
Abstract
BACKGROUND:
Neuromodulation is a therapeutic option to improve limb salvage in end-stage peripheral arterial disease (PAD), but there is no consensus on its indication for spinal cord stimulation (SCS) in PAD patients.
OBJECTIVE:
The aim of this study was to present the outcome of end-stage PAD patients treated with SCS.
METHODS:
This study is a retrospective analysis based on a local prospective registry. Neuromodulation was performed if there was: 1) no revascularisation option, 2) no septicemia, 3) and Rutherford stage 4–6. The primary endpoint of the study was limb salvage. Secondary endpoints were reduction in pain or simply pain reduction pain (assessed using a visual anlog scale/VAS) and improvement in walking distance.
RESULTS:
Limb salvage was reached in 30/34 patients (88%). Patients reported a significant reduction in pain on the 10-point VAS scale from baseline (median = 7.5, IQR = 7–8) to follow-up at 2 years (median = 0, IQR 0–2.75), p < 0.001. Walking distance also improved from preoperative (median = 50 m, IQR = 20–50 m) to follow-up at 2 years (median = 150 m, IQR 50–272 m), p < 0.001.
RESULTS:
SCS implantation in patients with end-stage PAD can enable limb salvage in a high percentage of cases and increase mobility due to pain reduction. The role of microcirculation in these improvements needs to be investigated in further studies.
Keywords
Introduction
Peripheral arterial disease (PAD) is a common manifestation of atherosclerosis and is associated with an increased risk of coronary artery disease and cardiovascular death [1–3]. In addition, critical limb ischemia (CLI) is a major problem in these patients. Despite improvements in vascular surgery, especially in endovascular techniques, the rate of major amputations in end-stage PAD is still high due to critical limb ischemia (CLI) associated with impaired wound healing and pain.
End-stage PAD is characterized by rest pain, ulcers, or gangrene in one or both lower limbs due to pre-existing peripheral arterial occlusive disease, in most cases worsened by diabetes. Up to 66% of patients with diabetes who are unsuitable for revascularization will require major amputation within 12 months [4]. The mechanisms that impair microcirculation in diabetic patients include increased wall stress with increased wall thickness, changed extracellular matrix, and microvascular decrease [5]. Measuring foot perfusion in patients with diabetes is difficult, because of Mönckeberg’s sclerosis in patients with incompressible arteries [6]. Toe systolic pressure might be an alternative but is associated with a wide range of measurement [7].
Various non-revascularization modalities have been proposed to reduce the major amputation rate in patients with end-stage PAD who cannot be treated with bypass or endovascular intervention. These modalities include prostaglandin treatment, pain management, sympathectomy, wound management, and neuromodulation through spinal cord stimulation [8]. Limb salvage may possibly be improved when spinal cord stimulation (SCS) is employed [9], but evidence is inconsistent [10]. A systematic review and meta-analysis reported a one-year amputation rate of 20% after SCS implantation [11]. To date, there are no European recommendations for SCS implantation in patients with PAD [12]; therefore, many clinicians remain skeptical about the value of SCS. Nevertheless, SCS is considered a therapeutic option in carefully selected patients [13]. Especially for patients with chronic, treatment-resistant pain who are not suitable for vascular reconstruction, SCS may be the last option to achieve pain relief, increased mobility (in order to enhance microcirculation), and limb salvage.
The present study was designed as a single-center study to assess the mid-term outcome (limb salvage, pain level, and walking distance) after implantation of an SCS device in patients with end-stage PAD.
Methods
Study design
This study is a retrospective analysis based on a local prospective registry (Center for Vascular Diseases Nuremberg) and includes patients with PAD Rutherford stage 4–6 [14] unsuitable for arterial reconstruction, who had been treated with spinal cord stimulation between 01/2017 and 12/2020. The study was approved by the Ethics Committee of the Bavarian Medical Association (reference number 19026) and registered with the Clinical Study Data Base of the University Hospital Regensburg before data analysis (Z-2016-0741-9).
Endpoints
The primary endpoint of the study was limb salvage, defined as heel preservation. Secondary endpoints were pain (assessed with a VAS ranging from 0 = no pain to 10 = highest possible pain) and self-reported walking distance. Both secondary endpoints were assessed preoperatively: at discharge from hospital and during follow-up. In addition, complications and adverse clinical observations after implantation documented in the medical records were used for the present analysis.
Inclusion and exclusion criteria
Inclusion criteria were leg pain and implantation of an SCS device for non-reconstructable PAD Rutherford stage 4–6. Exclusion criteria were septicemia or no SCS implantation (Figure 1). All patients had given their informed consent before SCS implantation.

Treatment options for PAD patients without reconstructive option. If the main symptom was pain, spinal cord stimulation was performed. Patients with septicemia underwent major amputation. Patients with no relevant pain and no septicemia were treated with lumbar sympathectomy. n = number of patients.
Patients who were referred to the Center for Vascular Diseases Nuremberg received standard diagnostics including sonography, MRI, and/or angiography. All patients with PAD were discussed in an interdisciplinary meeting of vascular surgeons and radiologists. The decision to implant an SCS device was based on the following criteria: (1) no revascularization option, (2) no septicemia, and (3) Rutherford stage 4–6 (Fig. 1). The ASA score of patients was determined by an anesthesiologist before implantation.
PrimeAdvanced SureScan (Medtronic, Minneapolis, US) with tonic stimulation was used for neuromodulation. This device is not rechargeable, has 8 electrodes, and is percutaneously implanted and MR proof. Procedures were performed in the operating theater under fluoroscopy and under local anesthesia according to Deer et al. [15]. Single-shot antibiotics were given before implantation. The electrode was implanted at Th 11–12, modifying the top of the electrode from the midline or raising it to Th 10 according to the patient’s report of paresthesia during intraoperative testing. Intraoperative testing to measure impedance and presence of paresthesia at the body site of choice was carried out in all patients. The generator was placed in the gluteal region. The SCS device was permanently implanted from the very beginning. Thus, the temporary insertion of electrodes in the context of a “trial phase” (a procedure often conducted by neurosurgeons, 15) was circumvented in order to avoid electrode-associated infections. In addition, patients with PAD Rutherford stage 5 and 6 received prostaglandins, wound management, and, if needed, antibiotics. Patients with PAD Rutherford stage 4 had only received single-shot antibiotics before implantation (Table 1).
Multimodal therapeutic concept in treating PAD patients with neuromodulation
Multimodal therapeutic concept in treating PAD patients with neuromodulation
(according to Deer et al. [12]). # mean adjustments times on patients was 2 (range 1–12).
At discharge, our patients were thoroughly informed about the importance of wound management and supervised walking exercises in order to stabilize their health condition. They received prescriptions for specialized ambulatory wound management care and for walking exercises supervised by a physiotherapist.
All patients were followed-up according to their clinical needs, and their level of pain was assessed. Arterial perfusion was determined by ultrasound scan. SCS stimulation was re-adjusted in the follow-up phase according to patients’ preferences. Patients were offered follow-up examinations at 3, 6, 12, and 24 months.
Registry and documentation
All patients were diagnosed and treated at the Center for Vascular Diseases Nuremberg. Data were prospectively entered into an institutional database (M1, CompuGroup Medical) by trained staff throughout the observation period. Patient data were retrieved from this data base, pseudonymized, and then documented on a paper-based case report form (CRF), which was prepared for this study.
All patient-related variables were documented by the leading study physician (BC) and independently checked by a second person. Discrepancies were resolved by cross-checking with the original data in the data base (source data verification). CRF data were entered into a SPSS file for data analyses.
Statistical analysis
Descriptive statistics include counts, percentages, medians (Med), and interquartile ranges (IQR). The outcome variables pain and walking distance were not normally distributed; therefore, the Friedman test was used to calculate the difference across three assessment points: baseline, discharge from hospital, and last follow-up assessment. P-values < 0.05 were considered statistically significant. Because of the exploratory nature of the analyses, no adjustments for multiple testing were applied. Data were analyzed using SPSS version 26.0 (IBM, Armonk, NY, USA).
Results
Patient characteristics at baseline and compliance with follow-up assessments
From 01/2017 to 12/2020, 4677 patients with Rutherford stage 4–6 were seen at our center, of whom 34 (0.7%) received an SCS implant because of non-reconstructable PAD Rutherford stage 4–6 (Table 2). The technical success rate in terms of correct placement of the electrodes was 100%.
Patient characteristics, comorbidity, PAD stage, and number of major amputations
Patient characteristics, comorbidity, PAD stage, and number of major amputations
*Median and interquartile range (IQR)
In each of the 34 patients, pain and walking distance were measured at baseline and at discharge from hospital. One patient was unable to walk due to muscular dystrophy, resulting in a walking distance of 0 m. The number of patients complying with follow-up visits was n = 24 at 3 months, n = 23 at 6 months, n = 23 at 23 months, and n = 14 at 24 months.
Limb salvage was achieved in 30/34 (88%) patients in the follow-up period. One major amputation was performed before hospital discharge due to progressive septicemia. Three amputations had to be performed in the course of follow-up, 2 months after SCS implantation. All of the 4 patients who underwent major amputation were men, had diabetes and coronary heart disease, had received minor amputation in the preceding 6 months, and were classified Rutherford stage 6.
24/34 (71%) of the patients had diabetes, of whom 7/24 (29%) had minor necrosis at the time of SCS implantation. 10/24 (42%) patients had Rutherford stage 6 with gangrene, of whom 4/10 (40%) patients required major amputation during follow-up. Limb salvage was achieved in 20/24 (83%) of these patients with diabetes.
Pain
Patients had a significant decrease in pain from baseline (n = 34, Med = 7.5, IQR = 7–8) to discharge (n = 34, Med = 5.5, IQR = 5–7; Fig. 2). A Friedman test comparing medians over time in patients for whom assessments at all time points were available was statistically significant: Chi2 (N = 9, df = 5) = 40.99, p < 0.001.

Pain scale before and after SCS implantation. Pain was assessed preoperatively and postoperatively using a visual analogue scale (0 = no pain, 10 = highest possible pain) that was documented by the physician preoperatively (baseline), at discharge, and during follow-up. Patients had a significant pain decrease from baseline (n = 34, Med = 7.5, IQR = 7–8), to discharge (n = 34, Med = 5.5, IQR = 5–7), at 3 month-follow-up (n = 24, Med = 4, IQR = 3–5), 6 month-follow-up (n = 23, Med = 3, IQR = 2–5), 12 month-follow-up (n = 23, Med = 2, IQR 0–4), until 2 year-follow-up (n = 14, Med = 0, IQR 0–2.75).
Patients had an increased walking distance from baseline (n = 34, Med = 50, IQR = 20–50) to discharge (n = 34, Med = 50, IQR = 17.7–50; Figure 3). A Friedman test comparing medians over time was statistically significant: Chi2 (N = 12, df = 5) = 39.59, p < 0.001.
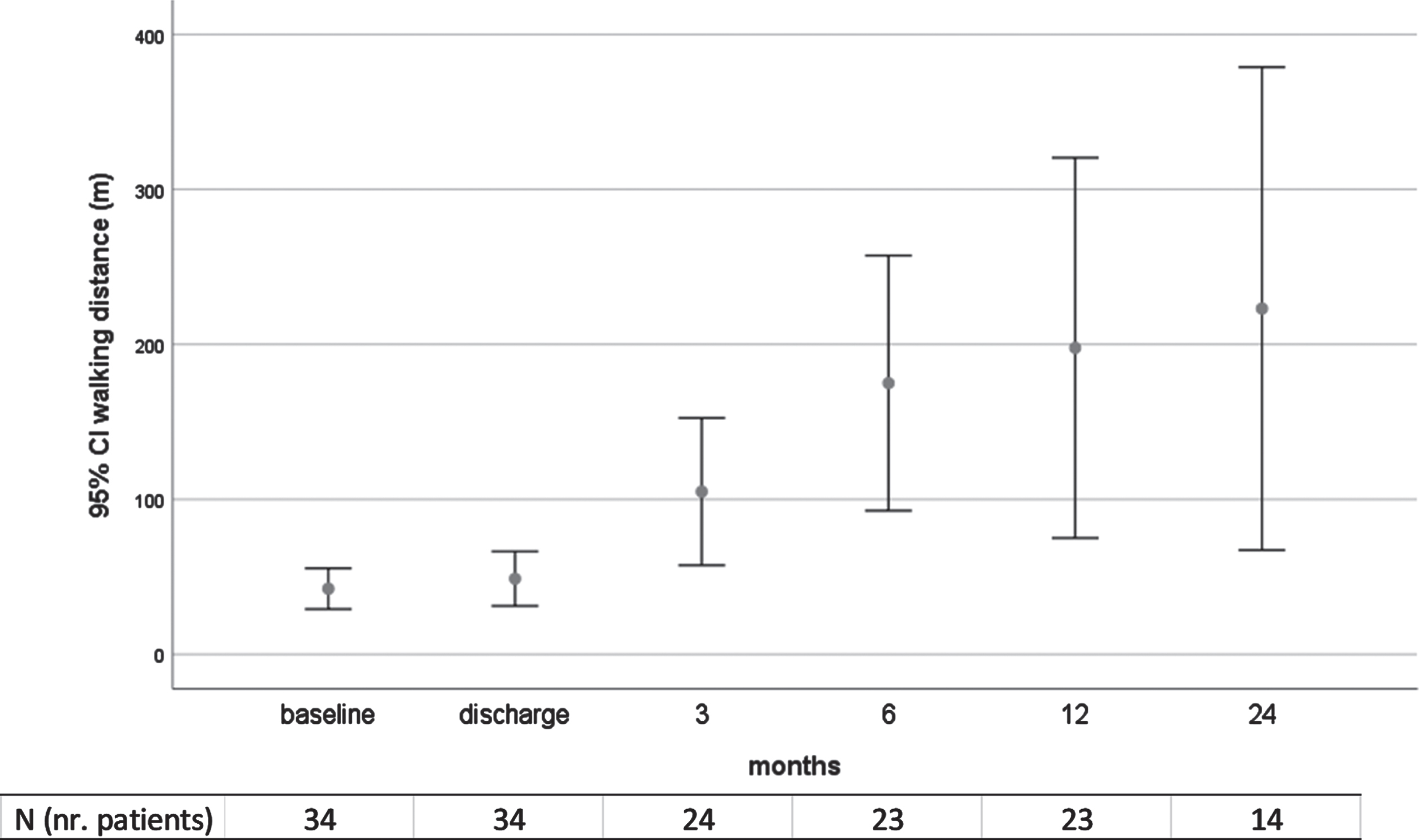
Walking distance of patients. In case of patients with major amputation, the walking distance was set at 0. One patient with muscular dysthrophy received SCS due to pain and non-healing ulcera; in this case, the walking distance was also set at 0 m. The patient had increased walking distance in meters: from baseline (n = 34, Med = 50, IQR = 20–50) to discharge (n = 34, Med = 50, IQR = 17.7–50), at 3 month-follow-up (n = 24, Med = 100, IQR 27.5–175), 6 month-follow-up (n = 23, Med = 100, IQR 50–200), 12 month-follow-up (n = 23, Med = 100, IQR 50–212.5), until 2 year-follow-up (n = 14, Med = 150 m, IQR 50–272). Follow-up was mean 17.9 months (range 1–39), 14 patients completed at least 2 years of follow-up.
From 01/2017 until 12/2020, SCS implantation was performed in 34 patients with intraoperative testing to avoid electrode malfunction (Table 1). In 2/34 (6%) cachectic patients, gluteal placement of the generator caused impingement pain of the sciatic nerve, requiring device removal. One (3%) patient with urinary incontinence developed generator infection after one month. The technical success rate was 100%.
Three patients died after two months (two after major amputation, one due to pneumonia). One patient died after 4 months (with major amputation), and one patient died after 2 years due to pneumonia. The fourth patient with major amputation was followed-up for 13 months and was then lost to follow-up.
Discussion
Outcome was evaluated after SCS implantation in patients with end-stage PAD who were not suitable for open arterial or endovascular reconstruction. If necessary, stimulation was regularly adjusted, and wounds were managed subsequent to SCS implantation. Pursuant to intraoperative electrode testing, the technical success rate was 100%. The infection rate was low (3%) and compared well with previously reported infection rates of 3% to 12% [10, 17].
Significant pain decrease leading to increased patient mobility was achieved in almost all patients at hospital discharge and at their last follow-up. Although SCS is not considered to result in permanent pain relief [12, 24], patients in this study had reduced pain after SCS implantation, which increased their mobility. This increase in mobility may explain the long-term pain relief in these patients.
The one-year amputation-free rate was 88% in the present patient group, which is similar to that of 80% reported by other investigators [11, 25]. 16/34 (47%) of patients experienced an increase in walking distance. Liu et al. reported an increase in walking distance from 64.86±40.80 to 1595.00±483.60 m in 37 patients with SCS [25]. Patients who had been unable to walk at baseline seemed to have obtained some benefit from SCS implantation. Whether these patients should be excluded from SCS treatment requires further evaluation. A Cochrane review confirmed increased mobility in patients with SCS compared to patients receiving conservative treatment alone [18].
In the present study, we instructed patients to engage in walking exercises and we observed both, decreased pain after implantation and increased mobility. To what degree walking exercises as such or the SCS device contributed to the increase in walking distance cannot be determined but is an interesting topic for further research. SCS may induce vasodilatation and improve microcirculation due to sympatholytic vasodilatation [19, 20]. Recent studies have doubted the effect of sympathetic vasodilator fibers in human limbs [20]. Hence, the positive effect of SCS on PAD stage might be induced by pain relief and therefore increased walking exercises. Shear stress of the vessels is increased, and therefore microcirculation and collateral network are improved due to activation of arteriogenesis [21]. The degree of arteriogenesis may be measured by changes in concentration of small non-coding RNA, miRNA [21]. Studies on this topic to measure SCS improvement of microcirculation in the limb are planned.
More accurate measurement of transcutaneous oxygen with TcpO2 may facilitate the evaluation of collateral vessel improvement after SCS implantation [23, 35]. However, 71% of patients in this study had diabetes with PAD and a high level of infection. Measurement of foot perfusion with TcpO2 or by hyperspectral camera might fail due to the heterogeneity of these patients with infection of the skin, non-healing ulcers, and altered microcirculation due to diabetes [29, 37]. These conditions may also impact measurements of velocity of erythrocytes [32]. Moreover, vessel diameter does not seem to increase patency rate [30], hence microcirculation measurement needs new markers, as diameter measurement and TcPO2 might be not suitable. Biomarkers, for example miRNA (e.g. miRNAs 126, 142, 195, and 197) may be an alternative [31].
Burst stimulation seems to reduce pain even better than tonic stimulation [26]. So far, no evidence concerning neuromodulation through burst waveform in patients with PAD has been presented, but this issue deserves evaluation.
In 87 patients treated with SCS, Gersbach et al. found that diabetes was a significant risk factor for major amputation during follow-up [22, 27]. Tshomba et al. reported in 101 patients with non-healing ulcers that the only predictive factor for functional success was delaying the time between the onset of ulceration and SCS [16]. In the present study, patients with diabetes did not show any higher major amputation rate. All patients requiring major amputation had Rutherford stage 6 and minor amputation soon after SCS implantation. Although patients with Rutherford stage 6 are at high risk for major amputation, we still would not exclude them from treatment with neuromodulation. Multi-modal treatment with wound management, antibiotics if needed, prostaglandins, and supervised walking exercises may contribute to limb salvage, even in patients with Rutherford stage 6.
Major amputations were not observed after 6 months of follow-up. This finding is consistent with that of Gersbach et al., who found that the beneficial effects of SCS in patients with CLI persist far beyond the first year of treatment and that major amputations become infrequent after the second year. A recent study has demonstrated increased blood perfusion in rats only 10 weeks after SCS implantation [28]. In the present study, if minor amputation was performed within 6 months after SCS implantation, patients were at high risk for major amputation.
Limitations of the present study relate to the retrospective design, the small number of patients, and the lack of a control group. Therefore, in order to confirm and extend the present findings, prospective studies comparing various modes of SCS with other pain relief treatments are warranted.
In conclusion, the present retrospective study provides preliminary evidence that in patients with PAD, one-stage SCS implantation combined with wound management and walking exercises and, if necessary, SCS stimulation readjustments leads to a reduced number of amputations, considerable pain reduction, and thus increased mobility. Further studies are needed in order to elucidate the interplay between SCS stimulation, pain relief, increased mobility, and microcirculation.
Authors’ contributions
The authors confirm contribution to the paper as follows: study conception and design: BC; data collection: BC, HH; analysis and interpretation of results: BC, MK.; draft manuscript preparation: BC, MK, TN, WS. All authors reviewed the results and approved the final version of the manuscript.
Footnotes
Acknowledgments
We are grateful to Monika Schöll for her linguistic advice and to Ronja Pfleiderer for the revision of the manuscript.