
Abstract
BACKGROUND:
Registration of three-dimensional contrast-enhanced ultrasound fusion imaging (3DCEUS-FI) is time-consuming to obtain high success rate.
OBJECTIVE:
To investigate the influence factors on registration success rate of 3DCEUS-FI.
METHODS:
Water tank phantoms were made to obtain mimicked pre- and post- radiofrequency ablation three-dimensional contrast-enhanced ultrasound (3DCEUS) and CT images. Orthogonal trials were designed according to factors including size, depth, enhancement level of mimicked tumor, diameter and number of mimicked adjacent vessels. Mimicked pre- and post-RFA 3DCEUS images of 72 trials were fused to assess ablative margin (AM) by two radiologists. With CT images as standard, 3DCEUS-FI accuracy was considered as the consistency of AM evaluation. The inter-observer agreement and the influence factors on registration success rates were analyzed.
RESULTS:
The intraclass correlation coefficient (ICC) for the consistency of AM evaluation between CT and 3DCEUS-FI in x-axis, y-axis or z-axis was 0.840∼0.948 (P < 0.001). The ICC for inter-observer agreement was 0.840∼0.948 (P < 0.001). The success rates of registration within mimicked vessels with diameter of 2 mm were significantly lower than those with diameter of 3 mm and 4 mm.
CONCLUSIONS:
The mimicked AM measured by 3DCEUS-FI had high accuracy and inter-observer agreement. Diameter of the mimicked adjacent vessels was significantly related to success rate of registration.
Abbreviations
Ablative margin
Automatic registration
Interactive registration
Local tumor progression
Radiofrequency ablation
Three-dimensional contrast-enhanced ultrasound fusion imaging
Three-dimensional contrast-enhanced ultrasound
Introduction
Hepatocellular carcinoma (HCC) is the sixth most prevalent cancer and the third most frequent cause of cancer-related death [1]. Image-guided ablation has been currently considered the best option for patients with Barcelona Clinic Liver Cancer (BCLC) stage A who are not candidates for surgical resection [2]. However, local tumor progression (LTP) remains a problem owing to its high rate varying from 4.2% to 21.7% within five years [3–5]. Previous studies have demonstrated that insufficient ablative margin (AM) was an independent predictor of LTP after ablation. It had been reported that AM < 5 mm resulted in cumulative LTP rate of 28% ∼66% [6–9]. Therefore, it is critical to evaluate whether AM is sufficient accurately and quickly after ablation therapy. As a critical parameter of local ablation efficacy, accurate AM assessment could provide valuable feedback to the operator.
The emergence of image fusion enables AM evaluation. Image fusion refers to postprocessing technique used to merge cross-sectional images of same or different modalities of the same scene into a single composite image which integrates the useful information of those images [10, 11]. Image registration is the basis of image fusion, which refers to the process of aligning two or more images of the same scene taken at different times through specific algorithms [12, 13]. In recent years, mono-modality fusion imaging methods including CT-CT or MRI-MRI image fusion have been explored to assess AM after ablation and been universally acknowledged feasible ways that can evaluate AM accurately. However, it is not easy to access CT/MRI Digital Imaging and Communications in Medicine (DICOM) data in ultrasound-guided ablation procedure and perform CT-CT or MRI-MRI fusion immediately after ablation for hepatic tumors [14–16].
Nowadays, contrast-enhanced ultrasound (CEUS) has been widely used in evaluating treatment response of thermal ablation for hepatic tumors and many other tumors [17–20]. In recent years, some studies reported that three-dimensional contrast-enhanced ultrasound (3DCEUS) could not only evaluate treatment response of ablation for liver tumors but also provide intuitive spatial structure and perfusion information characteristics of the tumor and ablation zone [21, 22]. Our team has developed a novel mono-modality fusion technique of three-dimensional contrast-enhanced ultrasound fusion (3DCEUS-FI) imaging that could fuse the 3DCEUS images before and immediately after ablation. It proved to provide a way to evaluate AM accurately [23]. Through interactive registration (IR) instead of automatic registration (AR), the success rate of registration can be improved from 57.1% to 91.7% in clinical settings in our previous report [23]. Despite the high success rate, IR is really more time-consuming and inconvenient than AR. Therefore, in this study, we design orthogonal experiments to systematically investigate the influence factors on registration success rate of 3DCEUS-FI through a phantom study.
Methods
Water tank phantom fabrication
Water tank phantoms were fabricated using the plastic tank as a container, and sound absorbing sponges with a thickness of about 2 cm were fixed on the inner wall of the tank. The core part of the phantom was fabricated with a 14F double channel catheter and a balloon with good acoustic transmissibility. The balloon was fixed outside the urethra sacculus of the double channel catheter (Foley, Bard, USA). The core part was fixed in the center of the tank. According to minimum mimicked AM, the models were divided into two types: AM < 5 mm and AM≥5 mm. The vessels adjacent to the mimicked tumor were mimicked with hollow, thin-walled and transparent silicone tubes. The wall thickness of the tubes was 2 mm. The inner diameters of the tube were of three types: 2 mm, 3 mm and 4 mm, respectively. The mimicked vessels were distributed around the balloon and were not parallel to each other.
Contrast-enhanced agent was injected into the urethra sacculus to mimic tumors, and water was injected into the balloon to mimic ablation zone, and the space between urethra sacculus and balloon was used to mimic AM. Each part of the phantom was injected with fluid according to the concentration of SonoVue in Table S1 and the volume in Table S2. The water tank was filled with well-mixed 0.0016% SonoVue so as to mimic the liver parenchyma. The pre-ablation situation with hyper-enhanced tumor was mimicked by injecting 0.2% SonoVue into the urethra sacculus, while pre-ablation situation with hypo-enhanced tumor was mimicked by injecting 0.0008% SonoVue. The vessels were mimicked by injecting 0.2% SonoVue into the silicone tubes. The balloon was injected with 0.0016% SonoVue. Therefore, the mimicked tumor showed hyper- or hypo-enhancement compared with mimicked liver parenchyma, and the mimicked vessels were hyper-enhanced in mimicked pre-ablation 3DCEUS images. The post-ablation situation with non-enhanced ablation zone was mimicked by injecting water into the balloon and urethra sacculus. The vessels were mimicked by injecting 0.2% SonoVue into the silicone tubes and showed hyper-enhancement. Therefore, the mimicked ablation zone showed non-enhancement and the mimicked vessels were hyper-enhanced in mimicked post-ablation 3DCEUS images.
Orthogonal experiments design
In order to explore if the factors in Table 1 influence the registration success rate of 3DCEUS-FI, we design several orthogonal experiments. For both mimicked AM < 5 mm and AM≥5 mm phantoms, L36 (33×22) orthogonal table (Table S3) was designed. Therefore, a total of 72 trials were arranged in this study.
Research factors on registration success rate of three-dimensional contrast-enhanced ultrasound fusion imaging
Research factors on registration success rate of three-dimensional contrast-enhanced ultrasound fusion imaging
3DCEUS images were acquired with a Mindray DC8 ultrasound scanner (Mindray, Shenzhen) equipped with a 3D imaging probe (D6-2E, with a frequency range of 3.5∼5.0 MHz). The probe was stably fixed by the iron stand, and the coronal plane of the probe was parallel to the coronal plane of the tank. All 3DCEUS examinations were performed by a sonographer who had five years’ experience performing 3DCEUS. Before 3DCEUS examination, baseline ultrasound was performed to identify the mimicked tumor and the imaging parameters were optimized to achieve high-quality images. Then 2DCEUS was initiated and diluted SonoVue (Bracco, Milan, Italy) was injected into each part of the phantom and 3DCEUS was initiated. The imaging settings for 3DCEUS were as follows: mechanical index, 0.08–0.10; one focal zone; power output, 3–6%; dynamic range, 40-60 dB; volume angle, 60°. Both the pre- and post-ablation mimicking 3DCEUS volume data were stored within the US machine.
CT acquisitions
CT examinations were performed after 3DCEUS examinations. Scans of the phantoms were performed using an AquilionTM 64-slice helical CT machine (Canon, Tochigi, Japan) with the following parameters: 0.5 mm×64 mm collimation, 120 kV and 150∼200 mA. The phantom was placed horizontally on the CT examination bed and then the coronal plane and sagittal plane were calibrated. Flow chart of the study were shown were shown in Fig. 1.
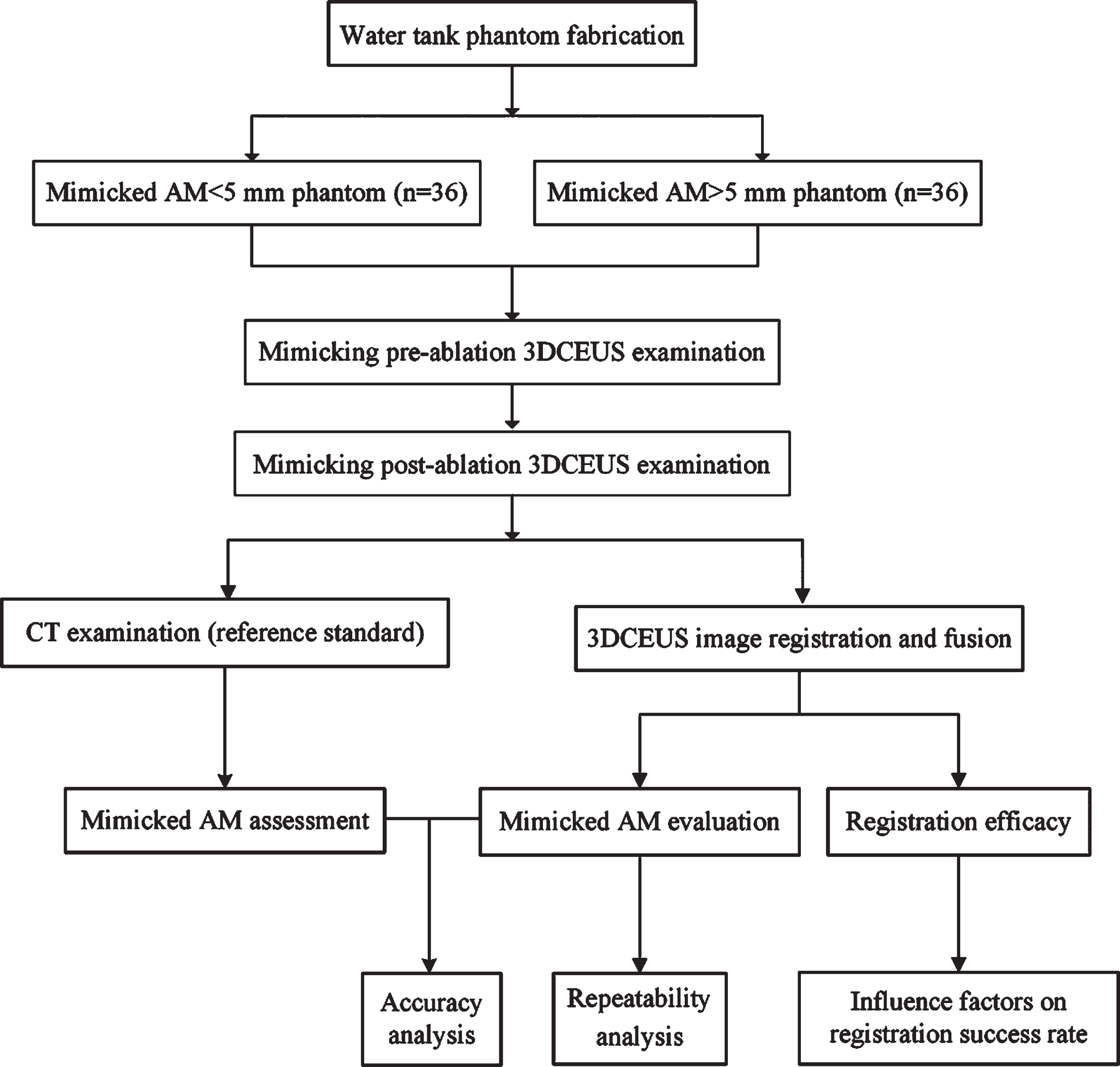
Flow chart of the experiment. AM, ablative margin; 3DCEUS, three-dimensional contrast-enhanced ultrasound.
A fusion software equipped in an ultrasound workstation (Mindray, Shenzhen) was used to evaluate mimicked AM. 3DCEUS-FI process was performed and interpreted by two radiologists (A and B, those with five years’ experience performing 3DCEUS) independently. The registration requires the interpreters to delineate corresponding vessels on pre- and post-ablation mimicking 3DCEUS images as landmarks, and then the software accomplishes registration. After registration, registration error (RE) assessment by the radiologists is needed. An arbitrary landmark adjacent to the mimicked tumor was marked on the mimicked pre-ablation and post-ablation 3DCEUS images and RE was measured on the fusion images. The RE was defined as the extent to which the same landmark was accordant between mimicked pre- and post-operation 3DCEUS images (Fig. 2). Registration was considered successful if the RE was no more than 3 mm. However, registration process was considered failed if a successful registration could not be achieved after three attempts. The success rate of registration of both radiologists was recorded respectively.
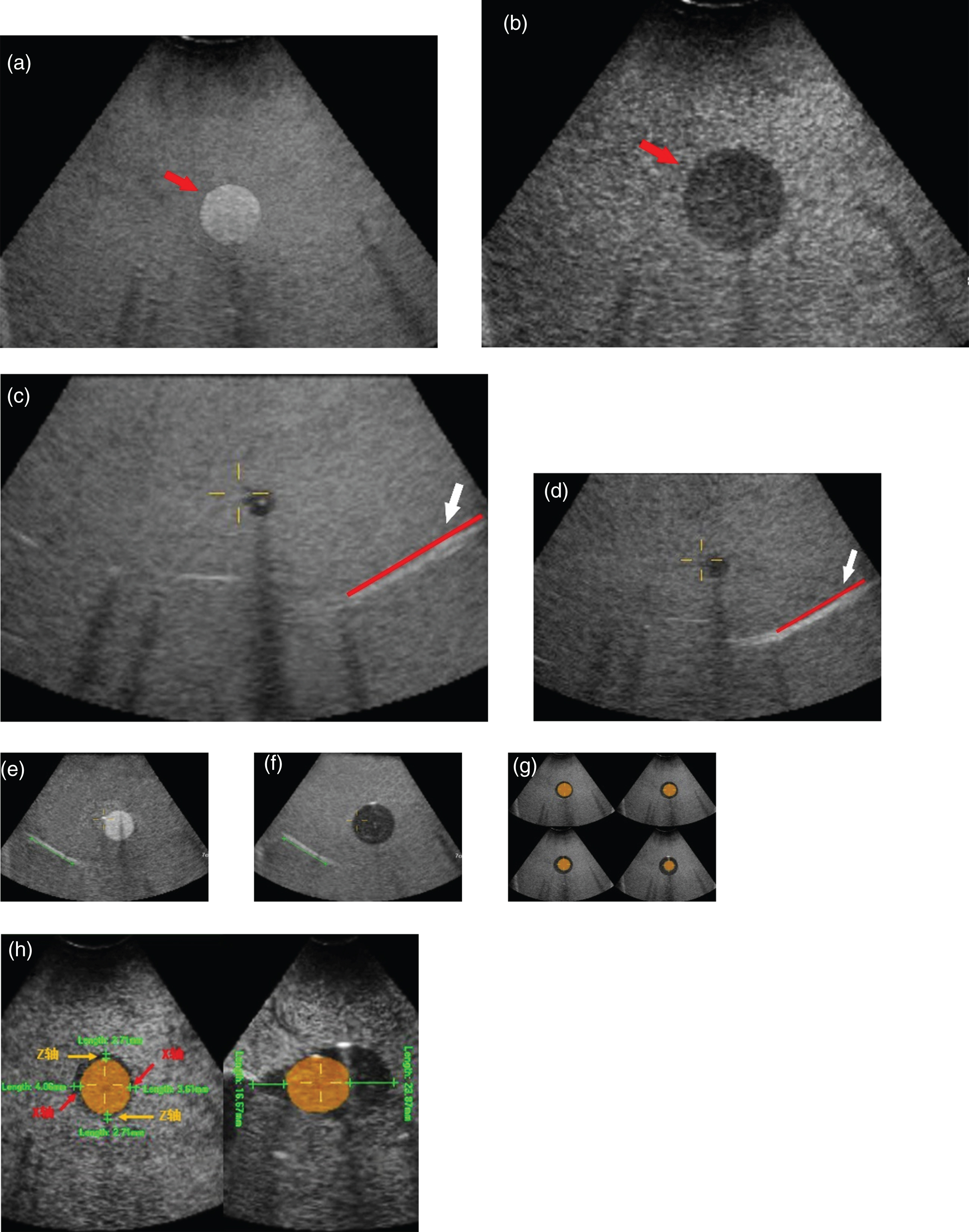
Interactive registration and measurement of mimicked ablative margin. (a) The mimicked tumor shows hyper-enhancement (red arrow) in the A-plane on the mimicked pre-operative 3DCEUS image, as ultrasound contrast agent was injected in the urethra sacculus. (b) The mimicked ablation zone shows non-enhancement (red arrow) in the A-plane on the mimicked post-operative 3DCEUS image, as ultrasound contrast agent was injected in the balloon. (c) The external wall of the mimicked vessel (red line, white arrow) was identified and marked on the mimicked pre-operative (c) and post-operative (d) 3DCEUS images, and then two images were registered by the software. (e) After registration, the external wall of a mimicked vessel (green line) is marked on the mimicked pre-operative image. (f) The marker (green line) delineated on (e) is automatically be mapped to the mimicked post-operative image. The registration error is the distance between the mapped virtual and real position of the external wall of the mimicked vessel and the real position. Therefore, the registration error is 0. (g) After successful registration, the mimicked tumor was segmented on the mimicked pre-operative image. Its contour information (orange) was automatically mapped to the mimicked ablation zone on the mimicked post-operative image. The relationship between the mimicked tumor and the ablation zone was observed in the multiplanar reconstruction mode (2 x 2). (h) On the A-plane, the mimicked ablative margins (left, green line) in the 3, 6, 9 and 12 o’clock directions of the maximum slice of mimicked tumor were measured. On the B-plane, the mimicked ablative margins (right, green line) in the 3 and 9 o’clock directions the maximum slice of the mimicked tumor were measured.
After successful registration, the mimicked tumor was needed to be segmented by the radiologists. Images of the mimicked tumor, which were marked in yellow to enhance the contrast between the mimicked-tumor and mimicked ablation zone, were overlapped on the mimicked ablation zone in a multiplanar reconstruction (MPR) mode. As a result, the mimicked tumor and ablation zone were fused on the same image. Therefore, the AM on Plane A, B and C could be measured by the radiologists easily and directly. AMs on the X-axis, Y-axis and Z-axis passing through the center of the mimicked tumor were required to be measured on the fused images. In other words, the six directions were at the 3, 6, 9, 12 o’clock directions on the maximum A-plane and at the 3, 9 o’clock directions on the maximum B-plane of the mimicked tumor.
The CT images analysis were performed by two radiologists with five years of experience with CT and blinded to results of 3DCEUS-FI, and consensus was obtained by discussion. The RadiAnt DICOM Viewer (Medixant, Poznan, Poland) software was used to analyze CT images and evaluate mimicked AM. The AM at the above six corresponding directions were required to be measured on the CT images (Fig. 3).
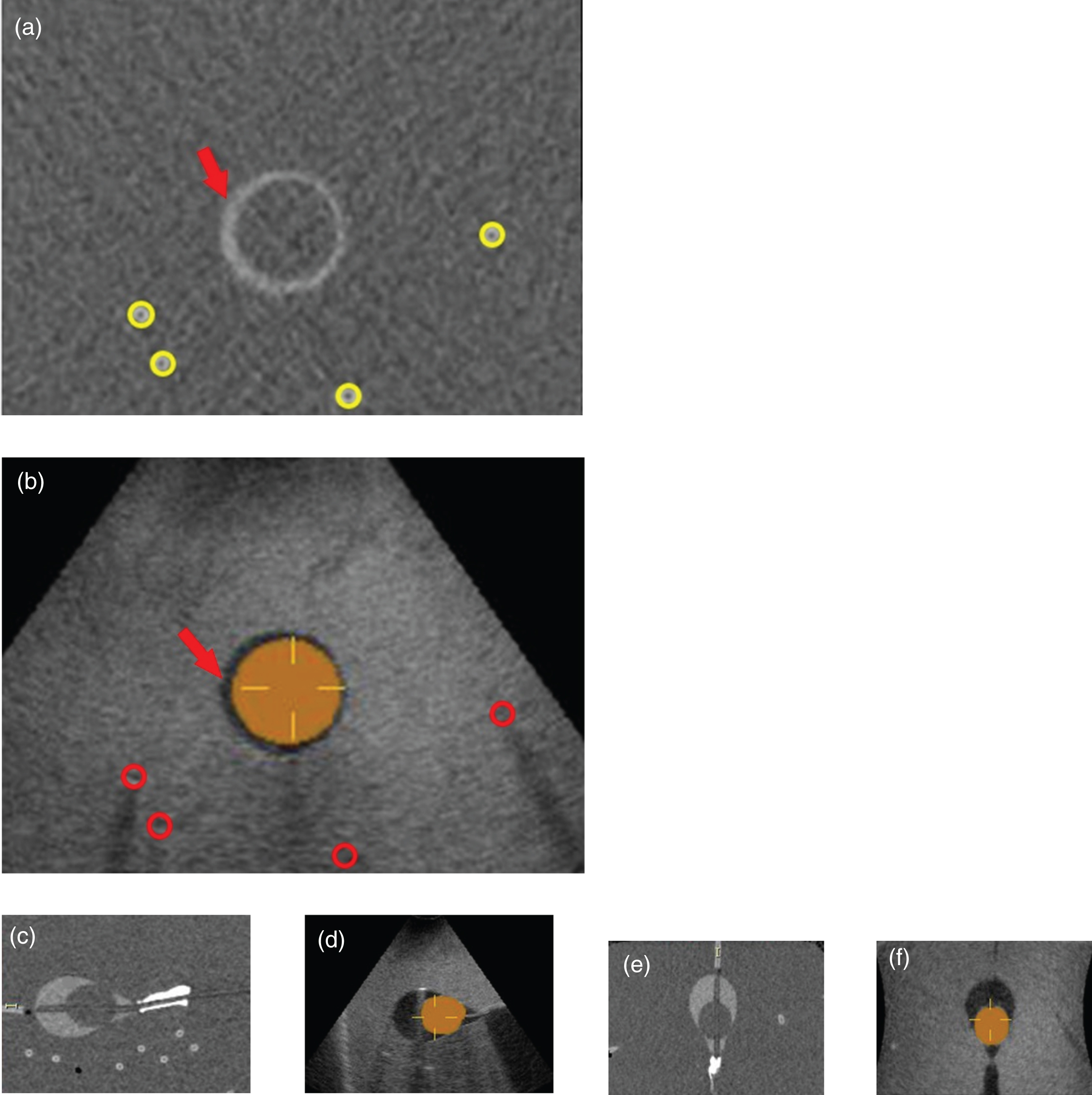
Evaluation of mimicked ablative margin by CT and 3DCEUS-FI. (a) It shows the mimicked ablative margin (red arrow) in the maximum slice of the mimicked tumor on the A-plane on CT image, and the mimicked vessels are marked in yellow circles. (b) It shows the mimicked ablative margin (red arrow) in the maximum slice of the mimicked tumor on the A-plane on 3DCEUS-FI image, and the mimicked vessels are marked in red circles. Similarly, (c) and (d) show the mimicked ablative margin in the maximum slice of the mimicked tumor on the B-plane on CT and 3DCEUS-FI image, respectively. (e) and (f) show the mimicked ablative margin in the maximum slice of the mimicked tumor on the C-plane on CT and 3DCEUS-FI image, respectively. 3DCEUS-FI, three-dimensional contrast-enhanced ultrasound fusion imaging.
Quantitative data were expressed as means±standard deviations. Differences in quantitative variables were detected with an independent sample t-test or Mann–Whitney U-test. The data analyses were performed using SPSS software (version 16.0, SPSS Inc., Chicago, IL). The consistency of AM evaluation between CT and 3DCEUS-FI was expressed in intraclass correlation coefficient (ICC) [24, 25]. The inter-observer agreement of 3DCEUS-FI was expressed in ICC-AB, which was tested with two-way random-effects model and the absolute agreement of single measures. ICC < 0.5 is considered with poor consistency. 0.5≤ICC<0.75 is considered with moderate consistency. 0.75≤ICC<0.90 is considered with high consistency. ICC≥0.90 is considered with excellent consistency. Firth’s penalized likelihood logistic regression analysis [26, 27] was used to explore the influence factors on the success rate of 3DCEUS-FI registration, which was conducted with logistf package and R software (version 3.4.0; http://www.r-project.org/). All data with P values less than 0.05 were considered statistically significant.
Results
The success rate of registration was both 81.9% (59/72) for Radiologist A and B. The duration time of registration was 5.8±2.6 min (range, 3.1∼12.3 min) for Radiologist A and 6.1±2.6 min (range, 3.3∼12.5 min) for Radiologist B.
Accuracy of 3DCEUS-FI to evaluate mimicked AM
The consistency of mimicked AM evaluation between CT and 3DCEUS-FI was high at the 3, 6, 9, 12 o’clock directions on the maximum A-plane and at the 3, 9 o’clock directions on the maximum B-plane of the mimicked tumor (Table 2). The range of ICC was 0.851∼0.961 (P < 0.001) (Table 2).
Consistency of mimicked ablative margin evaluation between 3DCEUS-FI and CT (n = 59)
Consistency of mimicked ablative margin evaluation between 3DCEUS-FI and CT (n = 59)
The consistency of mimicked AM evaluation between Radiologist A and B was high at the 3, 6, 9, 12 o’clock directions on the maximum A-plane and at the 3, 9 o’clock directions on the maximum B-plane of the mimicked tumor. The range of ICC-AB is 0.840∼0.948 (P < 0.001) (Table 3).
Variability of mimicked ablative margin evaluation by 3DCEUS-FI (n = 59)
Variability of mimicked ablative margin evaluation by 3DCEUS-FI (n = 59)
3DCEUS-FI, three-dimensional contrast-enhanced ultrasound fusion imaging; AM, ablative margin; ICC, intraclass correlation coefficient; ICC-AB, intraclass correlation coefficient of radiologist A and B; ICC-A, intraclass correlation coefficient of two measurements of radiologist A; CI, confidence interval.
Diameter of mimicked vessels was an independent factor of success rate of registration (Table 4). The success rate of registration decreases significantly when diameter of mimicked vessels is 2 mm. There were no significant correlations between mimicked tumor diameter, mimicked tumor depth, enhancement level of mimicked tumor, and number of mimicked vessels and the success rate of 3DCEUS-FI registration (Table 4).
Influencing factors on interactive registration success rate of 3DCEUS-FI (n= 72)
Influencing factors on interactive registration success rate of 3DCEUS-FI (n= 72)
*95% confidence interval was expressed in the parentheses. 3DCEUS-FI, three-dimensional contrast-enhanced ultrasound fusion imaging; AM, ablative margin; OR, odds ratio.
In this study, 3DCEUS-FI technique, a novel mono-modality fusion technique that could fuse the 3DCEUS images developed by our team, was feasible to evaluate mimicked AM in vitro phantom study. Water tank phantoms were designed and used as the basis of the experiment. The sound permeability of the urethra sacculus and balloon was good, and the imaging quality of baseline ultrasound, 2DCEUS and 3DCEUS was satisfied. By injecting diluted contrast agent of different concentration into each section of the phantom, the pre- and post-ablation situation can be mimicked. It should be noted that the volume of fluid that was injected into the same section should be consistent in both pre-ablative and post-ablative situations. CT images were served as the reference standard, and diluted CT contrast agent was injected into the section of mimicked AM, which were high density and easily observed and measured on CT image. In addition, the volume of liquid injected into each section should be the same as that of 3DCEUS imaging.
In the water tank phantom, the mimicked AM measured on 3DCEUS-FI had high accuracy and inter-observer agreement. 3DCEUS-FI had high registration efficiency and a registration success rate of 81.9%. With CT images served as the reference standard, the length of mimicked AM in six directions evaluated with 3DCEUS-FI analysis were in good agreement with the values that measured on CT images, which demonstrated the high accuracy of 3DCEUS-FI. Besides, the repeatability to measure mimicked AM with 3DCEUS-FI was high, both within inter-observer and intra-observer measurements.
In this study, an orthogonal experiment design was used to explore the influencing factors of 3DCEUS-FI registration success rate, and to investigate whether the size, depth, enhancement level of mimicked tumor, diameter and number of mimicked adjacent vessels could affect registration success rate. The orthogonal experiment design is a method that selects some representative experiment conditions to represent comprehensive experiment to carry out the experiment according to the orthogonality. By analyzing these conditions, the situation of the comprehensive experiment could be understood, which optimizes the scientific research process. It is an efficient and cost-effective design method [28]. In this study, the orthogonal table was designed according to the possible influence factors and the levels of the factors, and orthogonal parameters were reserved in consideration of the possible influence factors, the error, and the possible interaction term. Therefore, L36 (33×22) orthogonal table was selected for both situations of mimicked AM < 5 mm and mimicked AM≥5 mm, and 72 trials were carried out. The results of regression analysis showed that diameter of the mimicked adjacent vessels was significantly related to success rate of registration, and the success rate of registration was significantly reduced when diameter of mimicked vessels was 2 mm. On the other hand, there was no significant correlation between the size, depth, enhancement level of the tumor, number of mimicked adjacent vessels and the success rate of 3DCEUS-FI registration. In current situations, 3DCEUS-FI completes the registration by identifying the corresponding large blood vessels (diameter≥3 mm) on two images. The registration algorithm is mainly based on the contrast of gray-scale intensity between tumor and adjacent vessels, and the vessels were recognized as anatomical landmarks. In this study, the registration success rate was significantly lower when diameter of mimicked vessel was 2 mm than that when diameter of mimicked vessels was 3 mm and 4 mm, which was consistent with the algorithm foundation of the technique. In addition, in order to obtain enough AM during the ablation process in clinical practice, vessels with a diameter of no more than 2 mm adjacent to the tumor are damaged [29], which results in failure to be registration landmarks on post-ablative images. Therefore, when 3DCEUS-FI interactive registration is employed in clinical practice, the radiologists should mark intrahepatic vessels with a diameter≥3 mm as registration landmarks.
Owing to the study design, there are some limitations of our study. Since this is an in vitro experiment, the experimental conditions are easy to control. However, it will be affected by the patient’s respiratory movement and heart beat when acquiring 3DCEUS images in clinical application, and ultrasonic beam can be reflected and blocked by ribs and lungs. Besides, the lesion borders of some malignant lesions are irregular. These borders are different from the clear borders used in this work, which might influence the statistical analysis. Therefore, 3DCEUS-FI still needs further evaluation in clinical application.
Conclusion
The mimicked AM measured on 3DCEUS-FI had high accuracy and inter-observer agreement. Diameter of the mimicked adjacent vessels was significantly related to success rate of registration.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
Funding
This work was supported by the National Natural Science Foundation of China (Grants No. 81530055 and No. 81501493) and the State Key Project on Infectious Diseases of China (2018ZX10723204).
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.