
Abstract
BACKGROUND:
Ultrasound follow-up of transjugular intrahepatic portosystemic shunt (TIPS) is challenging due to the bent course of the stent-graft.
OBJECTIVE:
Aim of this retrospective study was to assess to which extent the combination of HR flow with Glazing Flow improves hemodynamic assessment in the ultrasound follow-up of TIPS.
METHODS:
Comparative studies with CCDS and High Resolution (HR)-Flow with Glazing Flow were evaluated regarding image quality and artifacts on a 5-point scale (0 = cannot be assessed up to 5 = maximum image quality without artifacts). In all cases, an experienced examiner performed the examinations with a 1–6 MHz probe (Resona 7, Mindray).
RESULTS:
61 ultrasound examinations in 48 patients were performed; the mean patient age was 54±14.2 years. The use of HR-Flow with Glazing Flow resulted in an improved flow display in 55/61 cases (90.2%). Both methods correlated well (r = 0.71), but HR flow with Glazing flow values were in general higher than CCDS values. The reading resulted in an average value of 2.52±0.54 for CCDS and 3.52±0.57 for HR flow with Glazing flow (p = 0.013).
CONCLUSION:
The combination of HR-Flow and Glazing Flow results in improved flow representation and reduction of artifacts in the ultrasound follow-up of TIPS.
Keywords
Introduction
Ultrasound diagnostics is the fastest available imaging to answer relevant questions regarding the planning, placement and follow-up of a transjugular intrahepatic portosystemic shunt (TIPS) in the hands of experienced examiners. Color-coded duplex sonography (CCDS) is the most important tool in the follow-up of TIPS. With high-performance ultrasound devices, CCDS is often available as a simultaneous mode with B-mode, Doppler spectral analysis and color Doppler. This facilitates identification of the hepatic artery, the portal vein and the hepatic veins and the acquisition of the flow curves.
After placement of TIPS, often from the right hepatic vein to the right portal vein, vascular flow changes to partially turbulent flow due to the shunt between the low-flow venous area and the medium flow of the portal vein with a high flow area within the stent-graft. Therefore, flow velocities of 10 cm/s up to 200 cm/s, with a normal flow velocity of 90 cm/s to 190 cm/s within the stent-graft [1], must be measured precisely and without relevant artifacts. This requires a broad experience with CCDS, since it is a very angle-dependent flow representation that requires optimal adjustment of flow rate to avoid artifacts such as aliasing or artifacts due to vibrations and pulsations. Blood flow measurements should only be carried out at an Doppler angle of 45 to 60 degrees [2]. Whereas at a Doppler angle of 90 degrees, no flow can be derived with the CCDS.
Advanced cirrhosis with portal hypertension and refractory ascites is one of the possible indications for the interventional placement of a TIPS [3, 4]. A less frequent indication is Budd-Chiari syndrome [5] with changes of the hepatic veins ranging from stenosis to occlusion, which are difficult to detect in ultrasound. Another emerging indication for TIPS is portal vein thrombosis [6]. These are difficult ultrasound conditions for CCDS. The assessment of TIPS after recanalization of a thrombosis of the stent-graft and/or the portal vein is another difficult ultrasound situation, even for experienced examiners. The day after placement of a TIPS, ultrasound assessment can be very difficult due to a thin layer of air trapped between the e-PTFE layers of the stent-graft [7]. However, it must be possible to rule out thrombosis or stenosis due to kinking of the stent-graft.
In a recent meta-analysis, Manatsahit et al found a sensitivity of 0.82 and a specificity of 0.58 for the assessment of TIPS dysfunction with ultrasound in the era of covered stents [8]. In the assessment of dysfunction of bare metal stents used as TIPS, sensitivities ranged from 64% to 84%, and specificities ranged from 70% to 100% [9]. Wit et al. found abnormalities in the follow-up after TIPS placement using Doppler ultrasound in 3.6% of patients. 7.8% of patients had TIPS revision due to clinical symptoms with inconclusive ultrasound studies [10]. Recently, newer high-resolution ultrasound techniques have been developed which try to achieve advantages for CCDS in difficult ultrasound conditions by digital flow detection and temporal and spatial summation with additional simultaneous acquisition of different ultrasound angles. This also includes the combination of HR-Flow with Glazing Flow. HR-Flow improves spatial resolution in color Doppler by continuous sampling of flow velocities in combination with zone sonography technology (ZST). ZST can cover the field of view in much fewer transit / receive cycles compared to conventional systems [11]. In Glazing Flow, 2D color information are visualized in 3D. This improves the differentiation of crossing vessels and vessels that are close to each other [12]. In a previous study we could demonstrate, that this combination can have advantages in determining the blood flow rate in the cirrhotic liver [12]. We hypothesized that HR-Flow/Glazing Flow could also improve US assessment in the follow up of TIPS.
The aim of this pilot study was to examine whether the combination of HR-Flow with Glazing Flow offers advantages in the imaging of blood flow and hemodynamic assessment of a TIPS.
Materials and methods
This study was approved by the institutional ethics committee (Reference number 21-2721-104). Written informed consent was waived due to the retrospective nature of this study.
Study design
Sixty-one consecutive ultrasound examinations of patients with TIPS between January 2021 and September 2021 were retrospectively analyzed. The ultrasound examinations were carried out for clinical reasons, either as routine US follow-up or due to presumed TIPS dysfunction, 660±1092 days after TIPS placement on an average (range 1–5987 days). All examinations were carried out on a modern high-end ultrasound device (Resona 7, Mindray, Shenzhen, P.R. China) by an experienced examiner with more than 3000 ultrasound examinations per year for more than 20 years with a high-resolution multifrequency probe (C1-6 MHz) and stored digitally. The assessment regarding possible artifacts was carried out retrospectively using the images stored in the Picture archiving and communication system (PACS) (syngo Imaging, Siemens Healthineers, Erlangen, Germany) by 2 independent readers, blinded to clinical and patient data, in consensus.
To assess the imaging quality of the TIPS tract, a scale from 0 to 5 was used. 0 meant no flow assessment possible; 1 flow assessment possible with massive artifacts; 2 with obvious artifacts; 3 partially overlaid with artifacts; 4 almost complete imaging of the TIPS tract without artifacts, 5 imaging of the entire TIPS tract with portal vein and hepatic vein confluence in one image without artifacts.
Image acquisition
The standard protocol included a B-mode examination of the entire abdomen, with special attention to signs of cirrhosis, portal hypertension and ascites, but also to possible complications after TIPS placement such as stenosis, kinking, dislocation and signs of acute thrombosis, bleeding and reactive inflammatory changes. The TIPS diameter was measured at three points in B-mode, proximally in the portal vein, centrally in the stent-graft and distally in the hepatic vein. With the help of CCDS, we assessed flow velocities in the portal vein, in the proximal and distal area of the stent-graft, in the liver veins and in the inferior vena cava (IVC). Additionally, flow velocity and resistive index of the hepatic artery was documented. All values were measured directly using the Doppler curve analysis program, with an optimal Doppler angle correction of 30 to 60 degrees. In addition, the complete TIPS tract, if possible, was documented in the PACS with CCDS and HR-Flow with Glazing-Flow (level 2 to 3) for independent assessment. The aim was to achieve an image that was as artifact-free as possible using adaptation to vascular flow via scale / PRF (pulse repetition frequency), color gain and sound angle.
The technical basis of HR Flow and Glazing Flow has been described earlier [12]. Briefly, in HR Flow, flow velocities are sampled continuously. In combination with zone sonography technology, HR Flow improves the spatial resolution in color Doppler. Glazing Flow is a 3D visualization method which can be used in color Doppler, power Doppler and HR Flow modes. This technique adds height information to the color Doppler display and allows a better differentiation of vessels which are close to each other.
Statistics
For all samples arithmetic means with standard deviation is given. Spearman correlation coefficients were calculated for correlation of CCDS rating and HR-Flow/Glazing-Flow rating. In addition, the ranks of both methods were compared using a two-sided paired t-Test. A P value <0.05 was considered significant in all tests. All statistical analyses were performed using MedCalc software (MedCalc Software Ltd, Ostend, Belgium).
Results
61 ultrasound examinations of 48 patients (23 women, 25 men) were performed. The patient age was 20–83 years, with an average of 54±14.2 years. Indications for TIPS placement were: therapy-refractory ascites (21 patients), varices (17 patients), acute portal vein thrombosis (5 patients), Budd-Chiari syndrome (3 patients). In 2 cases, TIPS placement was performed in external hospitals and the indication could not be determined. Patient characteristics are summarized in Table 1. In all cases, the experienced examiner succeeded in assessing the ultrasound flow of the TIPS, although in one case (1.6%) it was heavily restricted by the external sound conditions. Therefore, this examination had to be excluded.
Patient characteristics
Patient characteristics
Flow assessments in the stent graft by both methods were successful in all remaining examinations (n = 60, 98.4%). In five cases (8.3%), the flow rating did not differ between the two methods; in all other cases (55 examinations, 91.7%), the flow score was better by at least one rank level with HR-Flow/Glazing flow than with CCDS (p < 0.001); by one rank level in 50 examinations and by 2 rank levels in 5 examinations. Both methods showed a strong positive correlation (rs = 0.71; p < 0.001; 95% -CI: 0.53–0.87).
The independent reading resulted in values from 1 to 4 for the CCDS with an average of 2.52±0.54. The combination of HR-Flow and Glazing Flow resulted in a reduction of artifacts with a mean value of 3.52±0.57 (p = 0.013) (Fig. 1). The transition plot shows that the combination of HR-Flow and Glazing Flow resulted in an artifact reduction in 55 patients (91.7%) (Fig. 2), in 5 patients, HR-Flow/Glazing Flow and CCDS were ranked equally (8.3%). No loss of quality was observed. Figure 3 shows an exemplary comparison of CCDS and HR-Flow/Glazing Flow in the same patient. A complete freedom from artifacts (5 points) was not achieved due to the angle-dependent nature of CCDS. The detection of the low flow at the junction between the stent and the hepatic vein required an adjustment of the hemodynamic flow parameters to low speed ranges of <40 cm/s mean flow compared to up to 100 cm/s in the stent area.
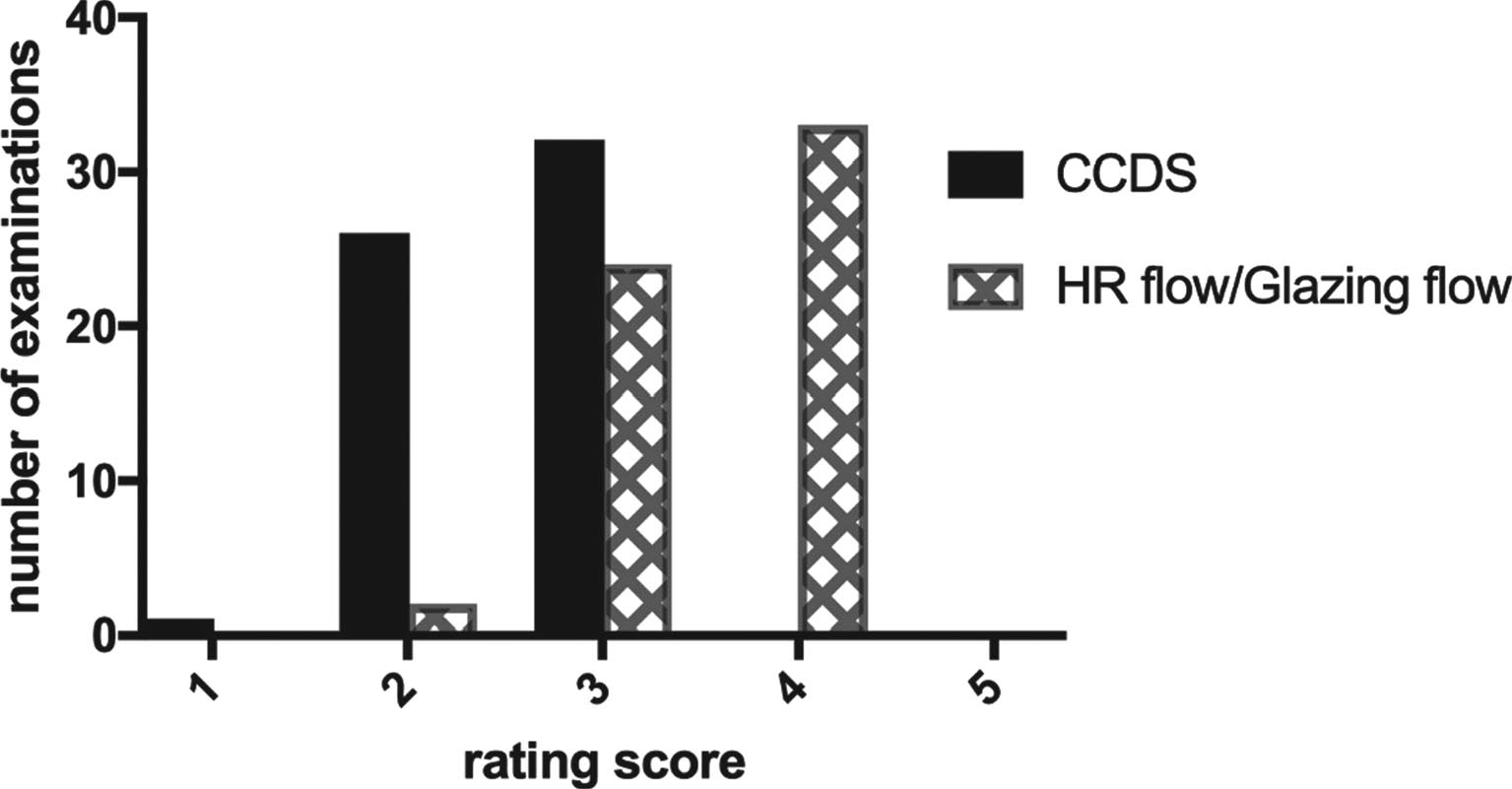
Column plot of the ultrasound rating for CCDS and HR-Flow/Glazing-Flow. 1, Flow assessment possible with massive artifacts. 2, Flow assessment possible with obvious artifacts. 3, Flow measurement partially overlaid with artifacts. 4, Almost complete imaging of the TIPS tract without artifacts. 5, Imaging of the entire TIPS tract with portal vein and hepatic vein confluence in one image without artifacts (was not achieved due to the angle-dependent nature of CCDS).
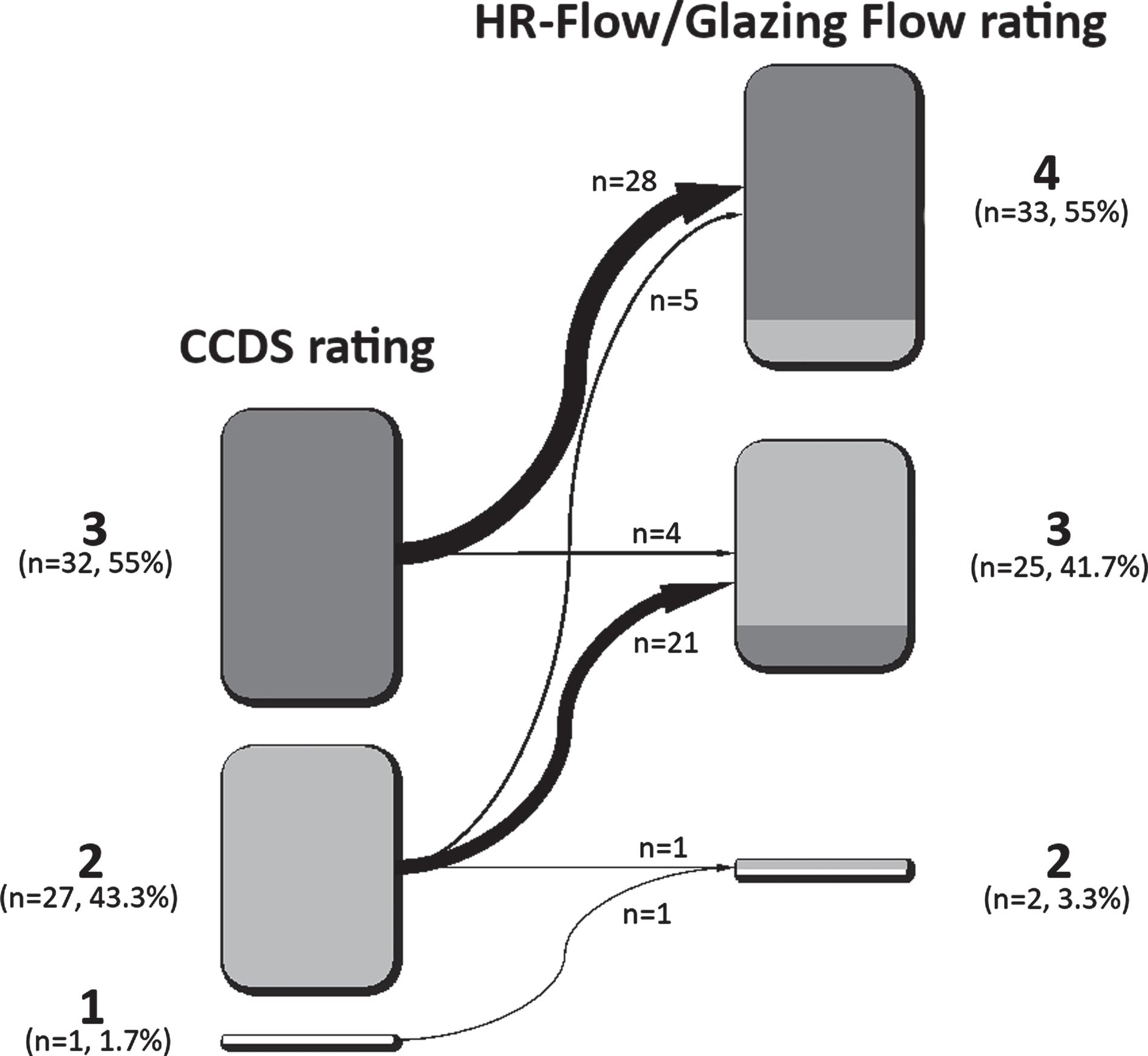
Transition plot of the ultrasound rating for CCDS and HR-Flow/Glazing-Flow. 1, Flow assessment possible with massive artifacts. 2, Flow assessment possible with obvious artifacts. 3, Flow measurement partially overlaid with artifacts. 4, Almost complete imaging of the TIPS tract without artifacts.
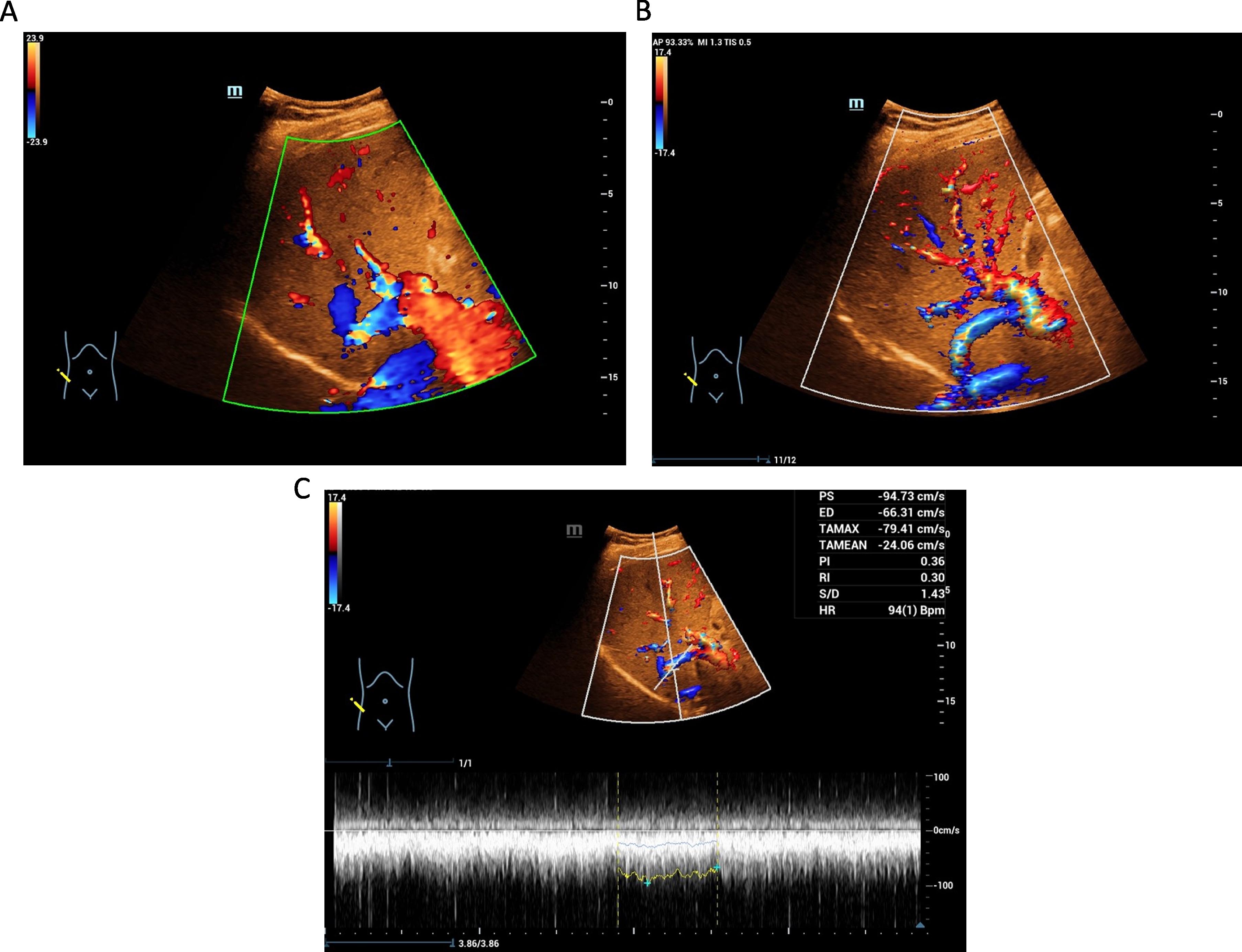
Ultrasound follow-up after TIPS placement in a 46-year-old patient with CCDS, HR-Flow/Glazing Flow and HR-Flow/Glazing Flow combined with Doppler ultrasound. A CCDS in intercostal plane with partial depiction of the stent-graft and the portal vein. Limited US quality with motion artifacts and pulsation artifacts. Rating: 3. B Complete depiction of the stent-graft with HR-Flow/Glazing-Flow in the same patient, without relevant artifacts. Rating: 4. C Combination of HR-Flow/Glazing-Flow and Doppler ultrasound in the same patient allows optimal assessment of the spectral curve with only minor artifacts. Rating: 4.
In all 60 cases examined, a flow assessment of the TIPS was possible with vascular ultrasound. For this purpose, the depth range had to be extended up to 25 cm and, if necessary, the patient had to be placed in left lateral position to optimize the Doppler angle. Furthermore, the mid-frequency of the sound probe was reduced to 2.5 MHz. In addition, ultrasound CT technology in B-mode was used to improve the visualization of the course of the TIPS.
For CCDS examination of the portal vein, the color velocity scale was regulated to 25 cm/s. Flow velocities of 25 to 59 cm/s were measured with an average of 38 cm/s±7 cm/s.
The liver veins were usually visualized via modified intercostal views. Here, a further lowering of the ultrasound frequency to <2 MHz could be helpful with adjustment of color velocity scale to 15 cm/s. We measured flow velocities of 12 cm/s to 33 cm/s, an average of 22 cm/s±7.5 cm/s in the hepatic vein. The measured diameters of the stent-graft were between 5 mm and 10 mm, with an average of 7.8 mm±1.2 mm. A stenosis of the stent tract with a diameter of less than 6 mm with flow velocities of <80 cm/s was considered relevant. In 3 cases, the depiction of kinks was done with cine loops with the possibility of a 3-D review in the PACS. Hypoechoic intraluminal band-shaped changes with a clear flow reduction <60 cm/s or no flow display in 2 cases were regarded as thrombus formation. The flow velocities in the stent-graft area were between 56 cm/s and 156 cm/s, with an average of 116 cm/s±17 cm/s.
In this pilot study, a combination of HR-flow and Glazing-flow improved the assessment of CCDS imaging of TIPS in the majority of cases. The combination facilitated Doppler spectral analysis and can therefore be valuable for the less experienced examiner in the US follow-up after TIPS placement.
The most important criterion in the US assessment of TIPS is the angle-corrected flow velocity measurement with a normal value of 90 –190 cm/s [9]. Low flow velocities below 60 cm/s can be caused by thrombosis in the stent-graft or post-stenotic reduction of flow [13]. High flow velocities of >200 cm/s also suggest hemodynamically relevant stenosis, e.g. due to kinking of the stent-graft. Another useful parameter is main portal vein velocity. After TIPS placement, main portal velocity typically increases to 30 cm/s [14]. If the main portal vein velocity drops below 30 cm/s, stenosis of the stent graft can be suspected [1].
The combination of HR-flow and Glazing flow uses a higher frame rate and a less angle-dependent digital detection of blood flow to improve assessment of low flow velocities even in difficult US conditions. Color gain, scale, color intensity and the range of flow velocity can be adjusted quickly by automated functions. Thereby, spectral Doppler analysis in the portal, midportion and hepatic segment of the stent-graft can be performed faster and more precisely; here phases of breath hold can be reduced or prevented completely by modified intercostal views and left lateral position.
The Advancing Liver Therapeutic Approaches group recommend TIPS venography and manometry with intervention in patients with CCDS findings suggesting TIPS dysfunction [15]. These findings include alterations in intrahepatic portal vein direction of flow and abnormal flow velocities within the TIPS.
There are some limitations to this study. Frequently, the transition from the stent graft into the hepatic vein lies deeply within the body, and the depth-regulation in B-mode had to be set to 20 cm and more. This restricts digital flow techniques because of their dependence of ultrasound frequency. In frequencies of below 2.5 MHz, assessment of flow is limited. In these cases, the ultrasound signal can be improved with contrast-enhanced ultrasound (CEUS), if necessary. Moreover, this is a retrospective, single center study with only a limited number of patients. Furthermore, the time between placement of TIPS and follow-up US varied greatly (0 –16 years). The results should be verified prospectively in direct comparison to catheter examinations.
Conclusions
In conclusion, the results of this pilot study suggest that the combination of HR-Flow and Glazing Flow results in improved flow representation within the stent-graft, reduction of artifacts and a facilitated hemodynamic assessment in the follow-up of TIPS with ultrasound.