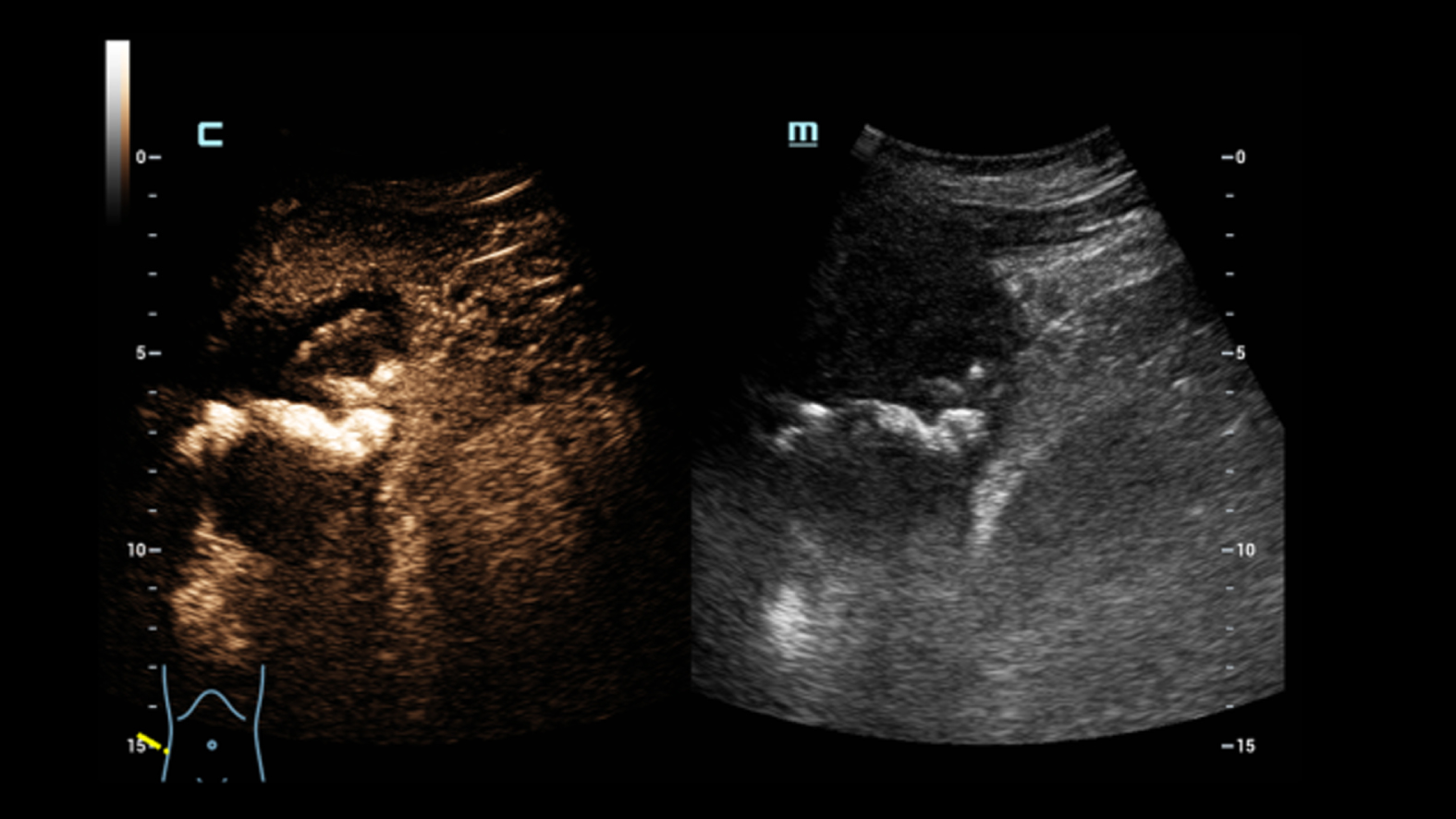
Flushing of the drainage with 1 ml sulfur hexafluoride microbubbles diluted with 9 ml sodium chloride with sterile conditions and intravenous application of 1 ml ultrasound contrast media for assessment of the liver parenchyma (Figure 1 c, d and e). No leakage into the peritoneal cavity visible. The inflammatory formations are decreasing (white arrow in axial portal venous CT (Figure 1f) and CEUS, (Figure g)) and there is only a little serous fluid collection adjacent to the diaphragm (visible on CEUS). No penetration of the bubbles visible. In the follow-up CT control 2 months after the drainage placement, the abscesses have completely disappeared (Figure 1h, coronal and axial reformations in portal venous phase).
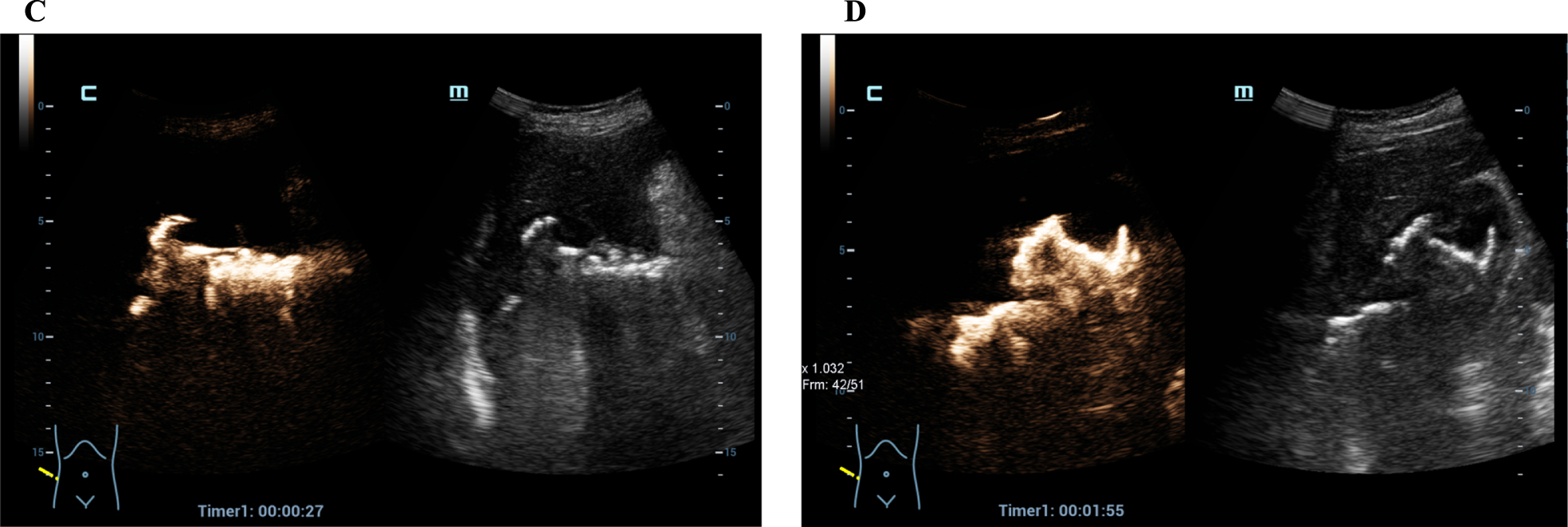
Dynamic assessment of the inflammatory fluid collection using endoluminal CEUS for the follow up after percutaneous drainage.
Endoluminal CEUS of the drainage and intravenous CEUS of the liver for detection and evaluation of the perihepatic fluid collection. No leakage into the peritoneal cavity visible.
No leakage into the peritoneal cavity visible and decreasing inflammation (CT).
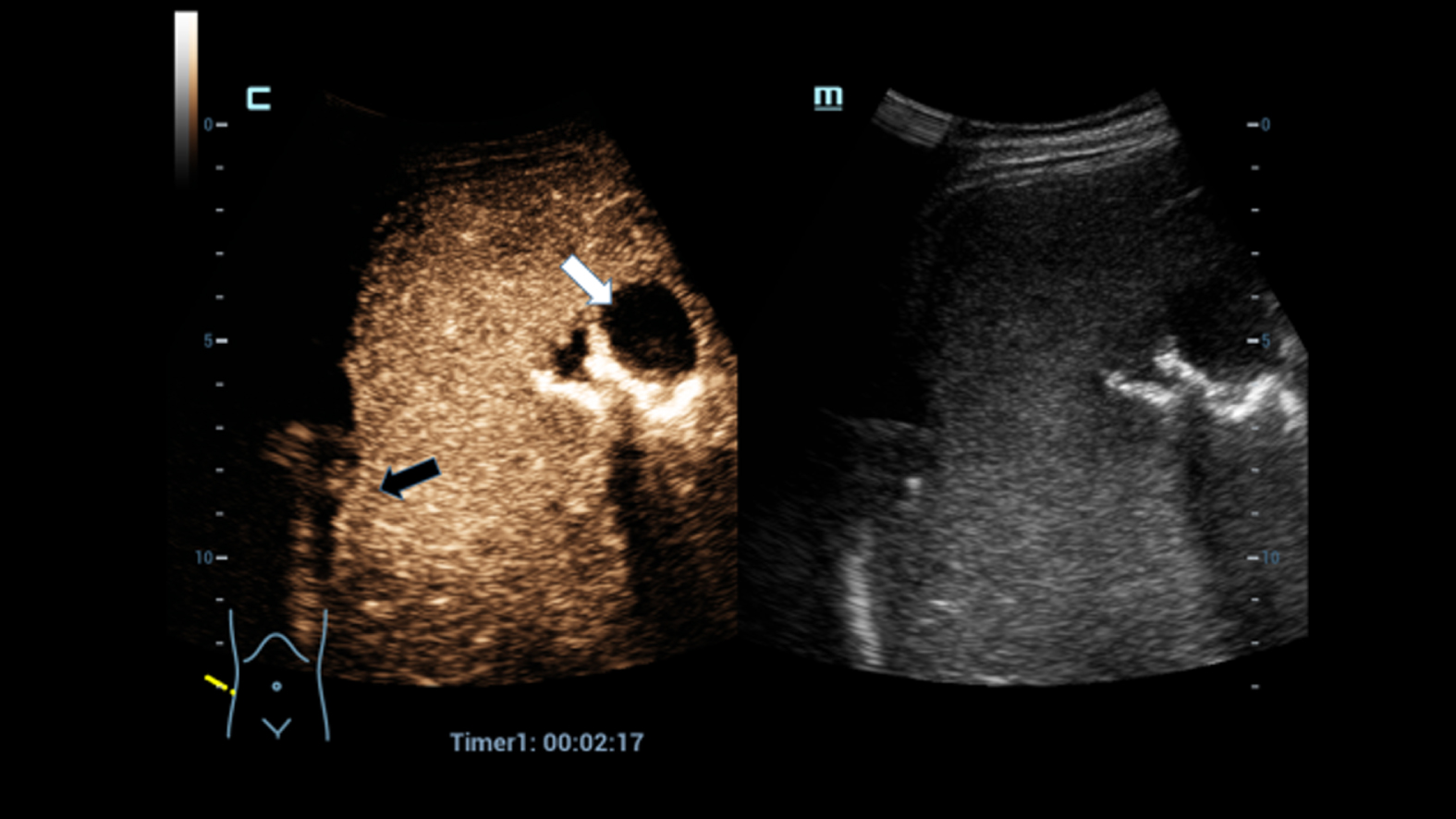
No leakage into the peritoneal cavity visible and decreasing inflammation (CEUS).
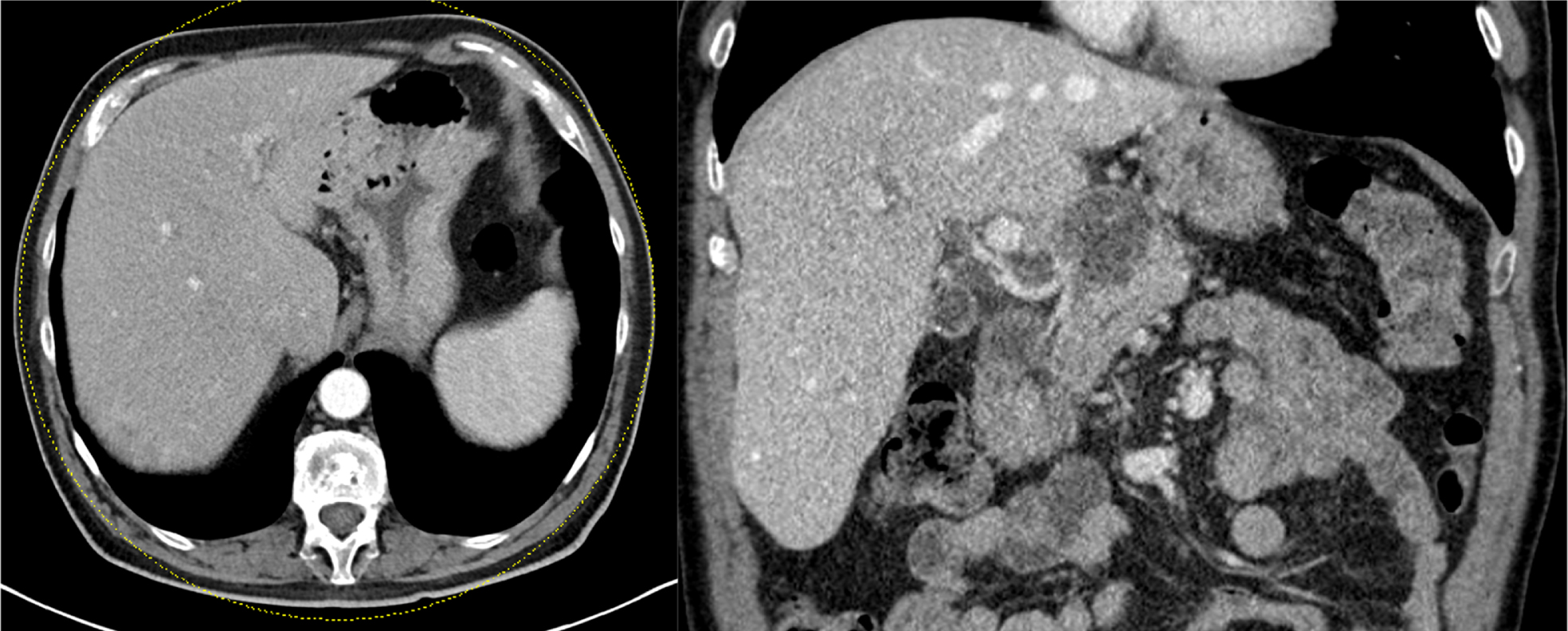
Follow-up CT control 2 months after the drainage placement, the abscesses have completely disappeared.
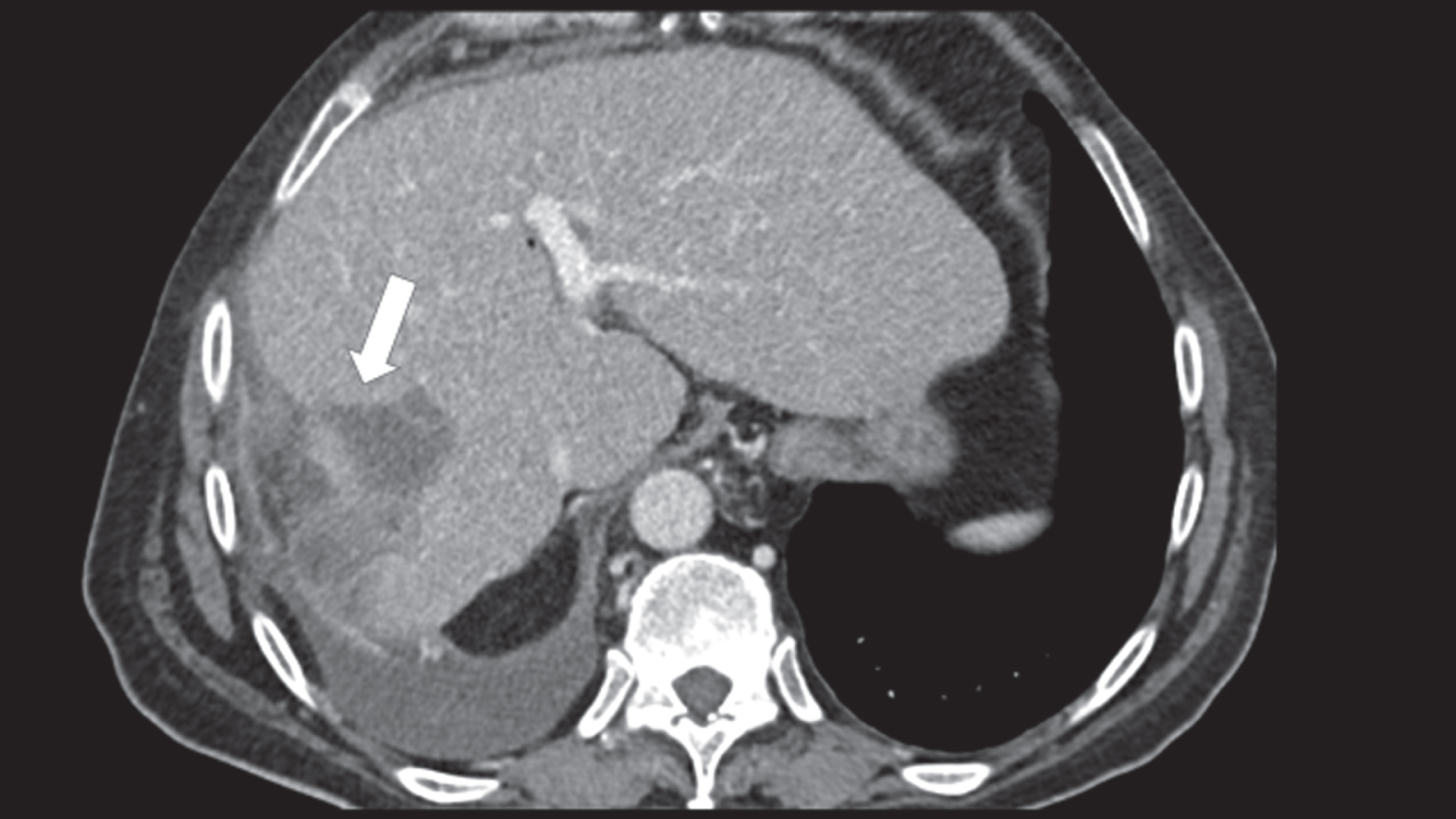
Intrahepatic inflammatory fluid collection on the rhigt liver lobe (arrow) detected by contrast enhanced CT scan.
Status post transarterial chemoembolization in segment VI and VII. CT shows biliomas (white arrow) and pleural effusion on the right side.
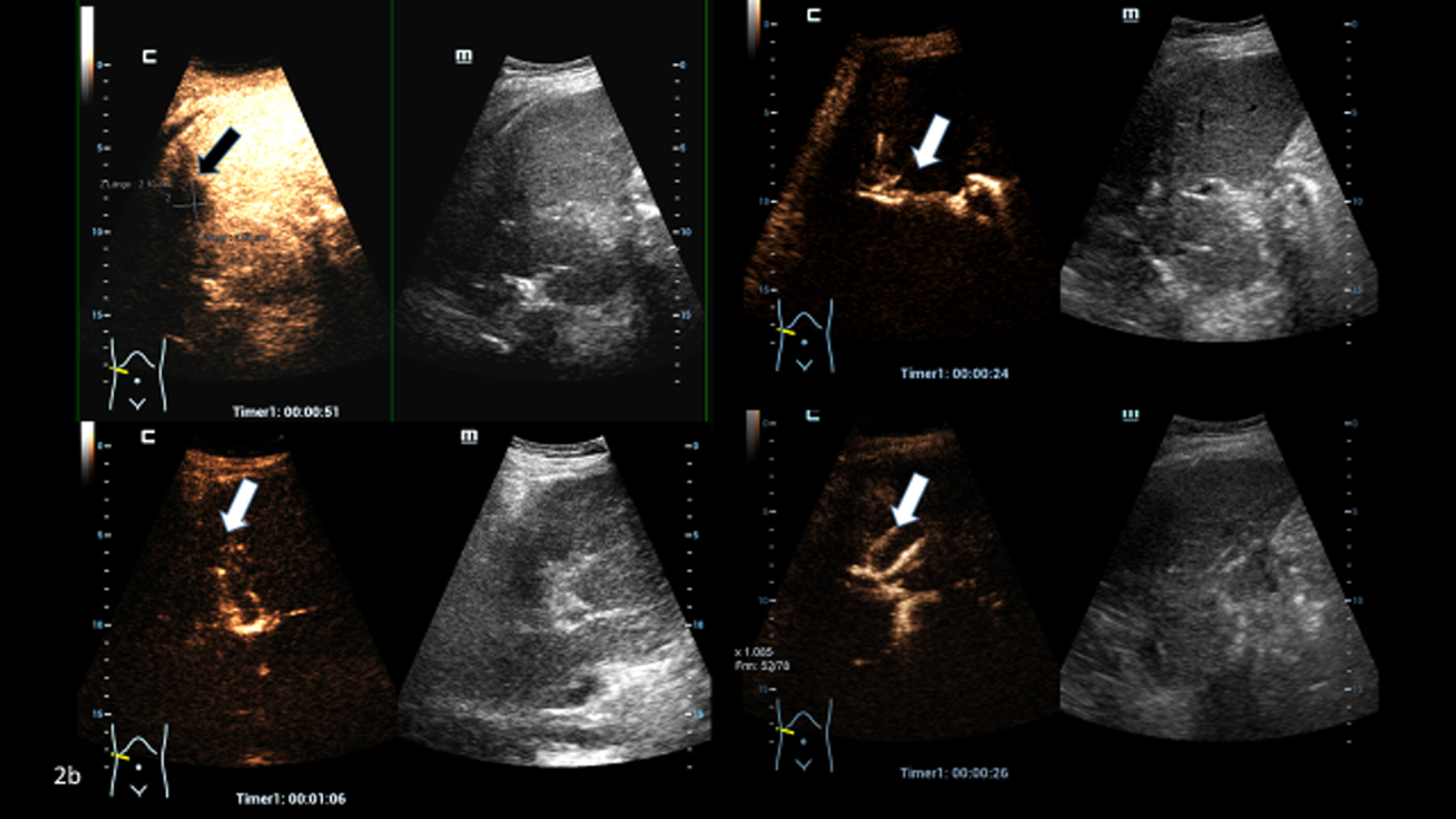
After application of 1 ml ultrasound contrast media diluted with 9 ml sodium chloride the biliary tracts are shown (arrow).
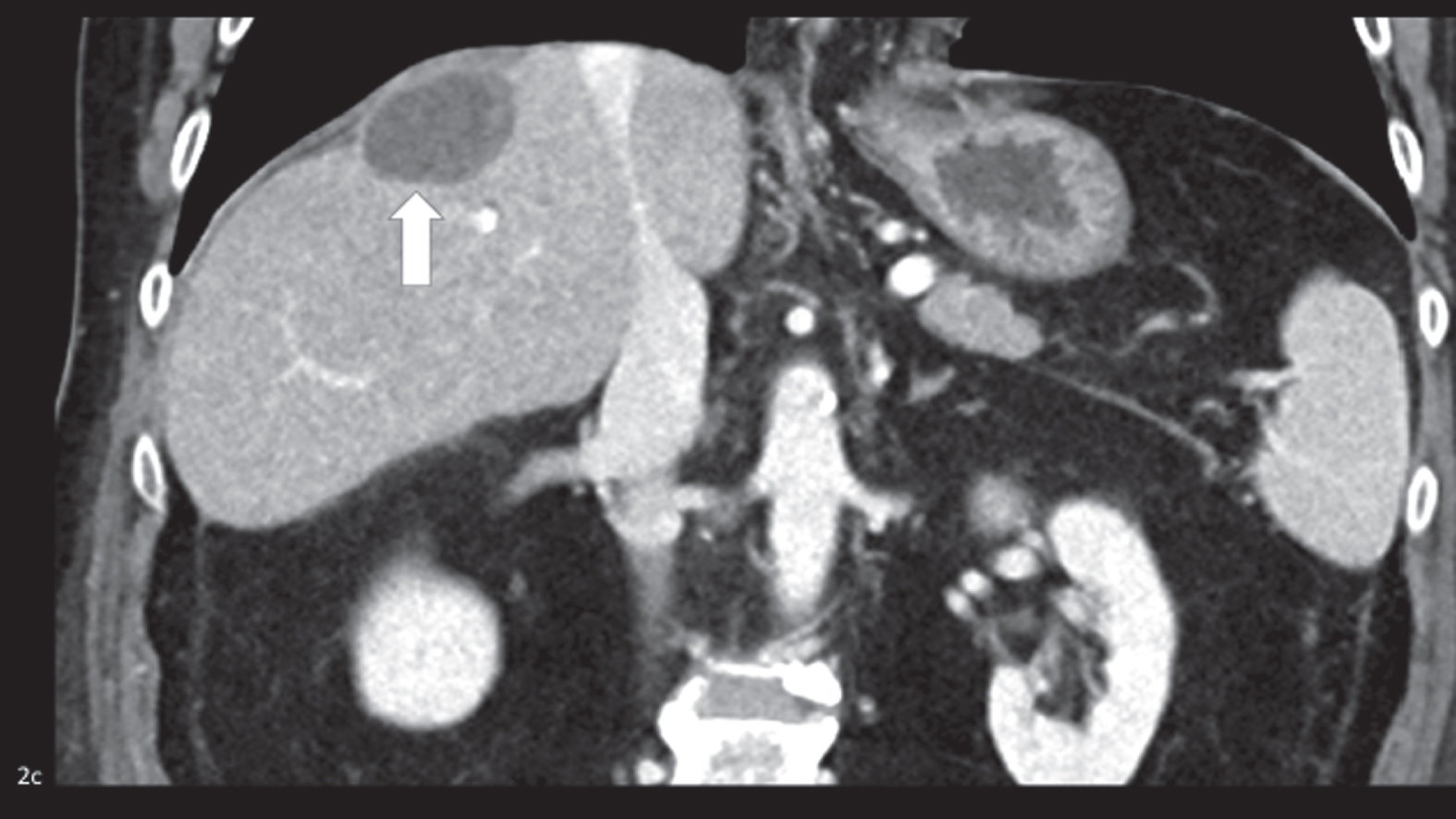
CT shows a remaining avascular post ablation cystic defect in segment VII black arrow, Figure 2c).
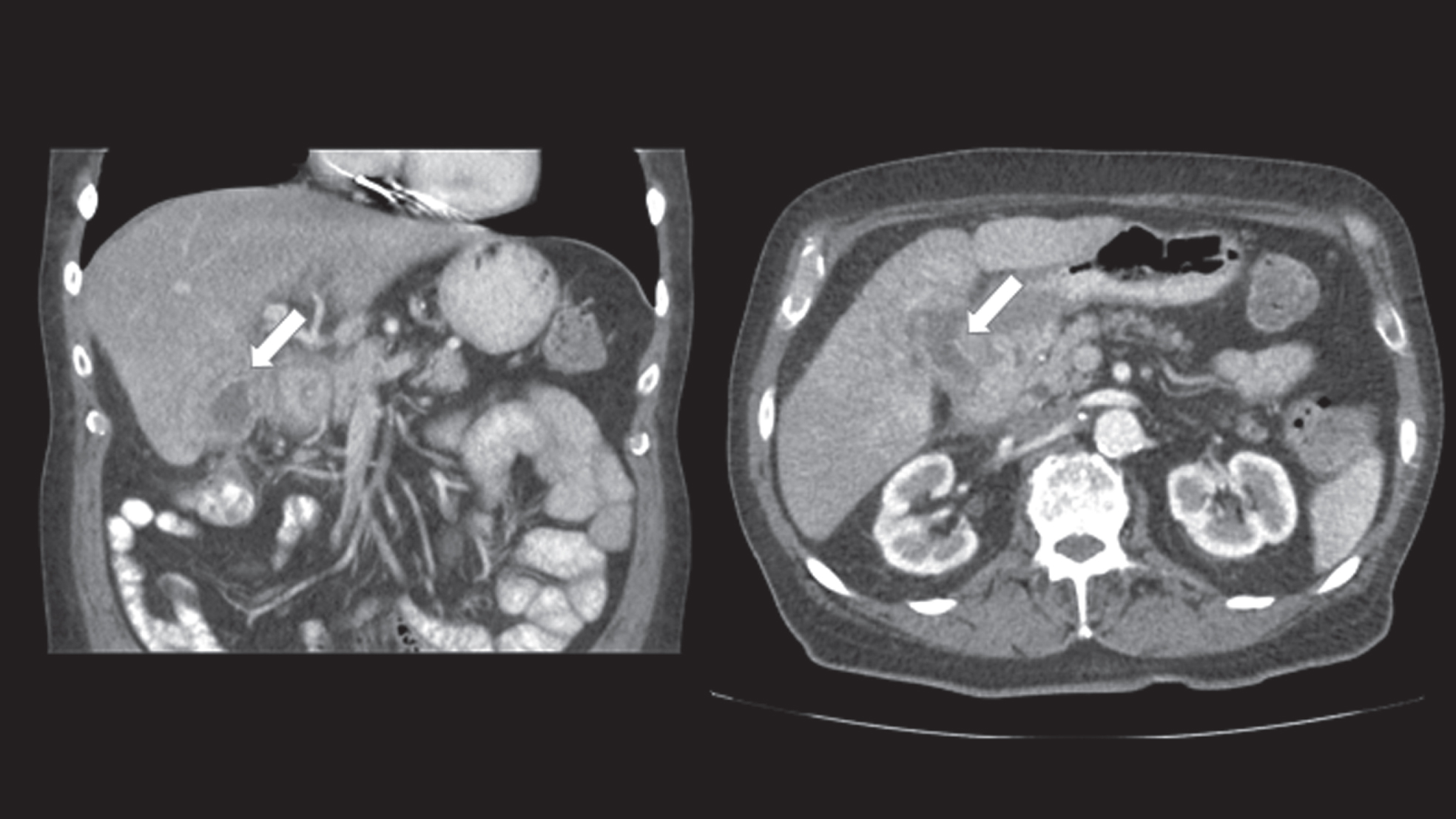
CT in portal venous phase with coronal (left) and axial (right) reformations: Inflammatory fluid collection around the gallbladder (white arrow).
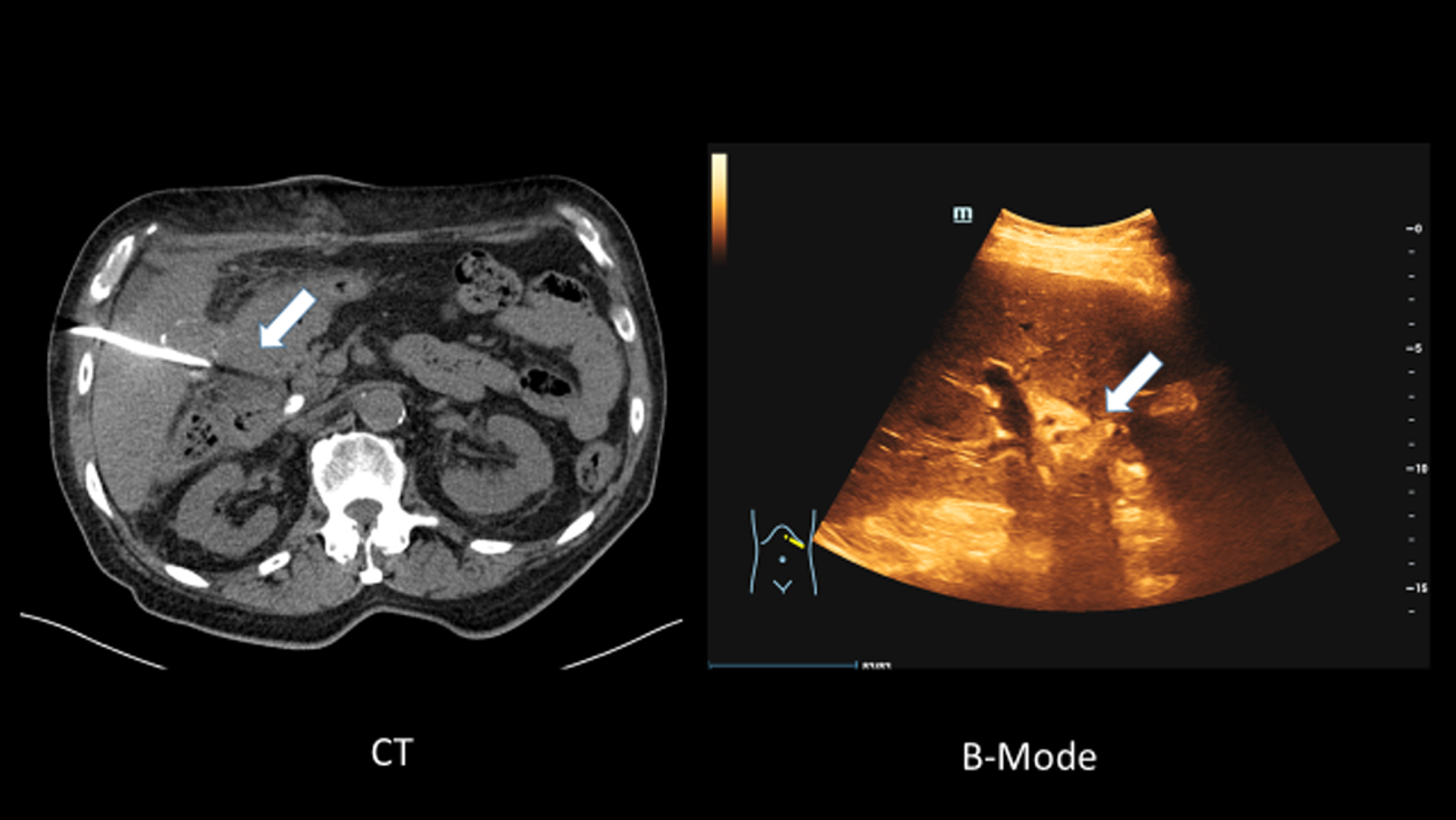
CT after placement of a 10 F drainage in the abscess, left axial CT without contrast media, right ultrasound with B-Mode. The fluid collection is hardly visible in native CT scan or B-Mode ultrasound.
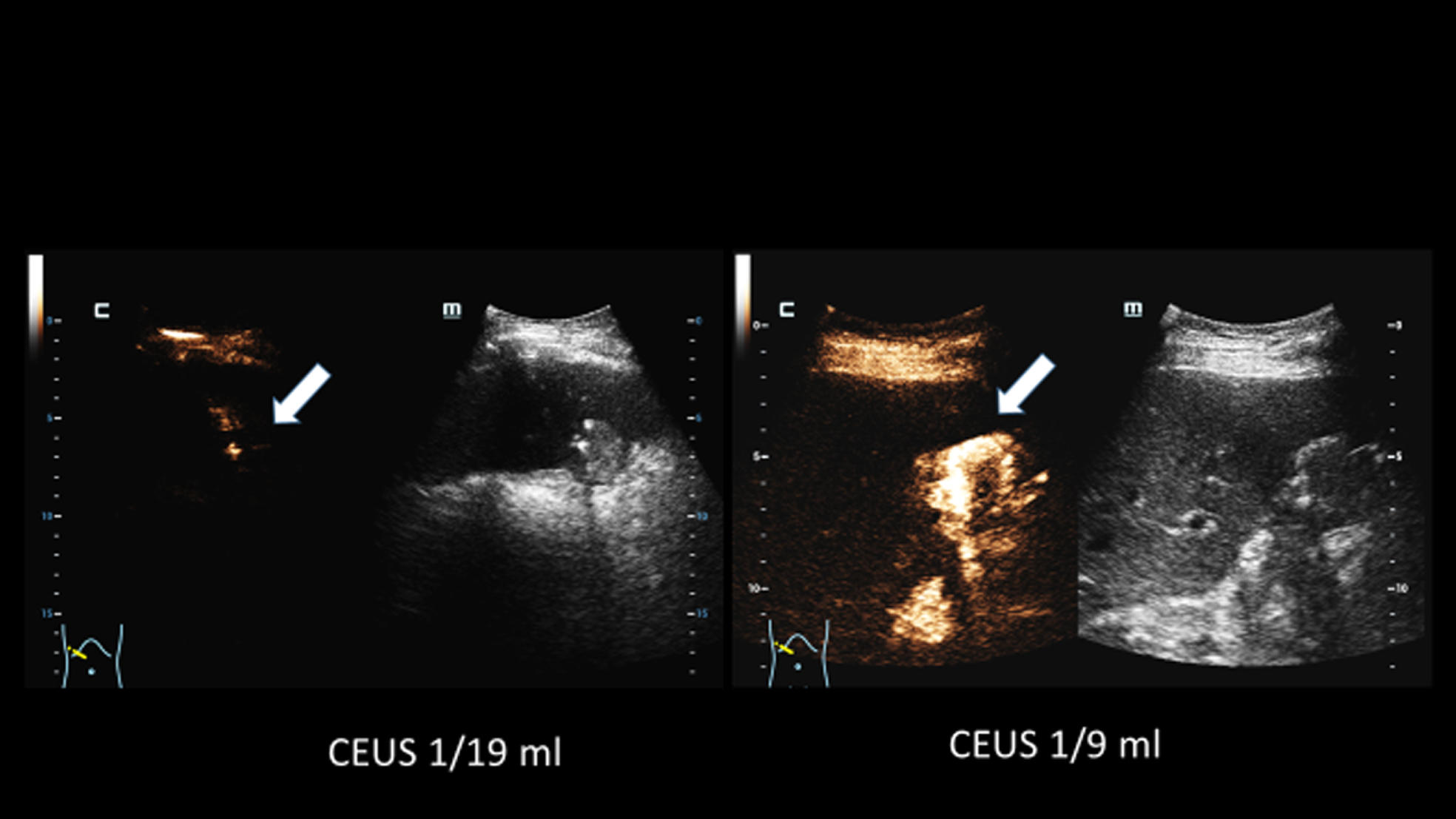
Application of contrast media via the drain for assessment of the drainage position and the abscess. Left 1 ml ultrasound contrast agent with 19 ml sodium chloride and right 1 ml ultrasound contrast agent with 9 ml sodium chloride was applied endoluminal by the drainage. With the high dilution (left) only the drainage loop is visible (arrow). With the higher dilution (right) the abscess can be displayed and more precisely.
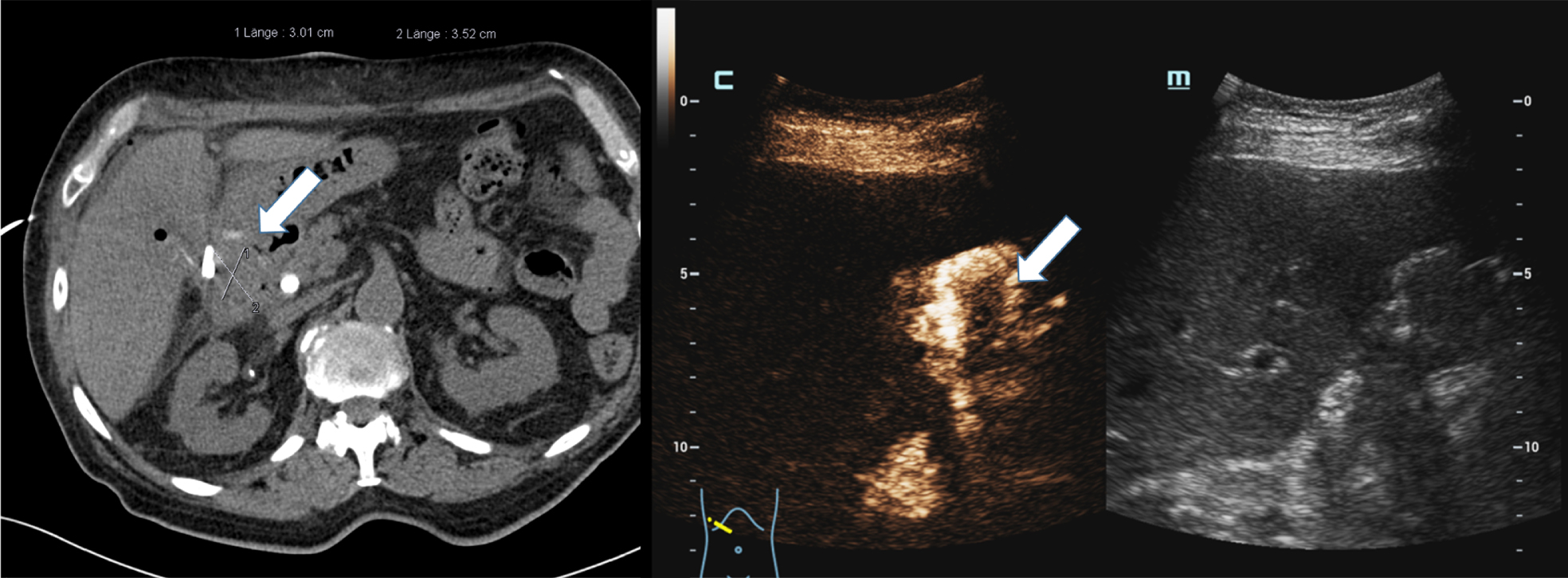
In comparison to the axial CT the abscess can easily be displayed with CEUS (left) and a sufficient dilution.
CEUS has been approved for many hepatic and non-hepatic applications. There is a growing number of CEUS indications and it is more and more integrated into clinical use [8, 16].
Percutaneous abscess drainages are also frequently placed either with fluoroscopy or ultrasound guidance depending on the localization of the fluid collection [17].
Currently there are no clear recommendations on whether or not drainages should be flushed with contrast media.
CEUS not only enables the detection and characterization of inflammatory fluid collections, but also functions as a control after the insertion of drainages [13, 18]. This also includes the display of drainage in the biliary tract using CT. B-Mode sonography only shows the inflammatory fluid formations, as air inclusions lead to artifacts. Only a small amount of sulfur hexafluoride microbubbles of 1 ml ultrasound contrast agent diluted with 9 ml sodium chloride sodium chloride can clearly show the course of the percutaneous drainage. The amount of ultrasound contrast media depends on many factors. If large drainages or bigger abscesses (e.g. 5–6 cm) are to be assessed 1 ml of contrast media might be sufficient [19, 20]. More contrast media might be needed for fistulas in a deep localization or in obese patients. However, if too much contrast media is used shadowing can be observed.
This also simplifies the decision on further procedure, whether the drainage can already be removed or not. In addition, other causes of inflammation such as fistulas to intestinal loops but also to biliary tracts must be recorded [21, 22]. This is possible with a low mechanical index (MI <0.2) and contrast harmonic imaging (CHI). In addition, the local resolution down to the capillary level is clearly superior to that in CT or MRI and does not carry the risk of impairment in kidney function, iodine allergy or radiation exposure. It is also possible to check seriously ill intensive care patients without being transported to the radiology department. CEUS is increasingly integrated into mobile devices. This means that dynamic control of inflammatory collection can be carried out much faster.
Microbubbles are strictly intravascular which is why they only have connection to the blood system in case of fistulas if injected into the drainage, but a connection to the biliary system / bile ducts can also be demonstrated with CEUS. Inflammatory collections and the extent of the drained abscess can be recorded with CEUS. In analogy, the percutaneous drainage can also be clearly evaluated with CEUS.
The advantage of CEUS is as a dynamic ultrasound examination technique that can be carried out quickly and documented in PACS. The present results of a post interventional control with contrast agent ultrasound show that these controls can be carried out without radiation exposure. The assessment of any remaining abscess is much more precise when using CEUS than in the B-Mode images. The fistulas can be recorded dynamically and the spread of inflammatory changes can be assessed dynamically. This also makes it easier to decide to what extent an abscess is sufficiently drained to remove the drainage. Ultrasound contrast medium enables a very high level of detail so that inflammatory wall structures and membranes can be assessed more precisely. Furthermore, fistulas can be displayed and the extent of the fistulas and conglomerates can be assessed for planning of surgeries. For endoluminal and endocavitary CEUS a smaller amount of contrast media is needed, since the volume of the fluid within a cavity is much smaller than the volume of circulating blood in the vascular system. The second-generation ultrasound contrast media is stable towards high frequencies and provides providing sufficient backscatter for endocavitary use and can even be used for up to 30 minutes. The mechanical index (MI) reduced to a sufficient value (less than 0.2). Contrast harmonic imaging (CHI) enables assessment of the microbubbles down to the capillary level. A combination with an intravenous ultrasound media application can then be used. In this case the abscess is depicted as a complicated cystic structure/area? with a marginal hyperemia. The ultrasound contrast agent does not reduce the kidney function or influence the thyroid gland. It is also radiation free with the best temporal and spatial resolution. However, special high-end ultrasound devices are necessary. Even though, there is not yet a recommendation for intracavitary use, the EFSUMB guidelines acknowledge the use of ultrasound contrast media in the assessment of non-physiological cavities safe and effective and a clinical individual decision can be made [23].
The main limitation is the relatively small number of patients collected in a short period of time and the retrospective design of the study.
Conclusion
In this study we could show the clear benefit of flushing drainages under CEUS during follow-up, since the fistulas to adjacent structures could clearly be demonstrated. Especially in patients who have undergone kidney transplantation, CEUS should be preferred to CT as the microbubbles do not decrease the kidney function.