
Abstract
BACKGROUND:
Vesicoureteral reflux (VUR) represents a common pediatric anomaly in children with an upper urinary tract infection (UTI) and is defined as a retrograde flow of urine from the bladder into the upper urinary tract. There are many diagnostic options available, including voiding cystourethrography (VCUG) and contrasted-enhanced urosonography (ceVUS). ceVUS combines a diagnostic tool with a high sensitivity and specificity which, according to previous study results, was even shown to be superior to VCUG. Nevertheless, despite the recommendation of the EFSUMB, the ceVUS has not found a widespread use in clinical diagnostics in Europe yet.
MATERIALS AND METHODS:
Between 2016 and 2020, 49 patients with a marked female dominance (n = 37) were included. The youngest patient had an age of 5 months, the oldest patient 60 years. The contrast agent used in ceVUS was SonoVue®, a second-generation blood-pool agent. All examinations were performed and interpreted by a single experienced radiologist (EFSUMB Level 3).
RESULTS:
The 49 patients included in the study showed no adverse effects. 51% of patients (n = 26) were referred with the initial diagnosis of suspected VUR, while 49% of patients (n = 23) came for follow-up examination or to rule out recurrence of VUR. The vast majority had at least one febrile urinary tract infection in their recent medical history (n = 45; 91,8%).
CONCLUSION:
ceVUS is an examination method with a low risk profile which represents with its high sensitivity and specificity an excellent diagnostic tool in the evaluation of vesicoureteral reflux, especially in consideration of a generally very young patient cohort.
Keywords
Introduction
Vesicoureteral reflux (VUR) is defined as a retrograde flow of urine from the bladder into the upper urinary tract and occurs as a typical urological pediatric anomaly in 1–2 % of the pediatric population [1–4]. With a prevalence of around 30–40%, VUR is diagnosed within the pediatric population with a documented urinary tract infection (UTI) [1, 5]. The pathogenesis of VUR in childhood still remains unclear, but it seems to be a congenital anomaly at the vesico-ureteral junction which is mainly caused by an abnormal embryological development [6].
The male-to-female ratio differs along the literature. Capozza et al. described a ratio of VUR with a prevalence of 3:1 in children under 6 months by an equal ratio at an age older than 21 months [7] whereas other studies have shown a percentage distribution of 91,9% female and 8,1% male patients [8]. Former studies also showed a strong genetic component with a prevalence of 27,4% in siblings and 35,7% in children with affected parents [9] while a specific causative gene has not been found yet [2, 10]. Recurrent VUR can lead to reappearing pyelonephritis, can induce the development of renal scarring and arterial hypertension or even end in end-stage renal disease [1, 2]. In addition to a thorough clinical examination followed by blood testing and blood pressure control, other imaging modalities represent an important part in den clinical setting of evaluating VUR. Available imaging modalities include among others voiding cystourethrography (VCUG), contrast-enhanced urosonography (ceVUS) or DSMA renal cortical scintigraphy [3]. Next to the high sensitivity and specificity, avoidance of ionizing radiation displays one of the elementary advantages of ceVUS [4]. Next to the VCUG, ceVUS also allows the evaluation of the entire urinary tract, which used to be a limited element in the earlier days [11, 12]. Further on, a recent study showed a sensitivity of 100% in detecting VUR when compared to VCUG [13] which goes along with the literature [14, 15].
VUR can be classified in five different subtypes. Grade I implies reflux in the non-dilated ureter while in Grade II the reflux also includes the renal pelvis and calyces. Grade III describes the situation when mild or moderate dilatation of the ureter and renal pelvis occurs and there is no or just a minimal blunting of the fornices. Grad IV is defined as a moderate dilatation and tortuosity of the ureter, renal pelvis and calyces while Grade V depicts a gross dilatation and tortuosity of the ureter, the renal pelvis, the calyces with accompanying loss of the papillary impressions [16] (Fig. 1).
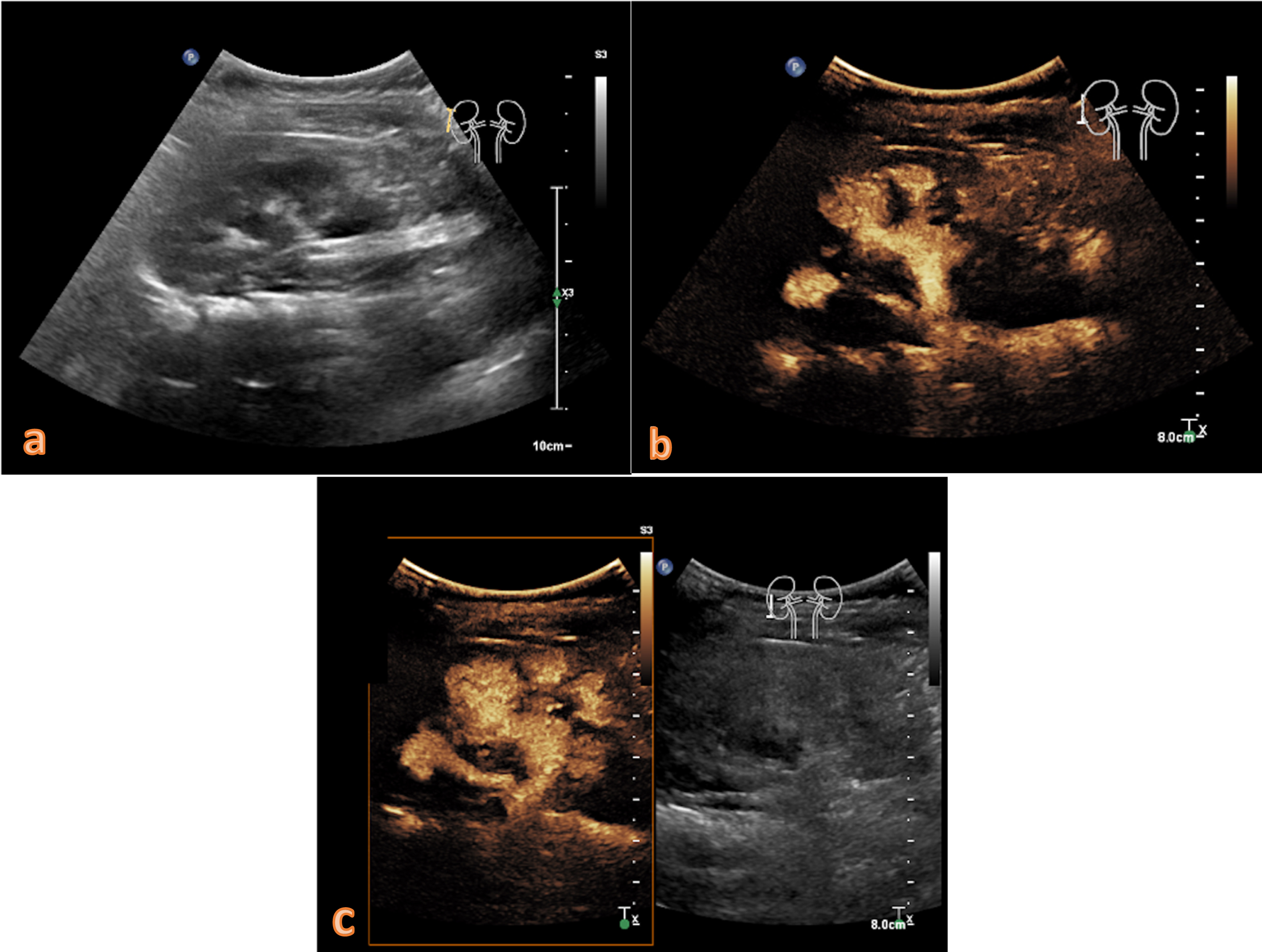
8-month year old girl with recurrent upper urinary tract infections showing a duplex kidney revealed by native B-mode (a). After administration of contrast agent, a marked enhancement of the right sided duplex kidney can be seen with a concomitant noticeable dilatation of the renal pelvis and initial blunting of the calyces in the upper (b) as well as in the lower part of the kidney (c). These sonomorphological findings indicate vesicoureteral reflux grade III.
SonoVue®, as a second-generation blood pool agent is the most widely used intravenous contrast agent in adults [17, 18]. In a retrospective study with almost 24.000 patients, no fatal events were registered by only having 29 adverse reactions (3 severe, 3 moderate and 23 mild) [19]. The intravesical use of SonoVue® in children has been approved by the U.S. Food and Drug administration (FDA) and the European Medicine Agency for the study of pediatric urinary tract to detect VUR [11, 20]. That goes along with large studies confirming the excellent safety profile of ceVUS at low doses of SonoVue® [14, 21] with minor transient effects only occurring in up to 3.7% of cases which usually are associated with the preceding bladder catheterization [21]. Even a safe use of SonoVue® during pregnancy has already been shown in first small case studies [22].
According to the EFSUMB guidelines, the use of ceVUS in the context of VUR is particularly recommended in the initial diagnostic of suspected VUR, in follow-up imaging after conservative or surgical therapy and in the screening of high-risk patients such as sibling or patients undergoing kidney transplantation [23]. According to the in-house paediatric urology setting, a different diagnostic strategy is still used from time to time in everyday clinical practice, depending on gender. In girls, ceVUS is often performed at an early stage, while in boys VCUG is sometimes still favored for better diagnosis of congenital urethral valves.
Furthermore, CEUS can also be performed during endoscopic treatments with the advantage of real-time monitoring which offers the possibility of repeated injections during the anti-reflux therapy. Thereby, CEUS increases the effectiveness of the therapeutic procedure and reduces the number of reinjections [24]. In addition to the indication presented here for the detection of VUR, CEUS can be widely used. This includes the intracavitary application of contrast agent into the pleural gap, the bile duct system or even in abscess formations, whereby these are usually considered off-label in pediatric patients [25]. Despite the advantages of ceVUS, the Guidelines of the European Association of Urology still set the VCUG as gold standard for the diagnosis and grading of VUR. Consequently, ceVUS is currently being performed in large patient collectives mainly in specialized centers outside of Central and Eastern Europe [26, 27].
The present retrospective single-center study was approved by our institutional ethical committee and all data were gained according to the principles expressed in the Declaration of Helsinki/Edinburgh 2002. Ethics Committee, Medical Faculty, Ludwig-Maximilians-University Munich; 17-087; date of approval: 14 March 2017.
In the present study a total of 49 patients were examined whereas the majority were female patients (n = 47, 95,9%). The period of investigation was between June 2016 and May 2020.
Before performing the CEUS scan, a detailed medical consultation about all potential risks took place and an oral and written informed consent were obtained by every patient. During the study there were no adverse side effects registered due to the applied contrast agent and a sufficient imaging quality could be achieved in every examination. The patient files were stored in the local archiving system of our institution to allow further analyses and a precise interpretation of the gained data.
All examinations were performed and subsequently analyzed by a single well-experienced radiologist (EFSUMB level 3) with a professional experience since 2000. The included patients were examined with high-end up-to-date ultrasound systems by using up to date CEUS protocols and in a supine position (Philips Ultrasound iU22, EPIQ 7, Seattle, Washington, USA; Samsung RS 80 A, Chertsey, Surrey, GB). SonoVue was used as contrast agent (Bracco, Milan, Italy), a second-generation blood-pool contrast agent with an only intravascular distribution pattern. That contrast agent also has been approved by the U.S. Food and Drug administration (FDA) and the European Medicine agency for the study of the pediatric urinary tract to detect VUR [11, 20]. A low mechanical index (< 0,2) helped to avoid an early destruction of the injected microbubbles. The bladder was contrasted using a 50 ml 0,9% sodium chloride syringe containing 0.3 ml of SonoVue. To achieve a good balance between a too low and too high amount of contrast agent, 1–3 injections of the diluted contrast agent are applied depending on the age of the patient and the size of the bladder. A too small amount of contrast agent can lead to a reduced delimitation of the cavity border, a too high amount of contrast agent can lead to a pooling of the microbubbles due to the diminished ability of a free movement or distribution [25].
Results
Between July 2016 and May 2020, a total number of 49 patients underwent CEUS examination. None of the 49 patients showed any kind of adverse reaction. The patient age ranged from 5 months to 60 years with a median age of 7,9 years and a mean age of 11,4. The patient population can further be subdivided into 47 female patients (95,9%) and only one male patient (4,1%) at an age of one year. Four patients had a duplex kidney with a bifid ureter, three of them with a pathological finding, one having an inconspicuous ultrasonographic result.
By forming two subgroups with patients younger and older than 18 years, the patients in the younger subgroup showed a median patient age of 6,5 years with a mean age of 5,8 years. The older subgroup showed a median patient age of 22,7 years with a mean age of 28,9 years. Within the patients with diagnosed bifid ureter the median age was 5,3 years with a mean age of 8,5 years (Table 1).
Overview of the patient collective in terms of number of patients and age distribution
Overview of the patient collective in terms of number of patients and age distribution
Within the 49 patients, 29 patients had inconspicuous and 20 patients had pathological findings. This corresponds to a percentage of 59,2% to 40,8% between normal and pathological findings. Further examination of the presented patient cohort with abnormal findings revealed a slight difference between right to left. In total, eleven patients had an exclusively positive finding on the left side, seven patients on the right side and two patients on both sides, resulting in a percentage value of 55%, 35% and 10% (n = 20). The left pyelo-ureteral unit (PUU) was conspicuous in 61,5% of the examinations (n = 16) while the right side showed a conspicuous finding in 38,5% of the cases (n = 10) (Table 2). In consideration of the four duplex kidneys, this leads to a total number of 26 abnormal PUU findings out of the included 102 PPUs (25,5%).
Overview of the number of affected patients with display of the affected side of the vesicoureteral reflux
The leading indication to perform ceVUS was in patients with at least one UTI in their present medical history. Among them, 45 patients had at least one UTI (91,8%), whereby three patients without a UTI were exclusively referred for a follow-up examination (6,1%) and one patient was referred to the Radiology Department due to the diagnosis of hydronephrosis (2,0%). In the included cohort, the number of patients without previous surgery is higher than that of patients with previous surgery (n = 36 respectively n = 13; 73,5% respectively 26,5%) (Table 3).
Number of patients according to the given indication
In the evaluation of the patients regarding the number of upper urinary tract infections, the clinical data of recurrent UTI were equated with the number greater than 4. Regarding to that, the vast majority experienced more than 4 UTIs (n = 27; 55,1%) [26]. The second peak is in the group with only one UTI followed by patients who had no history of UTIs (Table 4). The median age of patients with more than 4 UTIs (n = 19) is 10,5 years with a mean age of 14,3 years, the median age of patients who had a previous surgery is 15,9 years with a mean age of 18,2 years. The range of patients with more than 4 UTIs is between 5 and 50,8 years, that of patients with a previously performed surgery between 5,8 and 50,8 years.
Number of upper urinary tract infections in relation to the number of patients affected
Contrast-enhanced sonography is an established method in diagnosing VUR, but so far only plays a minor role in Europe. Already at the beginning of the 21st century studies showed the high efficacy of ceVUS, with the possibility to reduce a supplementary examination by VCUG by a percentage up to 53% [29, 30]. Since then, however, there has been no widespread use of ceVUS and the literature shows that the case studies with the exception of a study from Greece [21] show a comparable patient size with usually two-digit patient numbers [31]. The largest study in central Europe was conducted by a research team from Poland who compared 3D/4D ceVUS with 2D ceVUS. In 150 patients with a mean age of 3.7 years, they found a superiority of 3D/4D ceVUS over 2D ceVUS [32].
Native ultrasound imaging has found its place in the regular workflow of young patients in an early period after the onset of a UTI in both, the 2012 and 2015 published guidelines of the European Association of Urology and in the American Urological Association Guidelines, but the gold standard in the further diagnostics for suspect native ultrasound still remains the VCUG [26, 27]. In consideration of the recommendations of the 2017 updated EFSUMB guidelines, ceVUS however should be performed as part of the initial examination in suspected cases of VUR, in postoperative follow-up’s and in the screening of high-risk patients such as patients with a positive family history [9] or after a kidney transplantation [23].
Between July 2016 and May 2020, 49 patients could be included in this study with a female to male ratio of 95,9% to 4,1% (n = 47 respectively n = 2). This ratio is quite similar to the patient cohort described by Hoberman et al. (8) but differ from other studies that showed a distribution of approximately 3:1 [7, 13] which is presumably due to different inclusion criteria’s, the small number of enrolled patients and the fact, that not only the pediatric urologists of the in-house urological department still refer boys to the VCGU for a better assessment of the urethra, while the ceVUS is the method of choice within the female population. Overall, the very broad cohort with an age structure between 5 month and 60 years, no severe adverse effects were observed after intravesical application of contrast agent which goes in line with the recent literature [21]. In comparison with the VCUG and its iodine-containing contrast agent, ceVUS has a significantly better safety profile. In large case studies, side effects ranging from new-onset urticaria, iatrogenic hypertension to even anaphylaxis and laryngeal edema in up to 0.26 –0.48 percent of the cases [33].
Within the group of patients with no pre-existing but clinical suspicion of VUR (n = 25), this study showed confirmation of the suspected diagnosis in 52% of cases. There is no significant difference between the number of previous urinary tract infections and a higher probability of suffering from VUR. In the group of patients who have already undergone surgery (n = 13) four patients still show VUR (30,8%). According to the current literature, this represents a very large number of cases while having an operative success rate of up to 98% in patients undergoing open surgery [16]. Depending on the severity of the reflux, the success rate of an endoscopic therapy is between 66% and 79%, while the success rate increases up to 90% after a second endoscopic session [34]. Possible reasons for such a high number of post-surgical patients in the underlying cohort might be the selection bias of a University Hospital with a specialized Urology and Radiology Department and the increasing number of endoscopic treatments in the past years and the small patient cohort.
When diagnostic imaging techniques are used, VCUG in comparison to ceVUS still remains the gold standard in the diagnostic workflow of VUR [5, 26]. The use of ionizing radiation and contrast agents with higher risk profiles compared to SonoVue® are relevant disadvantages compared to ceVUS. Some former studies showed, that the sensitivity, specificity and the negative predictive value of VCUG and ceVUS are equivalent with a range up to 97% [14, 35]. The radiation exposure of the VCUG means an exposure for the examined patient, equally and not to be neglected, it also means a radiation exposure for parents, who usually attend the examination to provide a calm atmosphere for the infant. Another advantage is the possibility to perform the examination even at the patient’s bedside, which can lead to a substantial relief for the attending doctor and a stress-free examination for the child.
Notwithstanding these advantages, there are also a few studies, that previously demonstrated the diagnostic superiority of ceVUS compared to VCGU in detecting and grading VUR, implying that ceVUS should at least considered as an equivalent imaging modality [12, 36].
Conclusion
CeVUS displays a highly sensitive and ionization-free imaging modality with an excellent safety profile concerning the application of intravesical contrast agent. Further advantages in the examination of small children are on the one hand the absence of radiation exposure not only for the patient but also for the parents who attend the examination to allow a calm atmosphere and on the other hand the fact that the examination can be carried out directly at the patient’s bedside. Due to its high sensitivity and specificity, also in correlation with VCUG, ceVUS should always be considered as a potential imaging modality for the diagnostic confirmation of VUR.