
Abstract
BACKGROUND:
Liver transplantation is a life-saving treatment in end-stage liver failure. Hemorheological features as blood fluidity and red blood cell aggregation may alter effective tissue perfusion, graft function and hemodynamic variables.
OBJECTIVE:
The aim of the study is to investigate effect of albumin infusion on red blood cell deformability and aggregation, blood viscosity and hemodynamics in liver transplant patients.
METHODS:
Seventeen live or cadaveric donors were included in this prospective study. Hemorheological and hemodynamic measurements were performed in order to evaluate the effects of albumin infusion in perioperative period.
RESULTS:
Erythrocyte aggregation was significantly reduced 90 minutes after albumin infusion (p < 0.01). Mean blood viscosity revealed significant decrease at 20 rpm and 50 rpm after 90 minutes of albumin infusion (p < 0.05). Plasma viscosity decreased significantly compared to the value before albumin infusion at 20 rpm (p < 0.05). Albumin replacement improved hemodynamic variables in patients with low blood pressure and cardiac index measurements (p > 0.05).
CONCLUSIONS:
Human albumin infusion led to decrease in whole blood and plasma viscosities, red blood cell aggregation and induced blood pressure and cardiac index elevation in perioperative liver transplant patients. Determination of hemodynamic and hemorheological effects of human albumin replacement in various patient populations may serve beneficial clinical data.
Introduction
Liver transplantation is a lifesaving treatment option for the patients with end stage hepatic diseases and acute organ failure due to viral, toxic, metabolic and traumatic insults. Lipid, protein and cellular contents of blood change during chronic liver diseases. For the reason, rheological properties of blood as red blood cell aggregation, deformability and viscosity alter during various clinical conditions such as liver insufficiency [1–3]. Blood fluidity may influence the incidence of vascular complications as thrombosis, stenosis or bleeding, in liver transplant patients. Moreover, graft perfusion most likely depends on rheological properties of blood. However, perioperative alterations in blood fluidity at liver transplantation were not investigated before. Addressing these alterations may raise awareness for perfusion insufficiency and reveal the factors affecting blood fluidity. Early recognition and prompt correction of perfusion disorders related with hemorheological alterations may improve graft survival at liver transplantation.
Albumin is the major plasma protein with various fateful functions in healthy individuals. It contributes to 80% of total colloid osmotic pressure. Albumin fastens numerous drugs and endogenous molecules, maintains microvascular integrity and acts as a potent plasma buffer with antioxidant properties. Albumin solution is frequently used for preserving plasma concentration and hemodynamic stabilization intraoperatively and during intensive care unit (ICU) stay after liver transplantation. It has been reported that albumin may affect the coagulation profile in many situations. In different studies, anticoagulant [4, 5], or procoagulant [6, 7] characteristics of albumin solutions continues to be discussed. Hemorheological effects of albumin infusion have been investigated in experimental and clinical studies and conflicting results were reported [8–12].
The aim of this prospective, single centered, clinical study was to investigate the perioperative hemorheological characteristics of liver transplant patients and discover the efficacy of albumin infusion on blood rheology and hemodynamics which may modify blood fluidity and graft perfusion by changing circulating erythrocyte manner (aggregation, deformability) and blood viscosity.
Methods and experiments
Patients and medical interventions
The study was approved by the Akdeniz University Hospital Medical Ethics Committee (06.03.2019/240). Informed consent for surgery, blood samples, and random albumin therapy was obtained from all participants according to the Declaration of Helsinki. Seventeen adult recipients with liver insufficiency who underwent transplantation from alive or cadaveric donors between March 2019 and January 2020 at Akdeniz University Hospital were included in this study. Ten donors were brain death cadavers and 7 liver donors were relatives of the patients. The exclusion criteria were as follows: patients younger than 18 years of age, patients with occult intravascular volume and/or blood loss intraoperatively that may lead to confusions in interpreting hemorheological results, unplanned and emergent transplantations.
Albumin infusion was ordered by the anesthetists intraoperatively or ICU physicians during ICU stay, according to plasma albumin concentrations and/or clinical hemodynamic findings. For the reason, perioperative total amount of albumin infusion varied among patients. Human Albumin (Human Albumin CSL BehringTM 20%, 200 g/l) solution was infused in 20–30 minutes, intravenously. Crystalloid fluid replacement of 5 ml/kg.h–1 was continued simultaneously with the albumin infusion. Ongoing vasoactive drug infusion (noradrenaline) rate was not changed during albumin infusion.
Specimen collection and hemorheological analysis
Blood specimens were collected to EDTA tubes (1.8 mg EDTA/ml blood) for analyzing red blood cell deformability, aggregation, plasma and blood viscosity intraoperatively and after ICU admission, before and after (at 15 and 90 minutes) albumin infusion. Blood samples were withdrawn only for the first dose of albumin infusion despite numerous (mean 5,65±2,28 vials) human albumin solutions were infused intraoperatively. The aim of this delimitation was to refrain from potentially misleading factors in terms of hemorheological properties such as hemodynamic alterations, infusion of blood products and vasoactive agents which may frequently occur during dissection phase of liver transplantation. Blood samples were transported to hemorheology laboratory and analyzed immediately to get most accurate results of blood fluidity.
Hemodynamic variables such as invasive blood pressure, pulse rate, central venous pressure and cardiac index (CI), systemic vascular resistance index (SVRI), global end-diastolic index (GEDI), extracellular lung water index (ELWI) were recorded (PICCO catheterTM, Getinge AB, Sweeden) simultaneously with blood sampling in the course of albumin infusion. Blood gases, blood cell count, hematocrit (Hct), albumin and fibrinogen analyses were also performed at aforementioned study intervals.
Hemorheological analysis
Whole blood (ηb) and plasma (ηp) viscosities were determined by using a rotational viscometer (Brookfield DV-II Viscometer) performing shear rates of 20 and 50 rpm at 37’C. Ectacytometer (LORRCA, RR Mechatronics) was used to detect blood cell deformability by analyzing laser diffraction at various fluid shear forces at 37’C. Deformability was calculated as elongation index (EI) between nine different shear forces (0,30 –75,02 Pa). A shear force, causing a shape change of 1/2 maximum elongation index for each EI value was called as SS1/2. Red blood cell aggregation was determined in autologous plasma at 37’C by using a photometrical aggregometer. Aggregation rate (AI) was calculated by detecting light conductivity changes of blood sample after 10 seconds of rotation at 500 sn–1 shear rate. Also, index of erythrocyte rigidity “Tk” was calculated according to the equation of Dintenfass: Tk = (ηr0.4 –1) / (ηr0.4 · Hct), where ηr was relative blood viscosity (ηb/ηp) [13].
Statistical analysis
Results were analyzed by using ‘GraphPad prizm 5’ program. Repeated measures One-way ANOVA and posthoc Tukey’s test were used for comparison of various groups. Two-group analysis was performed with Student-t test. P < 0.05 was defined as statistically significant. Values were demonstrated as mean±standard error.
Results
17 patients were included in the study. The demographic data of the patients, CHILD and MELD-PUGH scores, durations of intubation and ICU were summarized in Table 1.
Liver transplant patient’s demographic data
Liver transplant patient’s demographic data
Footnotes: n = number of patients. Datas are presented as mean±S.E.M.
EImax, SS1/2, AI, whole blood and plasma viscosity parameters of the patients were evaluated intraoperatively before albumin infusion (Pre-A), 15 and 90 minutes after albumin infusion (A-15 min. and A-90 min.).
There was no statistically significant difference in EImax (Pre-A: 0,634±0,015; A-15 min.: 0,652±0,019; A-90 min.: 0,655±0,017) and SS1/2 (Pre-A 3,954±0,316; A-15 min.: 4,027±0,447; A-90 min.: 4,005±0,409) data between the groups, in terms of erythrocyte deformability (p > 0.05) (Fig. 1a and 1b).
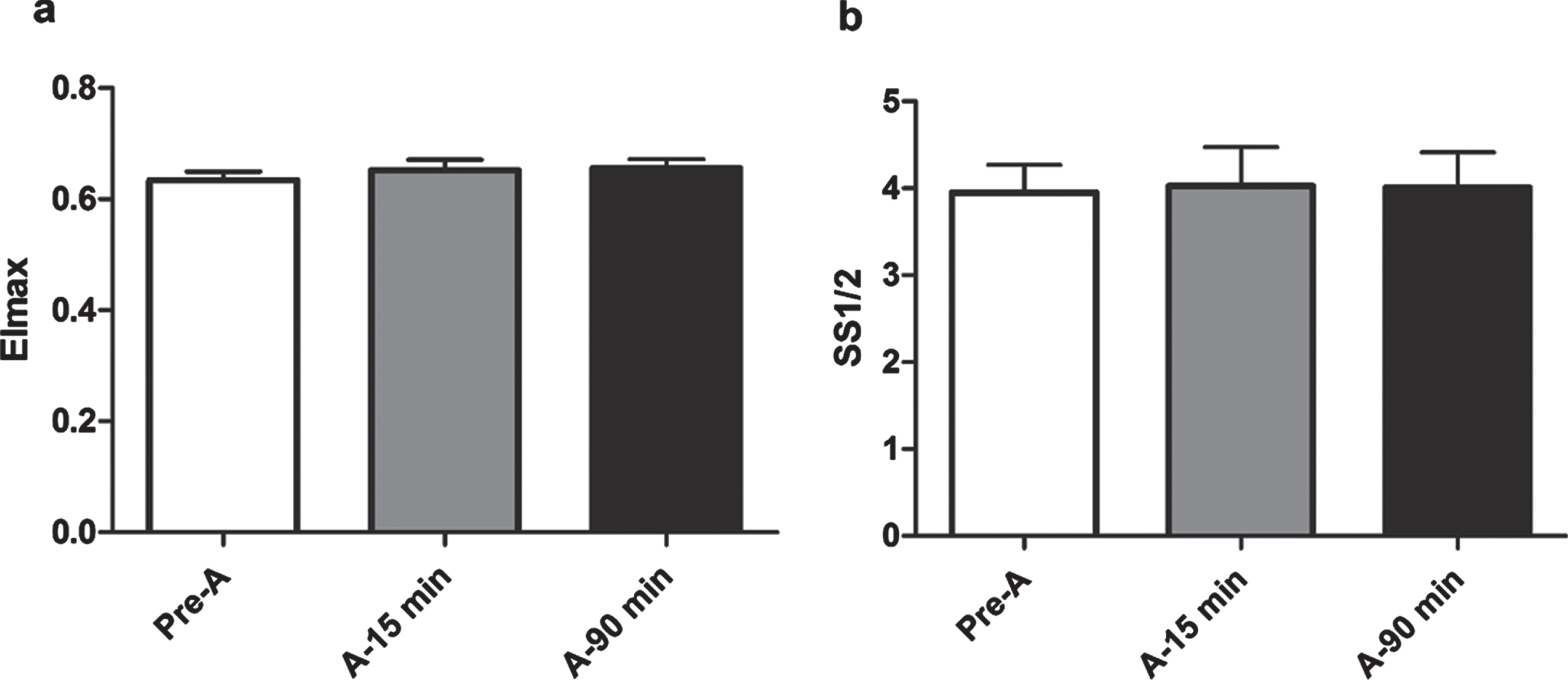
Erythrocyte deformability alterations after albumin replacement. a. EImax b. SS1/2.
AI of the groups did not change 15 minutes of albumin infusion (Pre-A: 56,280±3,390 vs. A-15 min.: 52,630±2,885) (p > 0.05). However, erythrocyte aggregation significantly decreased 90 minutes after albumin infusion compared with previous time points (Pre-A: 56,280±3,390 vs. A-90 min.: 42,550±4,096 p < 0,001 and A-15 min.: 52,630±2,885 vs. A-90 min.: 42,550±4,096 p < 0,01) (Fig. 2).

Aggregation index (AI) alterations after albumin replacement. ***p < 0.001 Pre-A vs A-90 min, ##p < 0.01 A-15 minvs A-90 min.
Whole blood viscosity decreased significantly after albumin infusion at 20 rpm (Pre-A: 7,287±1,132; A-15 min.: 2,916±2,225; A-90 min.: 2,787±0,222 p < 0.01) (Fig. 3a). At 50 rpm, whole blood viscosity decreased at 15 minutes of albumin infusion however the alteration became significant at 90 minutes statistically (Pre-A: 2,817±0,192; A-15 min.: 2,375±0,153 p > 0.05 and A-90 min.: 2,297±0,156 p < 0.05) (Fig. 3b).
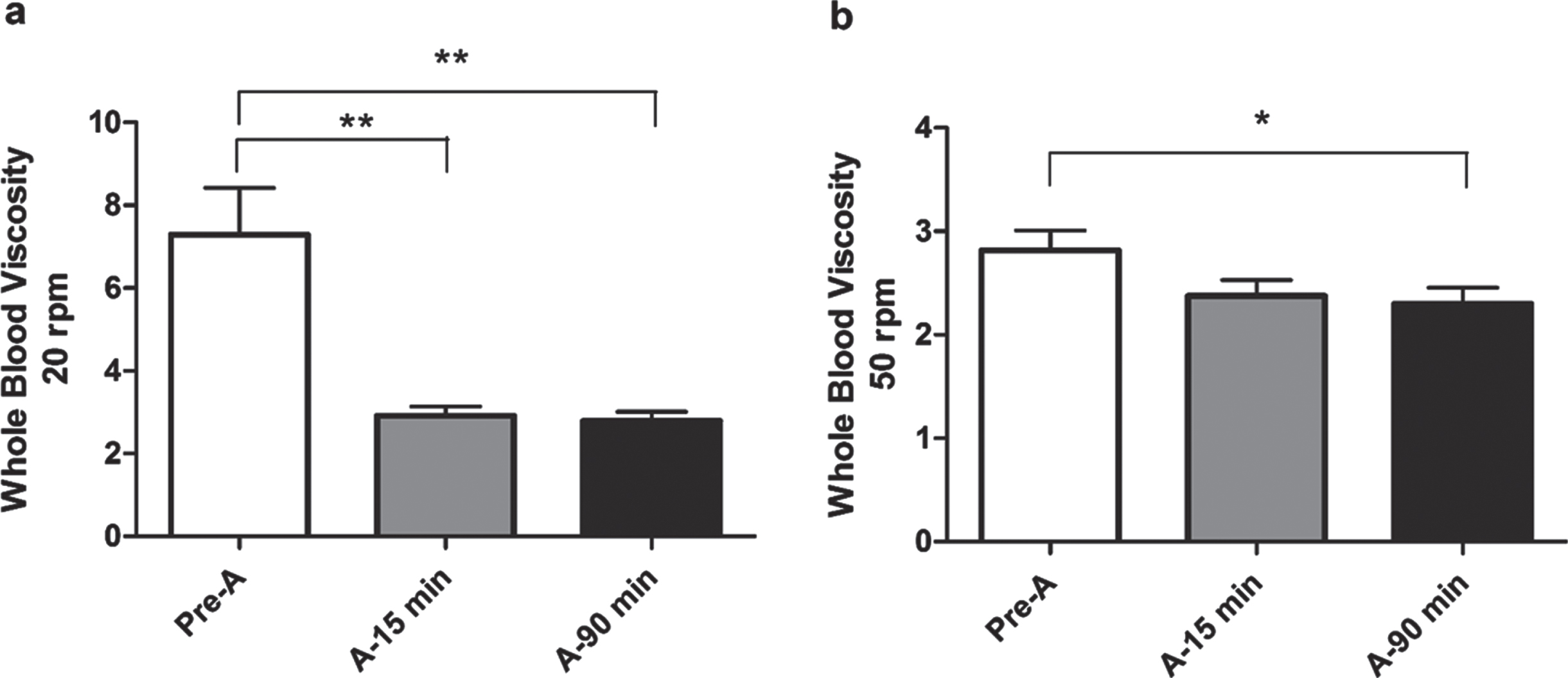
Whole blood viscosity alterations after albumin replacement a. 20 rpm b. 50 rpm. **p < 0.01 Pre-A vs A-15 min and A-90 min, *p < 0.05 Pre-A vs A-90 min.
Plasma viscosity also decreased significantly after albumin infusion at 20 rpm (Pre-A: 5,813±1,198; A-15 min.: 2,655±0,396; A-90 min.: 2,461±0,259 p < 0.05) (Fig. 4a). The reduction in plasma viscosity was insignificant in measurements at 50 rpm (Pre-A: 2,621±0,420; A-15 min.: 1,828±0,210; A-90 min.: 1,688±0,161 p > 0.05) (Fig. 4b).
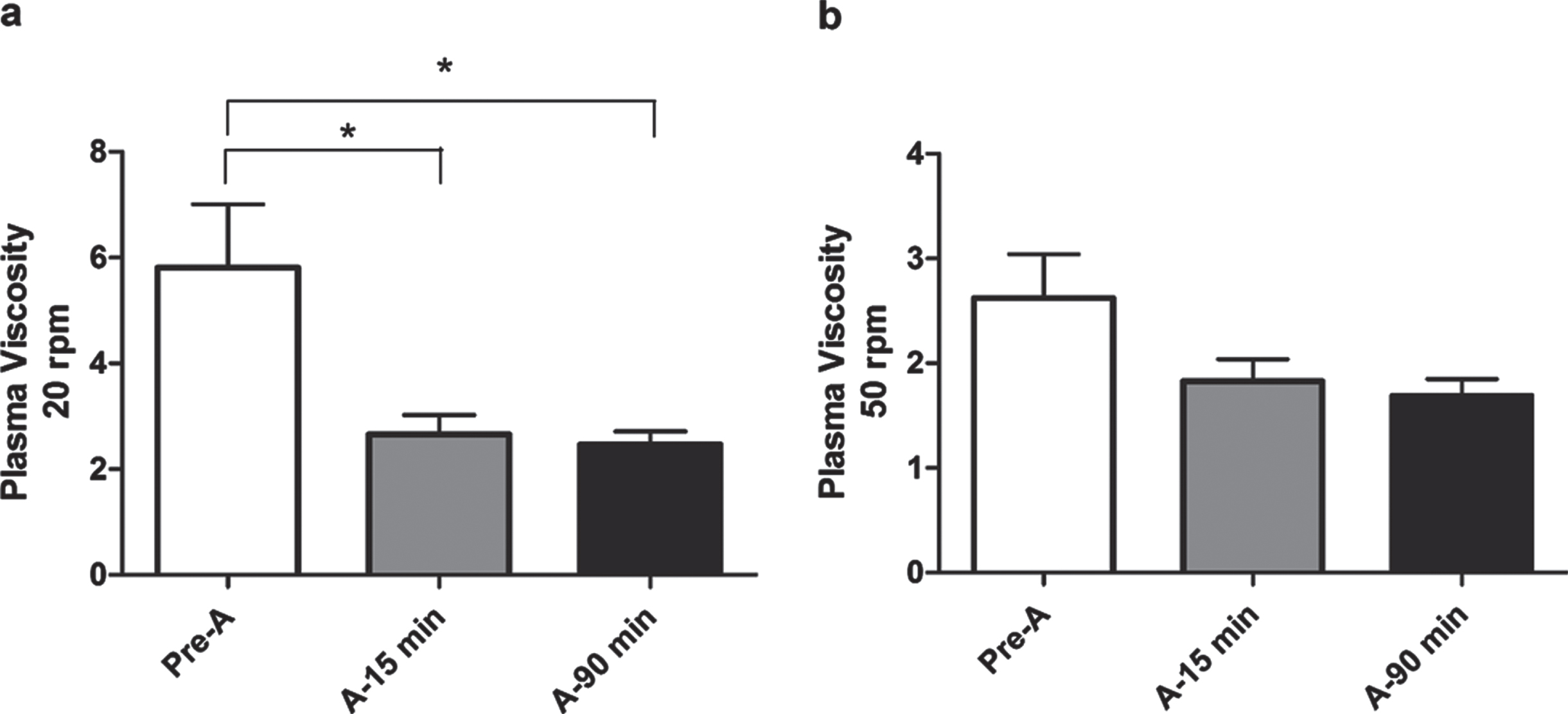
Plasma viscosity alterations after albumin replacement. a. 20 rpm b. 50 rpm. *p < 0.05 Pre-A vs A-15 minand A-90 min.
Although Hct values did not change among groups at 15 minutes of albumin infusion (Pre-A: 27,730±1,123 vs. A-15 min.: 26,590±1,187 p > 0.05), this parameter significantly decreased at 90 minutes of albumin infusion (Pre-A: 27,730±1,123 vs. A-90 min.: 25,230±1,153 p < 0,05) (Fig. 5).

Hematocrit alterations after albumin replacement. *p < 0.05 Pre-A vs A-90 min.
Tk also decreased significantly after albumin infusion at 20 rpm (Pre-A: 0,0121±0,0023 vs. A-15 min.: 0,0053±0,0017 p < 0.05; Pre-A: 0,0121±0,0023 vs. A-90 min.: 0,0045±0,0009 p < 0.01). However, Tk did not altered between 15 and 90 minutes of albumin infusion at 20 rpm (A-15 min.: 0,0053±0,0017 vs. A-90 min.: 0,0045±0,0009 p > 0.05). At 50 rpm, Tk decreased at 15 minutes of albumin infusion however the alteration became significant at 90 minutes statistically (Pre-A: 0,0076±0,0022; A-15 min.: 0,0058±0,0027 p > 0.05 and A-90 min.: 0,0056±0,0005 p < 0.05) (Fig. 6).
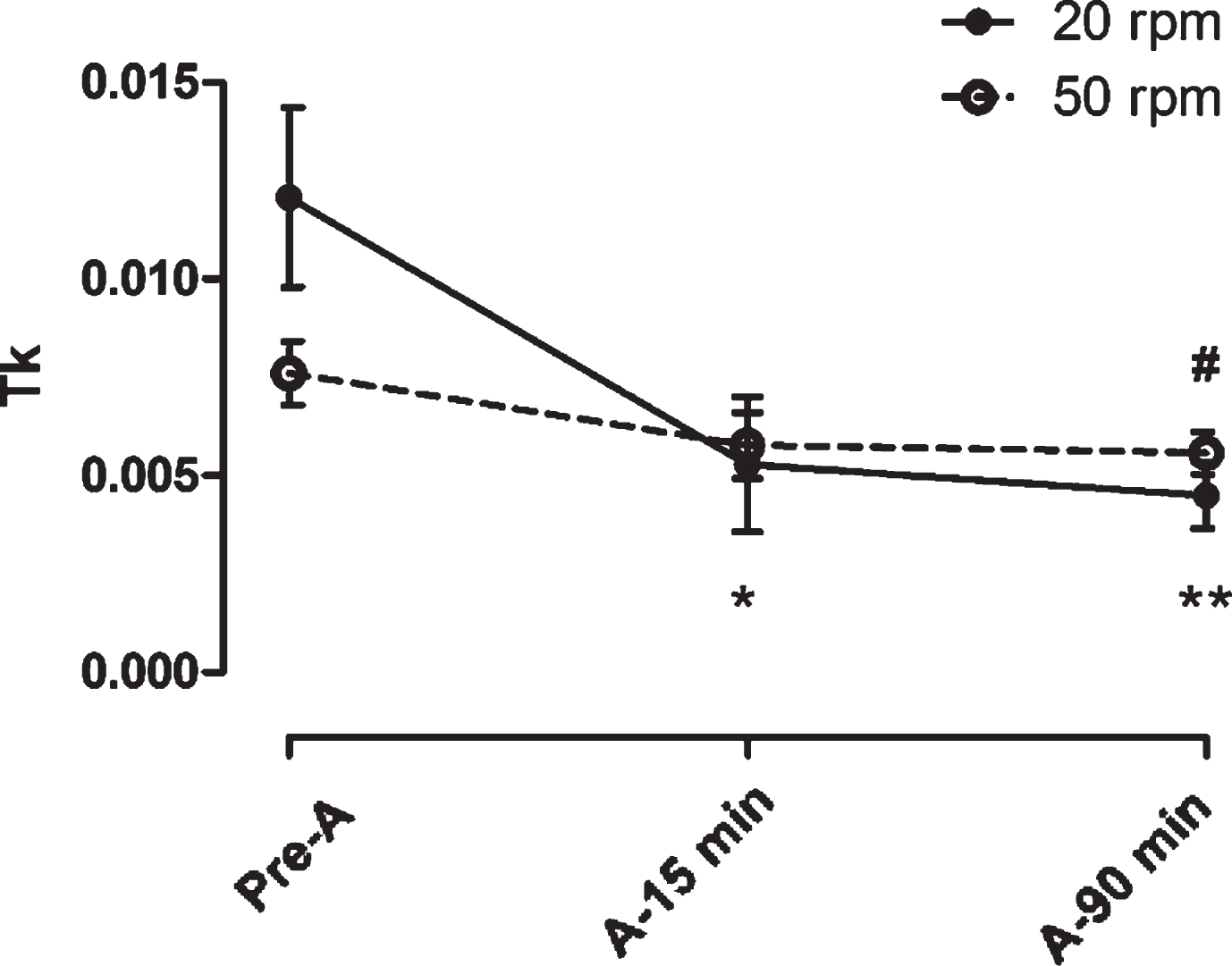
Erythrocyte rigidity coefficient (Tk) alterations at 20 rpm and 50 rpm after albumin replacement. *p < 0.05 Pre-A vs A-15 min, **p < 0.01 Pre-A vs A-90 min, #p < 0.05 Pre-A vs A-90 min.
Albumin infusion did not make a sense in systolic, diastolic and mean arterial blood pressure values of the patients (p > 0.05). Hemodynamic effects of albumin were re-evaluated by comparing the patients with systolic blood pressure values below or above 90 mmHg before infusion. Similar assessment was made in patients with mean arterial blood pressure below or above 70 mmHg. Albumin infusion significantly increased blood pressure values in the sub-group of patients with SBP below 90 mmHg and MAP below 70 mmHg (p < 0.05) (Table 2).
Hemodynamic parameters of patients
Footnotes: SBP: Systolic Blood Pressure, DBP: Diastolic Blood Pressure, MAP: Mean Arterial Pressure, Pre-A: Pre-albumin replacement, A: Post-albumin replacement. ap < 0.05 Pre-A vs A-15 min, bp < 0.05 Pre-A vs A-90 min. Datas are presented as mean±S.E.M.
In 9 patients who underwent advanced hemodynamic monitoring; CI, SVRI, ELWI and GEDI values were not affected from albumin infusion (p > 0.05). Data related with cardiac output was re-evaluated by separating the patients into two groups according to their CI values as below or above 3 L/min before infusion. Patients with CI values below 3 L/min revealed an increment in CI values after albumin infusion however the difference was not significant (Table 3).
Advanced hemodynamic monitoring parameters of patients
Footnotes: CI: Cardiac Index, SVRI: Systemic Vascular Resistance Index, ELWI: Extravascular Lung Water Index, GEDI: Global End-Diastolic Volume Index, Pre-A.: Pre-albumin replacement, A:Post-albumin replacement. Datas are presented as mean±S.E.M.
Blood fluidity is a fundamental function for graft perfusion and survival in liver transplant patients. Otherwise, liver acts as the major determinant of protein and coagulation factor synthesis and liver pathologies may lead to alterations of blood fluidity. Information related with hemorheological behaviors may provide better hemodynamic treatment strategies in the patients suffering from liver insufficiency and/or transplantation.
Albumin solutions are frequently used at perioperative period, for the purpose of replacement of albumin, modification of coagulation status [4, 7–9] or hemodynamic stabilization in liver transplant patients. The relationship between albumin and hemorheology was investigated in various studies and conflictive results were informed [5, 10–12]. The study of Nagase et al. was the first which revealed that red blood cell deformability is influenced by plasma albumin concentration in analbuminemic rats. Hypoalbuminemia was shown to cause a decrease in red blood cell deformability and an increase in blood viscosity by altering red blood cell membrane phospholipid layer composition [10]. Washing stored red blood cells in an albumin solution was reported to improve microvascular perfusion and morphologic properties of red blood cells. However red blood cell deformability decrease related with blood storage was not influenced by albumin interaction [6]. The possibility of a relationship between plasma albumin concentration and red blood cell aggregation was suggested at first time by the observation of concomitant increase in plasma fibrinogen/albumin ratio and red blood cell aggregation [14]. Decline in plasma albumin concentration in patients with chronic renal failure was associated with increase in red blood cell aggregation and whole blood viscosity [15].
In this prospective study, perioperative acute effects of albumin infusion in liver transplant patients on hemorheology, hemodynamics and coagulation were investigated. It was the only study protocol which investigated the course of hemorheological properties and their alteration with albumin infusion in liver transplant patients. For addressing the acute effects of albumin infusion, blood samples were withdrawn just before and 15 and 90 minutes after delivery.
Albumin was suggested to correct morphological changes or deformability properties of red blood cells previously. Wong et al. informed the reversal of erythrocyte echinocytosis by incubation and storage by serum albumin [16]. Likewise, Reinhard et al. showed that washing stored red blood cells in an albumin solution improved their morphologic and hemorheological properties. The authors have suggested that washing with % 1 human serum albumin may represent a new approach to improving the quality of stored red blood cells and thus potentially reducing the likelihood of adverse clinical outcomes associated with transfusion of blood stored for longer periods of time [8]. Another study investigating the effects of human serum albumin on red blood cell deformability was performed with stored or dehydrated red blood cells in vitro. Authors suggested that human serum albumin can increase red blood cell deformability by improving Band-3 protein ion exchange on cell membrane. Afore mentioned studies were designed to investigate the efficacy of human serum albumin on correcting the red blood cells morphological or hemorheological alterations caused by blood storage or dehydration. However, red blood cell deformability was in accordance with the values of healthy controls at our liver transplant patients both before and after human albumin infusion (data not shown). Calculations of EImax and SS1/2 was not altered following albumin infusion at any time point. The main reason for not detecting any improvement in terms of deformability may result from intact morphological properties and deformability of red blood cells prior to human albumin infusion in our study group.
Previous studies reveal great discrepancy at the role of human albumin solution on red blood cell aggregation [17–22]. Diversity of results may result from different techniques used in order to measure aggregation and not considering the interaction of various plasma proteins. Considering albumin adsorbs to the RBC surface but not produces bridges between individual RBC, theoretically albumin should decrease RBC aggregation. Early results demonstrated albumin inhibits RBC sedimentation and aggregation [18, 20]. However, opposite interaction considering a negative correlation between plasma albumin concentration and RBC aggregation has also been shown under various conditions [17, 23]. Aggregation stimulating factors may also change the effect of albumin on RBC aggregation [19]. While albumin has shown to inhibit lgG induced aggregation, it cause increment in fibrinogen induced aggregation. However, in suspensions containing high concentrations of fibrinogen and lgG, albumin has shown to increase RBC aggregation [17]. Authors suggested that albumin acts as an important trigger of red blood cell aggregation in the setting of high fibrinogen and immunoglobulin concentrations. According to available data, existence of a red blood cell aggregation model depending on plasma proteins was announced and interactions between red blood cells and proteins were highlighted to bring out disguised mechanisms. There are two potential mechanisms which may clarify the plasma protein-aggregation connection. The first one is the ‘Fibrinogen Theory’ which is constructed on the hypothesis that fibrinogen molecules attach red blood cells, form bridges between cells and aggravate aggregates. The second theory assumes an influence of surface charge change on red blood cells caused by fibrinogen resulting with altered aggregation behavior. From this point of view, concentrations of albumin and other plasma proteins may have different influences on red blood cell aggregation depending on present plasma fibrinogen status. There was no difference of mean aggregation index between the measurements performed from the bloods withdrawn before and 15 minutes after human albumin infusion in our study group. However, aggregation index significantly decreased 90 minutes after human albumin infusion compared with the values measured before and 15 minutes after albumin administration. Our patients had mean fibrinogen levels of 226±16,3 mg/dL (ref; 180–350 mg/dL) and mean albumin concentrations of 3,19±0,12 g/dL (ref; 3.4–4.8 mg/dL), preoperatively. Very close concentrations of fibrinogen and albumin compared to reference values may lead to aggregation index measurement similar to healthy individuals in our study (data not shown). Besides this, in the environment of stable fibrinogen concentrations as we designed at our study protocol, tendency of decrease in red blood cell aggregation 15 minutes after human albumin infusion and a statistically significant decrease after 90 minutes lead to an assumption that albumin suppresses the aggregation of circulating red blood cells. Hct decrease is in parallel with the reduction in RBC aggregation. Hence, RBC aggregation may be affected by the concurrent Hct decrement at 90 minutes of albumin infusion. The relation between Hct and RBC aggregation has been well studied on human blood samples and shown to change in various animal species [24–29]. Reduction of red blood cell aggregation in liver transplanted patients may have a critical role in decreasing viscosity, reducing resistance to blood flow and improving graft perfusion. For the reason, perioperative maintenance of adequate albumin concentrations may be essential for graft survival in these patients.
Whole blood viscosity was evaluated both at 20 and 50 rpm. Mean blood viscosity significantly decreased at 15 and 90 minutes after human albumin administration however there was not any difference between the viscosity values obtained at these time points of 20 rpm measurements. Declining trend due to time in blood viscosity after human albumin infusion was also obvious at 50 rpm measurements and the difference was statistically significant after 90 minutes. Joles et al. described analbuminemia as a hyperviscous state in rats and informed that both whole blood and plasma viscosity were increased at every cutting speed [9]. Authors pointed out the increased risk of coronary atherosclerosis and thrombosis in the hypoalbuminemic patients with nephrotic syndrome and emphasized the importance of plasma albumin on whole blood and plasma viscosity. Even though plasma albumin concentration was within normal ranges in most of the patients included in our study, human albumin administration still revealed a blood viscosity lowering effect. This finding was not described at any study before and may provide new frontiers in terms of hemorheological therapies at liver transplant patients. Whole blood viscosity decrease rather than increase despite addition of human albumin to the circulation may be the result of a reduction in red blood cell aggregation and fluid shift between the interstitial and intravascular compartments triggered by the oncotic effect of human albumin molecules. Decreased hematocrit levels due to increased circulating plasma volume may lead to viscosity alteration.
Plasma viscosity was also evaluated both at 20 and 50 rpm cutting speeds in order to exclude the viscosity altering effects of corpuscular members of blood (ie. red blood cell aggregation) and concretize the effects of albumin and other plasma proteins in the current study. Mean plasma viscosity decreased 15 and 90 minutes after human albumin infusion at both cutting speeds and the difference from initial measurement result was statistically significant at 20 rpm in parallel with whole blood viscosity analysis. This finding supports the hypothesis that the alteration in blood viscosity was not only raised from decrease in red blood cell aggregation but also from oncotic effects of human albumin administered simultaneously.
Plasma fibrinogen concentrations of the patients were very close to reference values and did not alter after human albumin infusion during the study. This finding was also very important for associating the hemorheological results with human albumin other than fibrinogen. For the reason that fibrinogen is a major plasma protein and its plasma concentration may have influence on hemodynamic homeostasis and mechanisms that are simultaneously affected by hemorheology, various plasma fibrinogen concentrations of the subjects would lead to conflicts in addressing the hemorheological effects of human albumin [14].
Hemoglobin and Hct values detected by blood gases analyzer decreased significantly 90 minutes after albumin infusion. Fluid shift related to increased plasma oncotic pressure may be the reason for intravascular fluid expansion and relative anemia. Hasselgren et al. created a diagram revealing the intravascular volume expansion effect of 20% albumin infusion by time [30]. Volume expansion reached a peak level after 60 minutes and attenuated within hours. This finding may explain the hemoglobin and Hct decrease evaluated after albumin infusion.
Hemodynamic alterations related to human albumin administration were also investigated in our study and no change in terms of blood pressure parameters was detected. However, at the subgroup analysis which were performed at the patients with systolic and mean arterial blood pressures higher or lesser than 90 mmHg and 70 mmHg respectively, blood pressure measurements revealed increment after human albumin infusion at the patients with systolic arterial blood pressure below 90 mmHg and mean arterial blood pressure below 70 mmHg. Likewise, CI measurements revealed an increase trend at the patients whose CI values were below 3 L/min. The aim of these subgroup analyses was to investigate the effects of human albumin on hemodynamic restoration in hypovolemic and hypotensive patients. The results of this investigation suggest that human albumin therapy may be helpful to maintain hemodynamic stability in hypotensive liver transplant patients. In accordance with our study, Song et al. reported a significant improvement in mean arterial blood pressure after human serum albumin administration in a rat hemorrhagic shock model [31]. In a study of Shasthry et al. searching whether albumin infusion causes volume overload in cirrhotics, ninety nine consecutive cirrhotic patients receiving 1gm per kg albumin infusion were evaluated for development of volume overload. The authors concluded that cardiac output (CO) increased after albumin infusion and baseline diastolic dysfunction had little effect on the development of volume overload or changes in CO.
Our study has some limitations. Firstly, intraoperative albumin infusion amount was not standardized because of the patients actual needs varied with hemodynamic variables. For the reason, the measurements derived from the first albumin infusion were included into the analysis. Second limitation was the potential effects of fluid, blood products and vasoactive drugs on hemorheology which were administered intraoperatively. Third limitation was the shortage of PICCO monitorization in some patients. Fourthly, plasma viscosity should be assessed at high shear rate and shear-related decrease often measured in rotational devices as Wells-Brookfield which we used in our study is not considered to have a biological relevance. Finally, graft source was not the same at every subject (10 brain dead, 7 living donors) which may have unpredicted effects on hemorheological status.
In conclusion; present study revealed that perioperative human albumin replacement did not cause significant alteration at red blood cell deformability but led to decrease in red blood cell aggregation, whole blood and plasma viscosities in liver transplant patients. Such a decline at both red blood cell aggregation and blood viscosity may offer more favorable hemorheological setting in terms of improving graft perfusion. Moreover, human albumin replacement induced blood pressure and CI elevation in hypotensive liver recipient. The results of this clinical study may contribute new aspects to hemodynamic and hemorheological effects of human albumin replacement for improving microcirculation and graft survival during liver transplantation.
Conflict of interest
No conflicts of interest, financial or otherwise, are declared by the author(s).
Funding
This study was supported by the Akdeniz University Research Projects Unit (Project no. TTU-2019-4920).