
Abstract
BACKGROUND:
Thalassemia patients have reduced red cell deformability and decreased plasma zinc levels in their blood.
OBJECTIVE:
This study aimed to evaluate the effects of zinc (Zn) on the hemorheological parameters and antioxidant enzyme activities in β-thalassemia major (TM) and healthy volunteers (HV).
METHODS:
Hemorheological parameters were measured using LORCA (laser-assisted optical rotational cell analyzer) after adjusting the hematocrit to 40%. Zinc sulfate (ZnSO4.7H2O) was used for Zn incubation with a concentration of 0.5μg/dl. Oxidative stress and antioxidant status were determined using commercial kits.
RESULTS:
Data showed that after Zn incubation, EImax, the area under the EI-osmolarity curve (Area), and Omax decreased in TM. However, no significant difference was observed in the osmotic deformability parameters of HV. The increased elongation index was obtained at different shear stresses for TM and HV, and SS1/2 decreased in both groups. The AMP and aggregation index (AI) decreased in TM, and the required time for half of the maximum aggregation (t1/2) increased in HV. However, Zn did not affect oxidative parameters in both groups.
CONCLUSIONS:
This study showed that Zn incubation increased deformability and decreased aggregation in thalassemic erythrocytes. It means that Zn supplementation will contribute to microcirculation in thalassemia patients.
Introduction
β-thalassemia major (TM) is one of the hereditary autosomal recessive disorders characterized by a genetic mutation resulting in reduced synthesis of beta hemoglobin chains [1]. Individuals usually apply for medical support when they are under two years old and always need regular blood transfusions to survive. Clinical features of TM in untreated individuals are; growth retardation, pallor, jaundice, weakness in the muscular system, crooked leg, hepatosplenomegaly, extramedullary hematopoiesis, and skeletal changes due to bone marrow enlargement [2, 3].
Zinc (Zn) is a trace element that acts as the cofactor of more than 300 enzymes. It is essential in growth, development, wound healing, and the immune system. As a result, the usual symptoms of Zn deficiency are growth retardation, male hypogonadism, loss of appetite, mental lethargy, and delayed wound healing [4, 5]. On the other hand, many studies showed Zn deficiency in thalassemia major patients might be due to the excretion of excess Zn with urine related to iron chelation therapy and insufficient nutritional intake [6–10]. Arcasoy et al. showed significantly lower (p < 0.01) Zn levels in all thalassemia patients compared to the control [6]. Karunaratna et al. found a serum Zn level of 44.7±24.2μg/dl, significantly lower than the control (63.3±30.3) [7]. In another study, Mahyar et al. showed that 28/40 of TM patients had a serum Zn level less than 70μg/dl (called hypozincemia) with a mean value of 67.35μg/dl [8], and also Zekavat et al. published a study showed significantly lower serum Zn level in TM patient, receiving iron chelation therapy, compared to the control group (mean values: 35μg/dl vs. 173μg/dl) [9]. Sultan et al. showed a low Zn level in TM patients who used an iron chelator in another study. 22.2% of these patients had less Zn than 50μg/dl [10].
Hemorheology examines plasma and blood cells, flow properties of blood, and behavior such as blood viscosity, red blood cell (RBC) deformability, and aggregation [11]. Erythrocyte deformability is essential, particularly while the erythrocytes pass through narrow capillaries. It depends on the surface/volume ratio (S/V), cytoplasmic viscosity, and membrane viscoelasticity. Membrane viscoelasticity also depends on membrane lipid composition and cytoskeleton properties [12]. In many clinical studies, the relationship between blood flow and the severity of circulatory diseases has been confirmed [13, 14]. The alterations observed in these pathological conditions are called “hemorheological abnormalities” [15] and are demonstrated in thalassemia patients [16–18]. Several researchers have investigated the effects of Zn on hemorheological parameters, and some of these studies showed that Zn supplementation increased erythrocyte deformability in healthy individuals [19] and sickle cell patients [20]. Another study showed the effect of Zn on the osmotic fragility that increased in zinc-poor-fed rats but improved with zinc-rich feeding [21]. Since Zn deficiency has been demonstrated in TM, it is mostly recommended as a supplementary agent in the clinical procedure. The investigations on the effect of Zn on the hemorheological parameters of thalassemic erythrocytes are insufficient and still need to be done. Although Zn supplementation is recommended to patients in the clinics, this study will show for the first time in the literature whether there is any benefit to patients regarding hemorheological factors.
The body’s antioxidant systems reduce tissue damage by decreasing lipid peroxidation. Thalassemia patients need repeated blood transfusions which cause iron overload, leading to peroxidative damage in erythrocytes. Therefore, antioxidant enzyme systems are activated to prevent these harmful effects of oxidative stress on the tissues. These antioxidant enzymes include superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx). Malondialdehyde (MDA) is a lipid peroxidation product used to determine lipid peroxidation [22]. Various studies found MDA and SOD levels significantly raised while CAT and GPx levels decreased in TM compared to controls [23–25]. They suggested that iron overload may cause this high MDA level due to repeated blood transfusions and subsequent oxidative stress. The high values in the SOD enzyme may arise due to compensatory mechanisms in response to oxidative stress [22–26].
This study investigated the Zn effects on hemorheological parameters and some antioxidant activities in TM. Thus, we tried to explain the possible relationship between Zn deficiency and decreased deformability in TM. In addition, we aimed to show whether the hemorheological parameters of thalassemia patients would improve if Zn deficiency were prevented.
Methods
Patients, sampling, and RBC suspension preparation
The Ethics Committee approved this study of Istanbul University, Istanbul Faculty of Medicine (IRB: 61/2018), and the protocol followed the Declaration of Helsinki guidelines.
Thalassemia patients were obtained from the Department of Pediatrics, Division of Hematology/Oncology of Istanbul Faculty of Medicine (Istanbul University, Turkey). Before their routine blood transfusion treatment, heparinized fresh venous blood samples were collected from 28 TM patients. Patients who had blood transfusions in the last three weeks were excluded. Although all of them are on iron chelation therapy, these patients suffer from iron overload (Table 1). Also, 30 healthy volunteers (HV) were included in this study as a control group, mainly from students of the medical school who did not have any blood disease that might be effective on hemorheological parameters, both themselves and their families. Also, they had not had any health-related complaints in the past month. Firstly, hematocrit (Hct) was measured using the microhematocrit method (9000 rpm, 4 min). The whole blood was centrifuged at 3000 rpm for 10 min. Then, the Hct was adjusted as 40% for the hemorheological parameters via adding or discharging native plasma. Erythrocyte lysate was prepared for enzyme activities following the storage procedures of assay kits.
Ferritin, UIBC, and iron levels in TM patients
Ferritin, UIBC, and iron levels in TM patients
The thalassemia and healthy erythrocyte lysates, which were stored at –80°C, were measured using the Elabscience (E-BC-K137-M) kit. The measurement principle is based on detecting the change in color resulting from the reaction of zinc levels in the lysates with 5-Br-PADAP, which is then measured at 560 nm. The indicated procedure by the kit was followed. In short, the samples diluted in 1:4 ratio were centrifuged at a speed of 13,780 g, and the supernatant was collected. The supernatant was then incubated with chromogenic reagent in 1:1 ratio and measured using a plate reader. The obtained absorbance values were substituted into a formula obtained through standard samples to calculate the zinc concentration.
Incubation of erythrocytes with zinc
Preparation of zinc (Zn) solution: In the beginning, we noticed that there was still a lack of international standards for physiological zinc experiments, and we had to try different methods previously used in the studies. Therefore, like all beginners to the Zn studies, we encountered some unexpected problems, in particular, dependent on the choice of Zn dose, anticoagulant, and suspension medium. We used ZnSO4.7H2O (Zinc Sulfate Heptahydrate) and accidentally chose PBS as the solution. However, unexpectedly, we observed precipitation. Then, we found another study by Ollig et al. [27], which showed that ZnSO4 reacts quickly with phosphate anion in PBS and Zn-phosphate precipitates. Finally, we used distilled water to solve ZnSO4. In our previous hemorheological studies, we mostly used vacutainer tubes with EDTA. In addition, some other studies with Zn also used EDTA [28, 29]. Therefore, in the beginning, we used EDTA-covered tubes. However, an agglutination occurred when we added the Zn solution to the blood sample. Then, we found the reason for this problem in the literature. According to Neumaier et al., EDTA acts as a strong Zn-chelator [30]. Hence, we replaced our EDTA-covered sample tubes with heparinized ones.
Another problem was Zn concentration which was used in experiments. According to previous studies, there was not any consensus on the Zn amount in solutions and incubation time. Dash et al. used 1,5μM concentration and 20 minutes of exposure time [31]. On the other hand, Khaled et al. used four different concentrations from 0.25 to 2 mg/l with a 30 min incubation time [29]. This group also showed that a low dose did not show any effect, but a little high dose showed a significant effect [19]. Taylor et al. conducted the experiments with a zinc content just above the physiological level. Their incubation time was an hour in autologous plasma [20]. Hence, we conducted a preliminary study involving six healthy volunteers with a Zn-dose series from low to high doses to solve these problems and design the study using healthy volunteer blood samples. Four tubes were prepared by taking 2 ml from each blood sample with a Hct of 40%. Then, all the tubes were centrifuged again (3000 rpm, 10 min). Stock ZnSO4 solution (0.145 M) was replaced with plasma to have a final concentration of 0.25, 0.50, 0.75, and 1μg/dl per individual. All tubes were incubated for 30 minutes in a water bath at 37°C. Then, we chose deformability measurement as the comparative parameter. At the end of these measurements, we observed the following results; 0.25μg/dl Zn did not affect the red cell deformability, 0.5μg/dl Zn increased, but 0.75μg/dl and 1μg/dl decreased deformability compared to initials. So, we accepted 0.5μg/dl as the most convenient dose with positive effects on deformability parameters but has no hazard.
As a result, we designed the following method: 1M ZnSO4.7H2O (Merck KGaA, Darmstadt, Germany) was used for the Zn incubation. Zinc sulfate was dissolved in distilled water. Then, 0.145 M zinc sulfate stock solution was prepared and diluted with 1/100 distilled water for the experiments. 3 ml of blood with a Hct of 40% was centrifuged (3000 rpm, 10 min). The zinc sulfate solution was replaced with autologous plasma to a final Zn concentration of 0.5μg/dl in plasma. This erythrocyte suspension was incubated for 30 minutes in a water bath at 37°C.
Hemorheological measurements
RBC deformability, aggregation, and osmotic deformability were measured in the blood samples of all subjects before and after the Zn incubation as follows:
Erythrocyte deformability measurement
RBC deformability was measured by a laser-applied ektacytometer [LORCA (laser-assisted optical rotational cell analyzer); MaxSis, Mechatronics, Hoorn, Netherlands]. In this method, was applied ten different shear stresses (SS) from 0.3 to 50 Pascal (Pa) at 37°C and defined as elongation index (EI). The method that we used in this study was described by Hardeman et al. [32, 33] Maximal erythrocyte elongation index (EImax) and the SS required for one-half of this maximal deformation (SS1/2) were calculated using the Lineweaver-Burke (LB) model. This model shows that increased SS1/2 indicates decreased RBC deformability [32, 33]. 25μl of blood with an adjusted Hct of 40% was added to 5 ml of polyvinylpyrrolidone (PVP) solutions (Mechatronics, Hoorn, Netherlands, viscosity: 28.9±0.5 mPa.s) and then mixed gently. Approximately 1.5 ml of this mixture was placed into the system’s chamber for measurement.
Osmotic deformability measurement
The erythrocyte osmotic deformability was also measured at 37°C using the osmoscan unit of LORCA, applying a constant SS of 30 Pa. Parameters calculated are (EImax): maximal elongation index, (EImin): minimal elongation index at low osmolar conditions, (EIhyper): measurable elongation index at high osmolar conditions, half of the maximum elongation at high osmolar conditions, (Omin): osmolarity at minimum EI, (Omax): osmolarity at maximum EI, (Ohyper): osmolarity at EI hyper, and (Area): area under the osmolarity-EI curves [34].
In this method, 250μl of blood, adjusted Hct of 40% with autologous plasma, was added to 5 ml of PVP solution (Osmolality: 296 mOsm/kg), gently mixed, and placed in the osmoscan system. While the osmolality of the suspension medium gradually changed from 100 mOsm/kg to 500 mOsm/kg automatically, the erythrocyte elongation as a measure of RBC deformability was continuously recorded.
Erythrocyte aggregation measurement
LORCA was used for the RBC aggregation measurements, as mentioned by Hardeman et al. Aggregation parameters are described as follows: AMP: amplitude or extent of aggregation, t1/2: is the time of half of the complete aggregation; and AI (aggregation index): expresses the kinetics of aggregation [35]. Approximately 1.5 ml of whole blood, previously adjusted to 40% Hct with autologous plasma, was placed in the device system and measured automatically.
Determination of oxidative stress and antioxidant status
According to the manufacturer’s procedures, the enzyme activities of SOD, CAT, GPx, and MDA were studied in erythrocyte lysates by assay kits (Cayman Chemical, Michigan, USA). 96-well plates were used for enzyme assays. Measurements were made spectrophotometrically by a plate reader (Hybrid Reader, Synergy H1, BioTek, VT, USA) and calculated from the standard graph curve except for the GPx assay, which was measured by a time scale.
Statistical analyses
IBM SPSS 22.0 (Statistical Package for Social Sciences) was applied for statistical measurements. Data were presented as mean±standard deviation. The Shapiro-Wilks test was used for assessments of the normality of data. Wilcoxon Sum Rank test was applied to evaluate dependent groups for the nonparametric data, and Mann Whitney U analysis was applied to evaluate independent groups. p≤0.05 was accepted as significant.
Results
This study included 28 TM patients (15 women and 13 men) (TM group) aged 10 to 41. The mean age was 22.9±8.83 years old. There were 30 subjects (17 women and 13 men) in the HV group, aged 15 to 38, with a mean age of 21.3±4.92 years old. The Hct of the TM and HV groups was 28.89±3.15 and 42.43±4.41, respectively. The Hct of the TM group was significantly lower than the HV group, as expected (p≤0.001). The initial Zn level was 26.61±2.04μmol/l in the TM group and 29.82±3.54μmol/l in the HV group. The difference was significant.
Erythrocyte deformability was evaluated via SS1/2, EImax, and EI at ten different SS. Table 2 shows all hemorheological parameters of HV and TM groups before and after Zn incubation. As shown in Table 2, the initial SS1/2 of the TM group was significantly higher (p = 0.008) than the HV group. After Zn incubation, there was a significant decrease in SS1/2 in both groups (p < 0.027 for HV, p≤0.001 for TM). Initial EImax was significantly lower in the TM than in the HV group (p≤0.001). After Zn incubation, EImax did not change significantly in either HV or TM groups. Initial EI at ten different SS of HV and TM groups were compared statistically, and the results were shown graphically in Fig. 1. As shown in Fig. 1A, EI data of the TM group obtained at 0.94 –1.65 –2.91 –5.15 –9.09 –16.04 –28.32 and 50 Pa SS1/2 were found significantly lower than the HV group (p = 0.004 –≤ 0.001 –≤ 0.001 –≤ 0.001 –≤ 0.001 –≤ 0.001 –≤ 0.001 –≤ 0.001 respectively). Data shown in Fig. 1B, EI of the HV group at 1.65 –2.91 –5.15 –9.09 –16.04 and 28.32 Pa showed significant increases (p = 0.048 –0.017 –0.004 –≤ 0.001 –≤ 0.001 –0.002, respectively). Figure 1C shows that the EI of the TM group at 0.53 –0.94 –1.65 –2.91 and 5.15 Pa showed a significant increase after Zn incubation (p = 0.020 –0.002 –≤ 0.001 –0.005 –0.022, respectively).

A) Comparison of HV and TM groups as initial B) Zn incubation effect on EI of HV group, C) Effect of Zn incubation on EI of TM group. Elongation indexes (EI) that measured at shear stresses (SS) from 0.3 to 50 Pascal (Pa). Data points are presented as mean±standard deviation. Significance (p < 0.05): *, and (p < 0.001): **
Erythrocyte deformability, osmotic deformability, and erythrocyte aggregation parameters comparisons of HV and TM groups before and after Zn incubation
Data are given as mean±standard deviation. SS1/2: Shear stress required for half-maximal deformation, EImax: elongation index maximum, (EImin): minimal elongation index at low osmolar conditions, (EIhyper): measurable elongation index at high osmolar conditions, half of the maximum elongation at high osmolar conditions, (Omin): osmolarity at minimum EI, (Omax): osmolarity at maximum EI, (Ohyper): osmolarity at EIhyper, and (Area): area below the osmolarity-EI curves. AMP: amplitude of aggregation, t1/2: aggregation half-time, AI: aggregation index, Pa: pascal, p1 = before and after Zn incubation of HV group, p2 = before and after Zn incubation of TM group, p3 = before Zn incubation, HV and TM groups (as initial), p4 = before Zn incubation of HV and after Zn incubation of TM groups.
Figure 2 presents cumulated EI-osmolarity curves. We found significant differences between some of the initial osmotic deformability parameters of the HV and TM groups (Table 2). The TM group’s initial Omin, Omax, and Ohyper were significantly lower than the HV group (p = 0.003 –0.01 –≤ 0.001, respectively). As seen in Table 2, there was no significant difference in the HV group’s osmotic deformability parameters after Zn incubation. On the other hand, there was a significant decrease in EImax, Area, and Omax parameters in the TM group after Zn incubation (p≤0.001 –≤ 0.001 –0.04, respectively). However, the differences in other parameters were not significant.
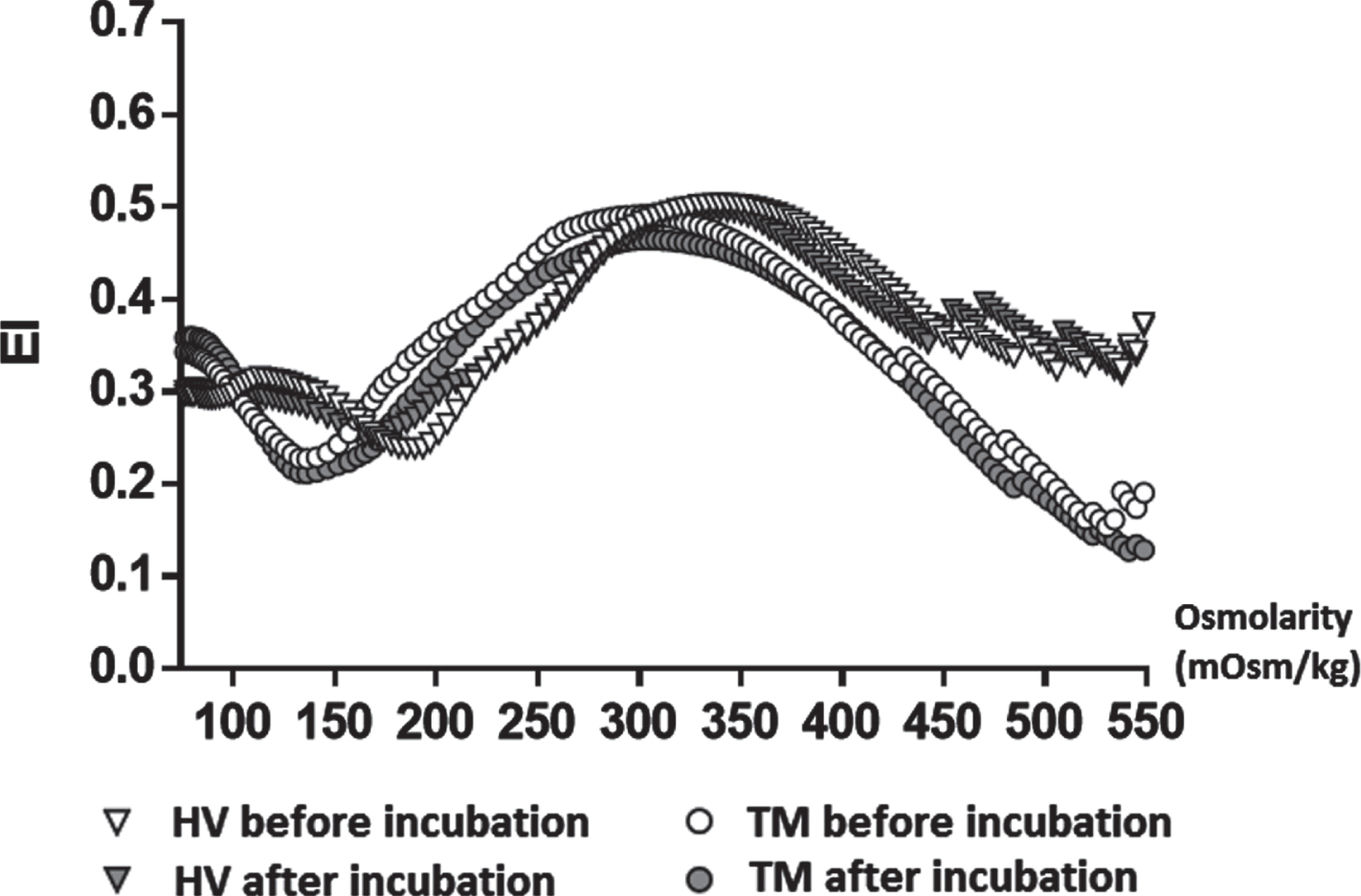
Cumulated EI-osmolarity curves measured before and after zinc incubation in the HV and TM groups.
Erythrocyte aggregation parameters measured in autologous plasma are shown in Table 2. According to the results, before Zn incubation, the initial AMP of the TM group was found to be significantly higher than the HV group (p = 0.011). In contrast, AI and also t1/2 were not significantly different in both groups. However, after Zn incubation in the HV group, there was a significant decrease in AI (p≤0.001) and a significant increase in t1/2 (p≤0.001). On the other hand, there was only a significant difference as a decrease in AMP (p≤0.001), but there was no significant difference in AI and t1/2 in the TM group after incubation.
Initial data of GPx, SOD, CAT, and MDA activities in HV and TM groups were analyzed, and the differences were not statistically significant. After Zn incubation, in comparing enzyme activities of the HV and TM groups, the differences were not statistically significant in both groups (Table 3).
Antioxidant enzyme activities and lipid peroxidation biomarker comparisons of HV and TM groups before and after Zn incubation
Data are given as mean (standard error). GPx: glutathione peroxidase, CAT: catalase, SOD: superoxide dismutase, MDA: malondialdehyde. p1 = before and after Zn incubation of HV group, p2 = before and after Zn incubation of TM group, p3 = before Zn incubation, HV and TM groups (as initial).
As we mentioned previously, many studies showed that Zn deficiency is a common problem for patients suffering from TM and may occur due to hyperzincuria depending on iron chelation therapy, high ferritin levels, liver failure, and insufficient nutritional intake [6–10, 37]. We also did measure Zn level in TM patients and HVgroups and we confirmed Zn deficiency in TM patients. In addition, previous studies have also shown that increased iron absorption from the gastrointestinal tract causes decreased Zn absorption in TM patients [7–9, 38]. All patients in this study have been using iron chelators continuously, and some Zn may be chelated in the autologous plasma during incubation. So, we checked some of the samples Zn level after incubation and we observed Zn level still higher after incubation. These results did not present in the manuscript, because, our primary goal was to investigate whether zinc would benefit thalassemia patients in their own conditions, since they must use chelators in their resting life.
Various studies showed that Zn increases erythrocyte deformability and decreases aggregation [19, 39]. Many studies have also demonstrated that Zn deficiency alters the plasma membrane composition [21, 40–42]. However, the hemorheological parameters presented in the previous studies were limited to blood viscosity and erythrocyte deformability [16–18, 44]. In the present study, we also measured the parameters of osmotic deformability and erythrocyte aggregation. The initial EI data of the TM group at low shear stresses were significantly lower than the HV group. Previously, some studies had shown significantly lower EI data compared to HV, which were similar to our data [16, 44–48]. Increased erythrocyte deformability at less than 3 Pa of SS is associated with increased membrane flexibility [49, 50]. In this study, Zn increased erythrocyte deformability at low SS in the TM group. So, it can be considered that Zn increased erythrocyte membrane flexibility in TM. In our study, the SS1/2 of the TM group was significantly higher than HV. In addition, EImax was found to be lower than the HV group, which might be due to increased membrane rigidity [51]. One of the most striking results of this study, the HV group showed a statistically significant decrease in SS1/2 after the Zn incubation. This result is important because decreased SS1/2 indicates increased RBC deformability [33]. In the literature on hemorheological studies regarding thalassemia, we could not find any result about SS1/2. Therefore, we supposed our result might be the first finding about these parameters.
We also measured osmotic deformability. We found that the TM group’s initial Omin, Omax, and Ohyper were significantly lower than the HV group. These findings are consistent with the study results previously performed by Singer et al. [52]. EImin represents the point at which the cells were maximally swollen and spherical [34]. As well, Omin is the osmolality where EImin occurs. It also reflects S/V and is associated with osmotic fragility [49, 51]. Based on this opinion, the low Omin of the TM group may result from an increase in S/V and/or an increase in membrane rigidity. Thalassemic erythrocytes are smaller than normal but have a surface area close to normal. For this reason, thalassemic erythrocytes have high S/V and become osmotically more resistant [51, 52]. According to our data, after incubation, both the curve shifts to the left, and the decrease in Omin mean decreased erythrocyte fragility in the TM group. These data are consistent with the study performed by Desouky et al. [43]. Shifting to the left of the Ohyper point may occur with the loss of osmotic water and Hb concentration changes and increased intracellular viscosity [51, 52]. According to our results, although Zn did not change osmotic deformability parameters significantly in HV, this effect was significant in the TM group. On the other hand, we have yet to find any previous results to compare. So, our paper might be the first study that examined the effect of Zn on the thalassemic erythrocyte’s osmotic deformability parameters.
Another important rheological feature of the blood is the tendency to form aggregates where the blood flow decreases, arranged like stacked coins called rouleaux. In our study, the initial AMP of the TM group was found to be significantly higher than the HV group, but the difference was found insignificant in AI and t1/2 parameters. The decrease in AMP and AI, also an increase in t1/2, are accepted as indicators of decreased erythrocyte aggregation [35]. Our results also showed that thalassemic erythrocytes have a higher tendency to aggregate and therefore constitute a risk group and observed a statistically significant decrease in AMP after Zn incubation. This finding indicates that Zn might have an important role in reducing aggregation. In addition, although the differences are not statistically significant, the decrease in AI and the increase in t1/2 after Zn incubation are supportive findings that reflect a tendency to decrease aggregation in TM.
TM patients require regular blood transfusions due to severe anemia. In addition, increased lipid peroxide levels, free radicals, and decreased antioxidant capacity cause oxidative stress [22]. Zn has antioxidant activity as well as various other properties [22]. In our study, although there were slight differences in enzyme activities, both initial and after Zn incubation data, there were no statistically significant differences between the HV and TM groups.
In conclusion, this study suggests that TM patients also constitute a risk group associated with microcirculation according to hemorheological parameters. On the other hand, Zn incubation significantly increased erythrocyte deformability and decreased erythrocyte aggregation in TM. Hence, this positive effect of Zn on thalassemic erythrocytes can reduce the risks associated with microcirculation and contribute to the prevention of anemia-related complications in patients. Zn supplementation may also improve treatment quality.
Footnotes
Acknowledgments
The authors are grateful to Dr. Michael W. Rampling (Imperial College, London, UK) for his help with native English.
Conflict of interest
The authors have declared that no conflict of interest exists.
Funding
This study was established from a Ph.D. thesis (Mukaddes Sinan) in Istanbul University, Institute of Graduate Studies of Health Sciences, and was supported by The Research Foundation of Istanbul University with a research number of 31192.