
Abstract
BACKGROUND:
Computed tomographic (CT) imaging in suspected pulmonary artery embolism represents the standard procedure. Studies without iterative reconstruction proved beneficial using increased iodine delivery rate (IDR). This study compares image quality in pulmonary arteries on iteratively reconstructed CT images of patients with suspected pulmonary embolism using different IDR.
MATERIAL AND METHODS:
1065 patients were included in the study. Patients in group A (n = 493) received an iodine concentration of 40 g/100 ml (IDR 1.6 g/s) and patients in group B (n = 572) an iodine concentration of 35 g/100 ml (IDR 1.4 g/s) at a flow rate of 4 ml/s. A 80-detector spiral CT scanner with iterative reconstruction was used. We measured mean density values in truncus pulmonalis, both pulmonary arteries and segmental pulmonary arteries. Subjectively, the contrast of apical and basal pulmonary arteries was determined on a 4-point Likert scale.
RESULTS:
Radiodensity was significantly higher in all measured pulmonary arteries using the increased IDR (p < 0.001). TP: 483.0 HU vs. 393.4 HU; APD: 452.1 HU vs. 372.1 HU; APS: 448.2 HU vs. 374.4 HU; ASP: 443.9 vs. 374.4 HU. Subjectively assessed contrast enhancement in apical (p = 0.077) and basal (p = 0.429) lung sections showed no significant differences.
CONCLUSION:
Higher IDR improves objective image quality in all patients with significantly higher radiodensities by iterative reconstruction. Subjective contrast of apical and basal lung sections did not differ. The number of non-sufficient scans decreased with high IDR.
Introduction
Pulmonary embolism (PE), an obstruction of the pulmonary arteries due to the washout of an embolus from the venous circulation, is a potentially life-threatening event. The gold standard method for diagnosing PE is computed tomographic pulmonary angiography (CTPA) [1–5], although recent advances have shown that ultrasound may serve as an possible alternative [6]. Using iodine-based contrast agent (CM), emboli can be visualized indirectly as filling defects in the pulmonary arteries thus allowing the diagnosis of PE [1, 7] (Fig. 1). To minimize the rate of false-positive and false-negative results, studies reported a cut-off value of 250 Hounsfield units (HU) for a diagnostically conclusive CTPA examination [8–10]. Less contrast-attenuated lung arteries may not allow the diagnosis of PE (Fig. 2).
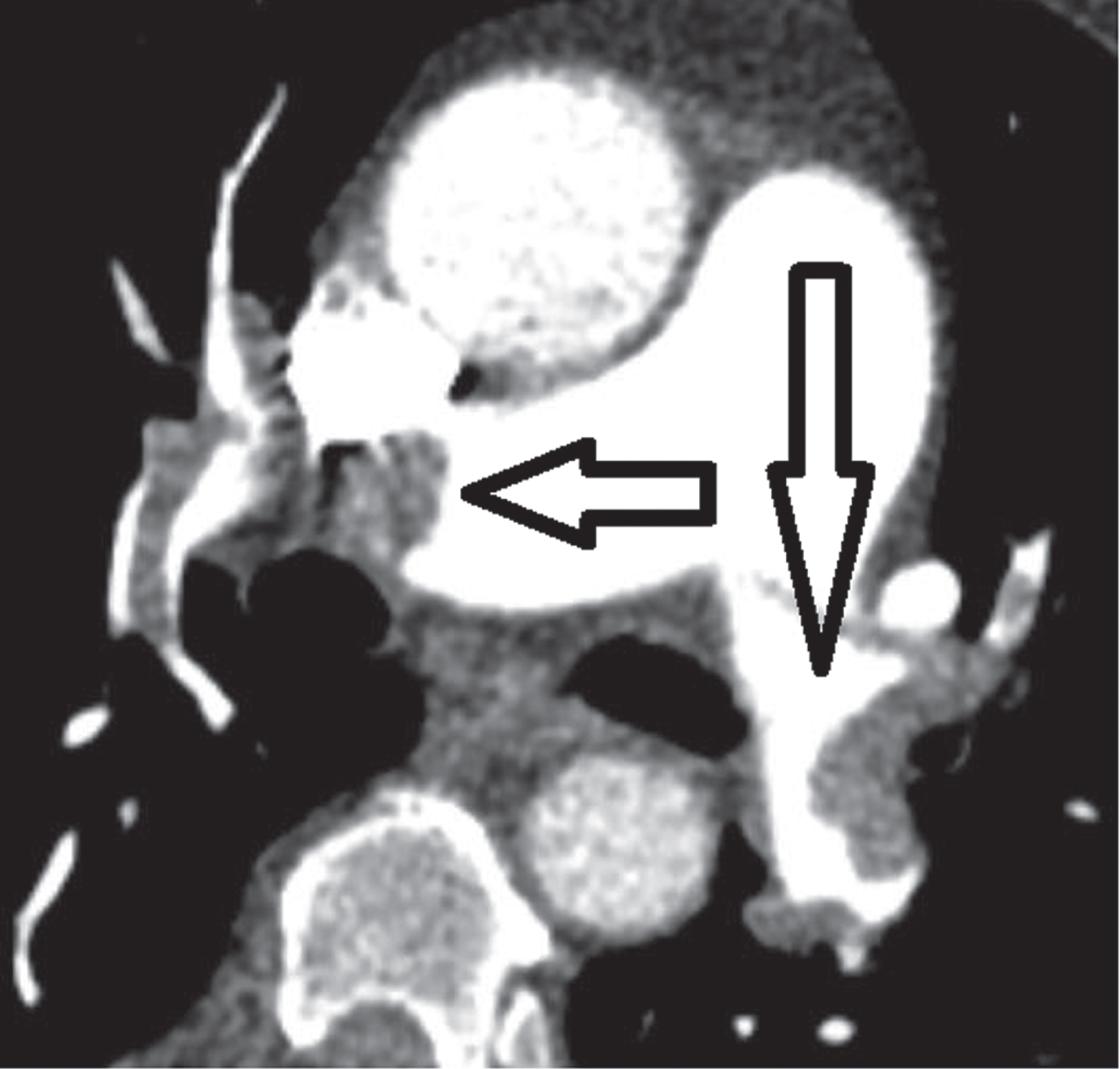
Axial CT image of hemodynamically relevant PE in A. pulmonalis dextra and A. pulmonalis sinistra in an axial CTPA image. PE marked by black arrows.
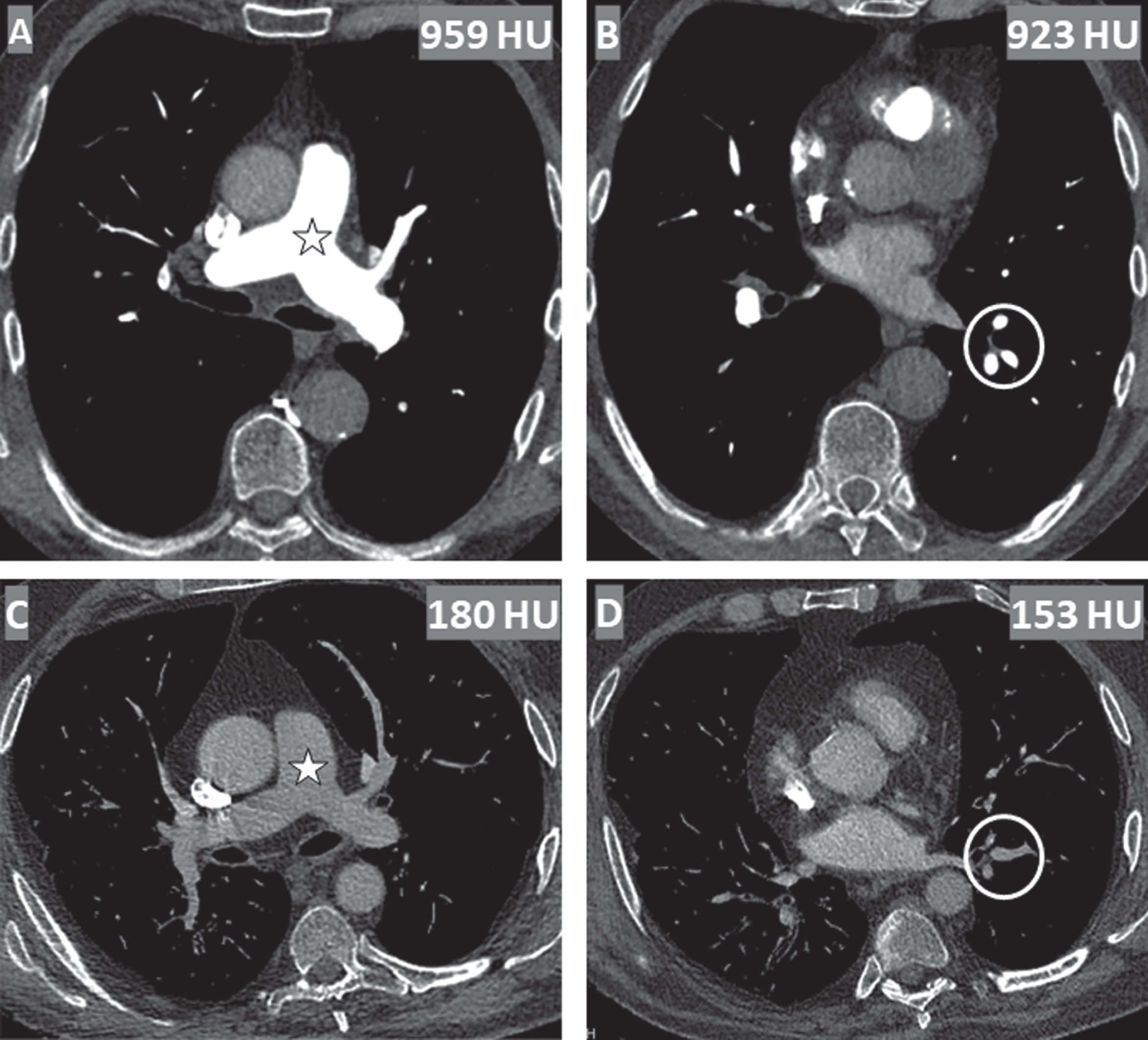
Axial CTPA images of the pulmonary trunk (marked by star) (A and C) and the lower lobe arteries (B and D) after the injection of 50 ml contrast. The measured mean density values are 959 vs. 180 HU for the pulmonary trunk and 923 HU vs. 156 HU in the segmental arteries of the left lower lobe. The improper image contrast (C and D) result in reduced sensitivity for PE diagnosis.
Various contrast agents with different iodine concentrations and effects are commercially available [4, 11–15]. Previous studies have found that increased injection rate and thus increased iodine delivery rate (IDR) leads to higher mean density values in the pulmonary arteries [3, 16]. The IDR is determined by the contrast agent’s iodine concentration and the injection rate. The injection rate is limited by the patient’s cubital vein catheter and the injector [4, 15–17]. In parallel, various methods such as the use of alternative breathing maneuvers, administration of the CM via the inferior vena cava inflow area, and different contrast injection protocols have already been investigated to optimize mean density values in the pulmonary arteries at the time of image acquisition [3, 18–20]. In recent years a new reconstruction method called “iterative reconstruction” (IR) has been introduced, which can improve computed tomography-based diagnosis [16, 22]. Iterative reconstruction can be used to improve image quality and reduce radiation dose [21–24]. The use of iterative reconstruction is reported to allow dose savings of up to 40%compared to filtered back projection (FBP) without the loss of adequate image quality [22, 24–26].
Based on these recent developments, the aim of this study was to evaluate the subjective and objective effect of higher IDR achieved by high concentrated contrast agent in PE diagnostics using IR.
Patients
For sufficient statistical power in this study, a sample size of at least 800 patients has been statistically calculated. In this study we analyzed the computed tomographic image recordings of 1065 patients who visited our clinic for exclusion of pulmonary artery embolism. The study was performed in accordance with the Declaration of Helsinki of the World Medical Association. The local ethics committee approved the study (EA4/140/17). Patients with noted technically incorrect bolus triggering, anatomic abnormalities, venous catheter access in the lower extremity, tracheostomized or intubated patients, non-adult patients and patients with contrast extravasation were excluded.
Scan parameters and contrast injection protocol
All examinations were performed on a monoenergetic 80-detector spiral CT scanner (Canon Aquilion Prime, Canon Medical Systems, Otawara, Japan). The following scan parameters were used: Tube voltage 100 kVp, tube current 80–600 mA, collimation 80×0.5 mm, pitch factor 1.388, rotation time 0.5 s. The tube current was actively modulated depending on patient’s size. Images were reconstructed using iterative reconstruction (AIDR 3D, Canon Medical Systems, Otawara, Japan) with medium IR strength applied. Image data were transferred to the hospital’s internal Picture Archiving and Communication System (PACS) for analysis. The analysis of objective and subjective image quality was performed on a PACS workstation (Merlin Diagnostic Workcenter Version 5.8.1, Phönix-PACS GmbH, Freiburg, Germany).
Between the two groups, the iodine concentration and thus the iodine delivery rate (expressed in grams of iodine per second) was changed. The total amount of CM was weight-adjusted in both groups. Patients in group A received a weight-adjusted contrast bolus of Iomeprol 400 (Imeron 400, Bracco Imaging Deutschland GmbH, Konstanz, Germany) (iodine concentration 400 mg/ml) with an IDR of 1.6 g/s. Patients in group B received a weight-adjusted contrast bolus of Iobitridol 350 (Xenetix, Guerbet GmbH, Sulzbach im Ts., Germany) (iodine concentration 350 mg/ml) with an IDR of 1.4 g/s.
In both groups, the prewarmed contrast agent was administered with an automatic injection device at a flow rate of 4 ml/s via a cubital vein. The contrast injection was followed by a 40 ml saline flush at an identical flow rate.
The CT scan was initiated by bolus tracking. For this purpose, a region of interest (ROI) was placed in the pulmonary trunk (TP). As soon as a threshold of 80 HU was exceeded all patients received the end-inspiratory breathing command “Please inhale and hold your breath.” To ensure linguistic understanding, the breathing command could be announced in different languages. After a fixed scan delay time of six seconds the device started the CT scan.
Objective image quality
For quantitative analysis of CTPA images, ROIs were manually placed in the vessel lumen of the pulmonary trunk (ROI size: 100–125 mm2) (TP), Arteria pulmonalis dextra (ROI size: 75–100 mm2) (APD), Arteria pulmonalis sinistra (ROI size: 75–100 mm2) (APS) and the ascending aorta (ROI size: 100–125 mm2) (AA). To determine the contrast enhancement of peripherally located arteries, a 10–15 mm2 ROI was placed in segmental arteries (ASP) 8, 9 or 10 of the lower left lobe. Intravascular density values were noted.
Subjective image quality
In addition, by consensus two readers reviewed the CTPA images on a window with the following control variables: Window Center = 150, Window Width = 650. They subjectively graded the contrast of the apical and basal pulmonary arteries on the following 4-point scale: 0 = “Poor”, 1 = “Adequate”, 2 = “Good”, 3 = “Excellent”.
To establish an interrater agreement for the parameters “Contrast enhancement apical” and “Contrast enhancement basal”, 100 randomly selected patients were submitted to a board-certified radiologist with eleven years of radiologic experience. She also evaluated the parameters on the 4-point scale. The Kendall’s tau B was then calculated. The effect size of Kendall’s tau was graded according to Cohen (1988): 0.1–0.3 = small; 0.3–0.5 = moderate; > 0.5 = large [27].
Additionally, the number of examinations without required density (< 250 HU) were noted and compared.
Statistical analysis
Statistical analysis was performed using the IBM Statistics 25 for Windows program (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as mean±standard deviation. Subjective image quality was analyzed by chi-square test. For analysis of nonnormally distributed density values and age, the Mann-Whitney U test was used. For analysis of gender, the chi-square test was applied. Statistical significance was present at a p-value < 0.05.
Results
Patient characteristics
A total of 1310 eligible patients were identified. Due to lack of notation of the contrast agent in the examination protocols (nA = 124, nB = 62) or due to the use of alternative contrast agents (nA = 39, nB = 20), statistical analysis was performed with 1065 patients in total. The patient characteristics are shown in Table 1. There was no significant difference in occurrence of PE between the two groups (p = 0.151). PE was diagnosed in 21.7%(107/493) of group A patients and 19.0%(104/572) of group B patients.
Patient’s characteristics
Patient’s characteristics
The mean density value in the pulmonary trunk was 483.0±166.4 HU in group A and 393.4±132.5 HU in group B (p < 0.001). In all other more peripherally located pulmonary arteries (APS, APD, segmental arteries) as well as the ascending aorta, the use of a high concentrated contrast agent also resulted in significantly increased contrast enhancement (Fig. 3). The p-value was p < 0.001 for AA, APD, APS, ASP, respectively. 6.3%(31/493) of the images in group A and 14.0%(80/572) of the images in group B had mean density values < 250 HU in the pulmonary trunk (p < 0.001).
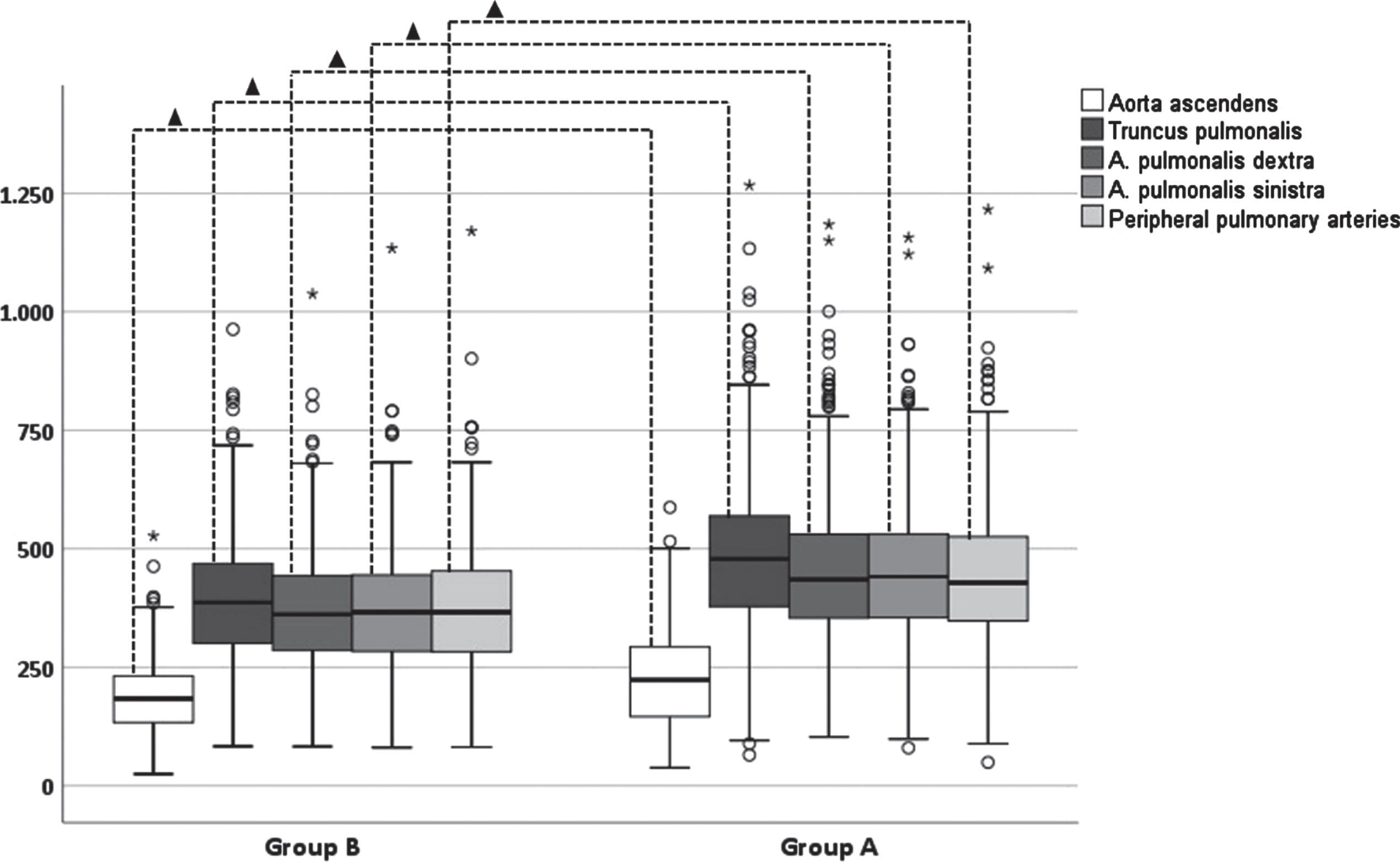
Contrast enhancement in the lung arteries and the aorta for both groups. Circle indicates a mild outlier. Star indicates an extreme outlier. Triangle indicates statistical significance (p < 0.05) between the two groups.
Optimal contrast enhancement in the apical pulmonary arteries was seen in 64.1%(316/493) of patients in group A and 57.2%(327/572) of patients in group B (Table 2). Poor contrast enhancement of apical arteries was seen in 3.3%(16/493) of group A patients and 3.3%(19/572) of group B patients. Excellent contrast of basal pulmonary arteries was seen in 55.0%(271/493) of group A patients and 52.8%(302/572) of group B patients. 2.6%(13/493) of group A patients and 2.6%/15/572) of group B patients had a poor contrast enhancement in the basal pulmonary arteries. There were no statistically significant differences between the two groups concerning the subjective contrast enhancement of apically and basally located pulmonary arteries (papical = 0.077; pbasal = 0.429).
Subjective image quality of apically and basically located peripheral pulmonary arteries
Subjective image quality of apically and basically located peripheral pulmonary arteries
For apical and basal contrast enhancement Kendall’s tau showed strong interrater agreements of τapical = 0.699 and τbasal = 0.589.
Discussion
In this study, we found that an IDR increased through the use of a high concentrated contrast agent in CTPA examinations with iterative image reconstruction resulted in a better contrast enhancement of central and peripheral pulmonary arteries. Increasing the iodine dose by 12.5%from 35 g per 100 ml to 40 g per 100 ml resulted in 22.8%greater contrast. This was evident not only in the large, central pulmonary arteries (TP, APD, APS) but also in the small, more peripherally located segmental arteries and in the ascending aorta. Despite the use of IR, an increased IDR significantly decreased the proportion of diagnostically inconclusive images with contrast < 250 HU. In group A 6.3%of the images were diagnostically inconclusive while in group B it 14.0%of the images were diagnostically inconclusive.
The influence of IDR was already demonstrated by Mühlenbruch et al, Keil et al, and Behrendt et al. [11, 28] without IR. They found that increasing the iodine concentration of the CM without increasing the IDR did not lead to any change in the contrast enhancement of the pulmonary arteries. Accordingly, the goal of high contrast in pulmonary arteries must be achieved by optimal IDR. Increasing IDR is possible in two ways: One way is to increase the contrast injection rate. This could increase the risk of CM extravasation and requires a minimum cubital vein catheter size, which is not always feasible in clinical practice. A second possibility is to increase the iodine concentration of the used CM.
Several studies have already investigated the effect of higher IDR on on the contrast in pulmonary arteries. They found that higher IDR resulted in significantly greater contrast of TP, APD, and APS [3, 29]. Commonly cited limitations of these studies are the small case numbers (80–120 consecutive patients). The authors recommended a larger study population to determine the true clinical benefit. Our study confirms the described results with a significantly higher case number. The use of IR instead of FPB in our study did not affect these results.
Most PE are localized at the lobar (upper, middle, and lower lobe arteries) and segmental (segmental arteries and their branches) levels [30]. We also examined the contrast enhancement of the segmental arteries. The reason is that smaller emboli with transient or no symptoms are reported to be overlooked, although they might have a high risk of recurrence and can be seen as a warning sign of larger emboli [2, 31]. Detection of smaller, peripherally located emboli could protect patients from future, life-threatening PE by initiating appropriate treatment early. We demonstrated that IR-based reconstruction had no effect on higher IDR which resulted in significantly higher mean density values of the peripherally located segmental arteries.
To our knowledge the study performed by Kosmala et al. in 2020 is the first study on this topic in which iterative image reconstruction was used [16]. In contrast to our study, CT-scanning was performed with a dual-energy CT scanner. In their retrospective analysis with 198 patients, they demonstrated that high IDR resulted in the strongest contrast enhancement in the pulmonary arteries. In their discussion, the authors pointed out that all patients with diagnosed PEs as well as not further specified artifacts were excluded from the statistical analysis. This meant that 198 of the 340 CTPA examinations performed were analyzed. Transfereability of the study to clinical practise might not be given. We examined 1065 patients on a monoenergetic CT scanner (widely used) and included all patients with PE. Because CTPA is performed primarily to diagnose PE, we consider the inclusion of this patient group as essential to demonstrate the true clinical benefit.
Despite the large number of cases, there was no statistically significant difference between the two groups for the subjectively assessed contrast enhancement of the apical and basal pulmonary arteries. However, we demonstrated by objective measurements that an increase of the IDR resulted in a significantly higher contrast of the peripheral pulmonary arterial pathway.
There are limitations of this study. Because of the retrospective nature of this study, the use of identical peripheral vein catheters cannot be guaranteed. Nevertheless, both our hospital’s standard protocols include a fixed contrast inflow rate of 4 ml/s. The automated injectors adjust the injection pressure to the targeted injection flow rate so that an achievement of 4 ml/s can be assumed. If this could not be guaranteed (technically incorrect bolus tracking), patients were excluded from this study.
In this study, we did not record any possible cardiovascular (arterial hypertension, valvular heart disease, persistent foramen ovale) or pulmonary diseases (pulmonary hypertension) of the patients, which could have had an influence on the cardiac output and thus on the distribution of the contrast agent in the entire pulmonary arterial pathway.
In addition, it was not possible to determine retrospectively whether patients understood the breathing command “Please inhale and hold your breath” and if they were able to sustain it for the full length of the examination. We suspect that some patients in both groups were unable to execute the breathing command correctly because of pain or dyspnea. This may have resulted in nondiagnostic images with mean density values < 250 HU. Due to the comparable patient population this effect should have occurred in both groups; an influence on the results seems therefore unlikely.
Conclusion
The use of high-concentration contrast agent at the same injection rate of CM resulted in significantly higher contrast enhancement in all centrally and peripherally located pulmonary arteries in iteratively reconstructed CTPA examination images. In both cohorts, mean density values above 300 HU were achieved. Nevertheless, the number of diagnostically inconclusive images was significantly reduced with increased iodine concentration.
Footnotes
Acknowledgment
This study was conducted as a part of the doctoral thesis of T. Burdenski.
LCA is grateful for her participation in the BIH Charité–Junior Clinician and Clinician Scientist Program and KKB is grateful for his participation in the BIH Charité Digital Clinician Scientist Program all funded by the Charité–Universitätsmedizin Berlin and the Berlin Institute of Health