
Abstract
OBJECTIVE:
To establish a nomogram for predicting cervical lymph node metastasis (CLNM) based on the preoperative conventional ultrasound (US) and shear wave velocity (SWV) features of papillary thyroid carcinoma (PTC).
METHODS:
A total of 101 patients with pathologically confirmed thyroid nodules were enrolled. These patients were divided into the CLNM-positive (n = 40) and CLNM-negative groups (n = 61). All patients underwent the preoperative conventional US and shear wave elastography (SWE) evaluation, and the US parameters and SWV data were collected. The association between SWV ratio and CLNM was compared to assess the diagnostic efficacy of SWV ratio alone as opposed to SWV ratio in combination with the conventional US for predicting CLNM.
RESULTS:
There were significant differences in shape, microcalcification, capsule contact, SWV mean, and SWV ratio between the CLNM-positive and CLNM-negative groups (P < 0.05). Logistic regression analysis showed that taller-than-wide shape, microcalcification, capsule contact, and SWV ratio > 1.3 were risk factors for CLNM; Logistic(P)=-6.93 + 1.647 * (microcalcification)+1.138 * (taller-than-wide-shape)+1.612 * (capsule contact)+2.933 * (SWV ratio > 1.3). The area under the curve (AUC) of the receiver operating characteristic (ROC) of the model for CLNM prediction was 0.87, with 81.19% accuracy, 77.5% sensitivity, and 85.25% specificity.
CONCLUSION:
The nomogram based on conventional US imaging in combination with SWV ratio has the potential for preoperative CLNM risk assessment. This nomogram serves as a useful clinical tool for active surveillance and treatment decisions.
Keywords
Introduction
Thyroid carcinoma (TC) is the most common malignant tumor of the endocrine system [1]. Papillary thyroid carcinoma (PTC) accounts for about 75–85% of the pathological types within TC [1, 2]. While PTC has an indolent clinical course, metastasis is an important issue in clinical management. About 30–80% of PTC patients with central lymph node metastasis (CLNM) have a stable high survival rate worldwide [3, 4]. However, CLNM is a risk factor that increases local tumor recurrence and decreases survival in certain high-risk groups [5–7]. Thus, preoperative imaging assessment of the PTC and central lymph node (CLN) is crucial for the prediction of metastasis, which can affect the treatment and surgical decisions.
High-resolution ultrasound (US) is the first-line imaging modality for the preoperative assessment of thyroid cancer [8, 9]. It enables the assessment of extrathyroidal extension (ETE), tumor size, and CLNM, thereby determining the stage of PTC and influencing the treatment and the extent of surgery [10, 11]. However, US for detecting CLNM in PTC has low sensitivity (36.7–61.0%) despite having high specificity (85.0–97.4%) [12]. It has been reported that in up to 90% of PTC with CLNM, the CLN microscopic metastases exhibited false-negative US characteristics indicating the requirement for an improved diagnostic method [4]. Recently, the association between tumor stiffness and pathological characteristics was established, and hence US elastography was suggested as a diagnostic tool for predicting ETE and CLNM [13, 14]. Acoustic radiation force impulse (ARFI) is another US-based elastography technique that allows quantitative (i.e., virtual touch tissue quantification, VTQ) and qualitative (i.e., virtual touch tissue imaging, VTI) estimation of tissue stiffness. While the conventional US cannot provide useful information on tumor hardness, shear wave elastography (SWE) can quantitatively evaluate tissue hardness with adequate repeatability [15, 16]. However, the effect of carotid artery pulsation on SWE has not been considered in previous studies [4, 17].
The purpose of this study was to explore the utility of the shear wave velocity (SWV) ratio for predicting preoperative CLNM in PTC. In addition, the study also explores whether the SWV ratio can improve the accuracy in diagnosing CLNM compared to SWV.
Materials and methods
The inclusion criteria in our study were: 1) the thyroid nodule was pathologically proven to be PTC, 2) underwent central lymph node dissection, 3) underwent conventional US and ARFI examinations in our institution, and 4) age≥18 years old (Fig. 1). The exclusion criteria included: 1) history of radiotherapy, radiofrequency ablation, or chemotherapy, 2) the target tumor was unclear on US images due to artifacts, and 3) diagnosed with other malignancies of thyroid tumors simultaneously, hyperthyroidism and hashimoto. Based on these criteria, among the 527 patients, a total of 101 consecutive patients with 101 thyroid nodules were included in our study. The study inclusion process is depicted in Fig. 1.

The process for patient enrolment.
Categorical and continuous variables were expressed as numbers and percentages, respectively. The values were expressed as mean±standard deviation. Chi-square and Fisher’s exact tests were used to compare the ratios. Means were compared using the Mann-Whitney test and Student’s independent t-test. Univariate logistic regression analysis was performed to assess the association between each asset and the presence of CLNM. Multiple logistic regression analysis was used to select the main independent predictors of CLNM. For univariate logistic regression, we created nomogram infographics using stepwise regression for variables with P < 0.05. The evaluation criteria are defined according to the regression coefficients of each variable. CLNM risk factor lines and eigenvalues were drawn according to the rating scale. The area under the curve (AUC) of the receiver operating characteristic (ROC) was calculated to evaluate the predictive performance of the model. The fit of the final model was assessed using the Hosmer-Lemeshow (HL) test. The DeLong test was performed to compare the AUC of two models and P < 0.05 was considered significant. Statistical analyses were performed using the software SPSS V26.0 (IBM Corp.) and Stata15.0.
Results
Among the 101 patients included in this study with pathologically confirmed PTC, 20 were males and 81 were females. A total of 40 PTC patients were positive for CLNM (39.6%), and 61 were negative for CLNM (60.4%). Among the CLNM-negative group, 51 were females and 10 were males. The CLNM-positive group comprised 31 females and 9 males. The mean maximum diameter of the nodules was 18.9±8.1 mm (range: 5.0 to 42.6 mm) which showed no association with CLNM (both P > 0.05) (Table 1).
US and SWV features of all patient
US and SWV features of all patient
The optimal cutoff values of SWV mean and SWV ratio for distinguishing PTC patients with and without CLNM were calculated to be 3.44 m/s and 1.3 respectively. These cut-off values were determined according to the ROC curve analysis. Interestingly, the SWV mean and SWV ratio were significantly higher in the CLNM-positive group than in the CLNM-negative group (P = 0.004 and 0.000, respectively). The values of the SWV mean and SWV ratio for predicting CLNM are shown in Table 2. SWV ratio showed the higher AUC for predicting CLNM (0.717; 95% CI = 0.616 to 0.819) however, was not significantly different from the AUC of SWV mean (0.709; 95% CI = 0.610 to 0.795) (P < 0.05).
Multivariate analysis of US and SWV for predicting CLNM
Conventional US characteristics of the PTC patients with and without CLNM are summarized in Table 1. We found that the conventional US features such as taller-than-wide shape, microcalcification, and capsule contact of PTC were significantly associated with CLNM (P < 0.05). In contrast, parameters such as tumor size, echogenicity, vascularity, boundary, and multifocality showed no clear association with CLNM (P > 0.05). Capsule contact (P < 0.001), taller-than-wide shape (P = 0.003), and microcalcification (P < 0.001), were more frequently found in PTC patients with CLNM than in those without CLNM suggesting they could be potential prognostic factors for predicting CLNM.
In the multivariate analysis, apart from the taller-than-wide shape, other factors such as microcalcification, capsule contact, and SWV ratio were also observed to be independent predictors for CLNM. Through binary logistic regression, these 4 independent risk factors were screened for predicting CLNM in PTC patients. The CLNM predictive scoring system for patients with PTC was established based on the coeffects of these factors along with the regression coefficients. (Table 2). The predicted scores (P)=-6.93 + 1.647 * (microcalcification)+1.138 * (taller-than-wide-shape)+1.612 * (capsule contact)+2.933 * (SWV ratio > 1.3) (existence of microcalcification: yes = 1, no = 0; taller-than-wide shape: yes = 1, no = 0; capsule contact: yes = 1, no = 0; SWV ratio > 1.3: yes = 1, no = 0) (Fig. 2). The AUC was 0.87 [95% CI, 0.802–0.939], indicating that the predictive scoring model performed satisfactorily.
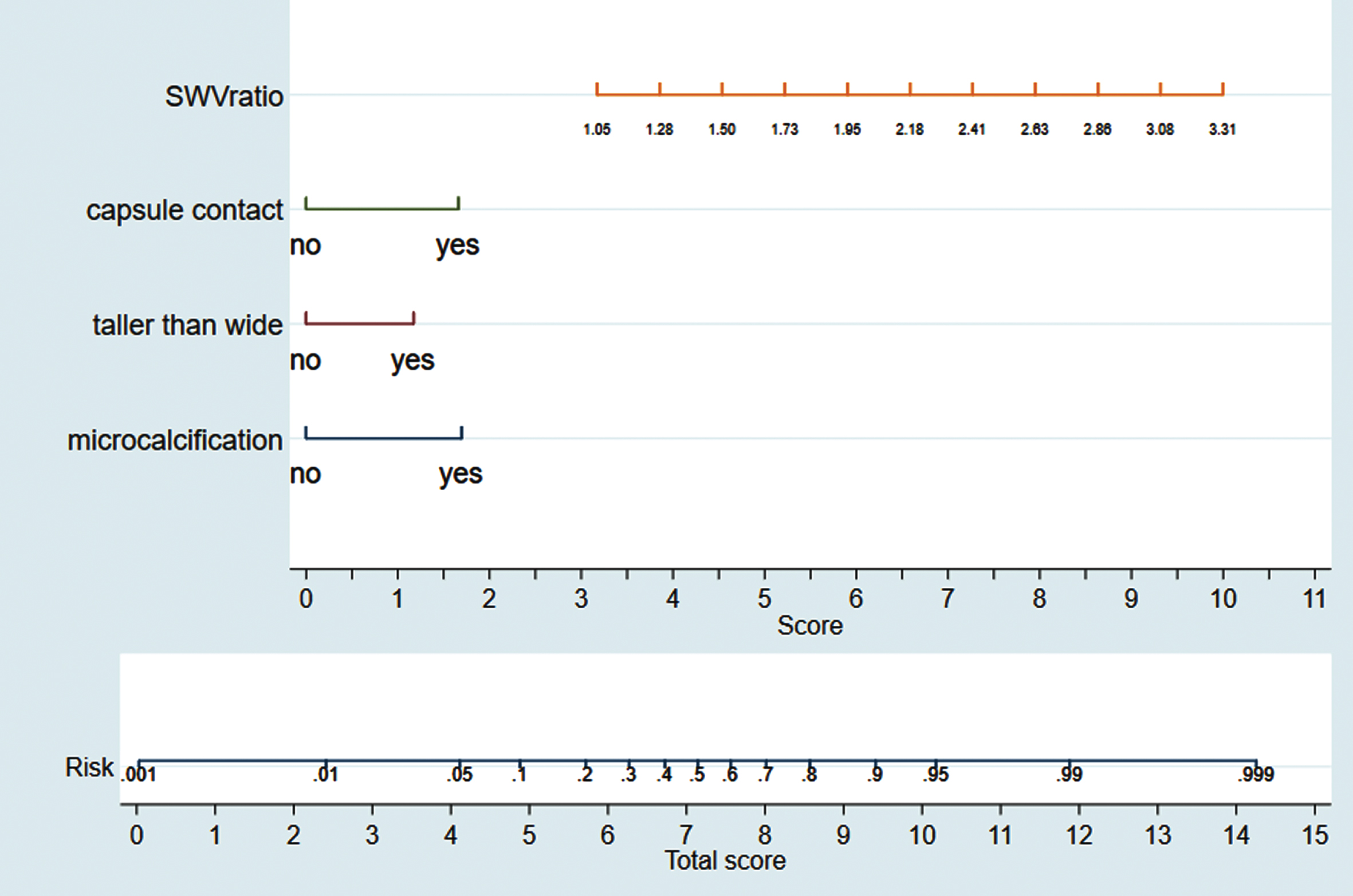
Nomogram for predicting the risk of CLNM in patients with PTC.
In addition, we constructed a nomogram with the above 4 independent predictors associated with contralateral CLNM (Fig. 3). Each predictor is assigned a specific number from 0 to 100 points. The estimated incidence of CLNM in PTC patients was determined by summing the total scores and placing them on the total subscale.
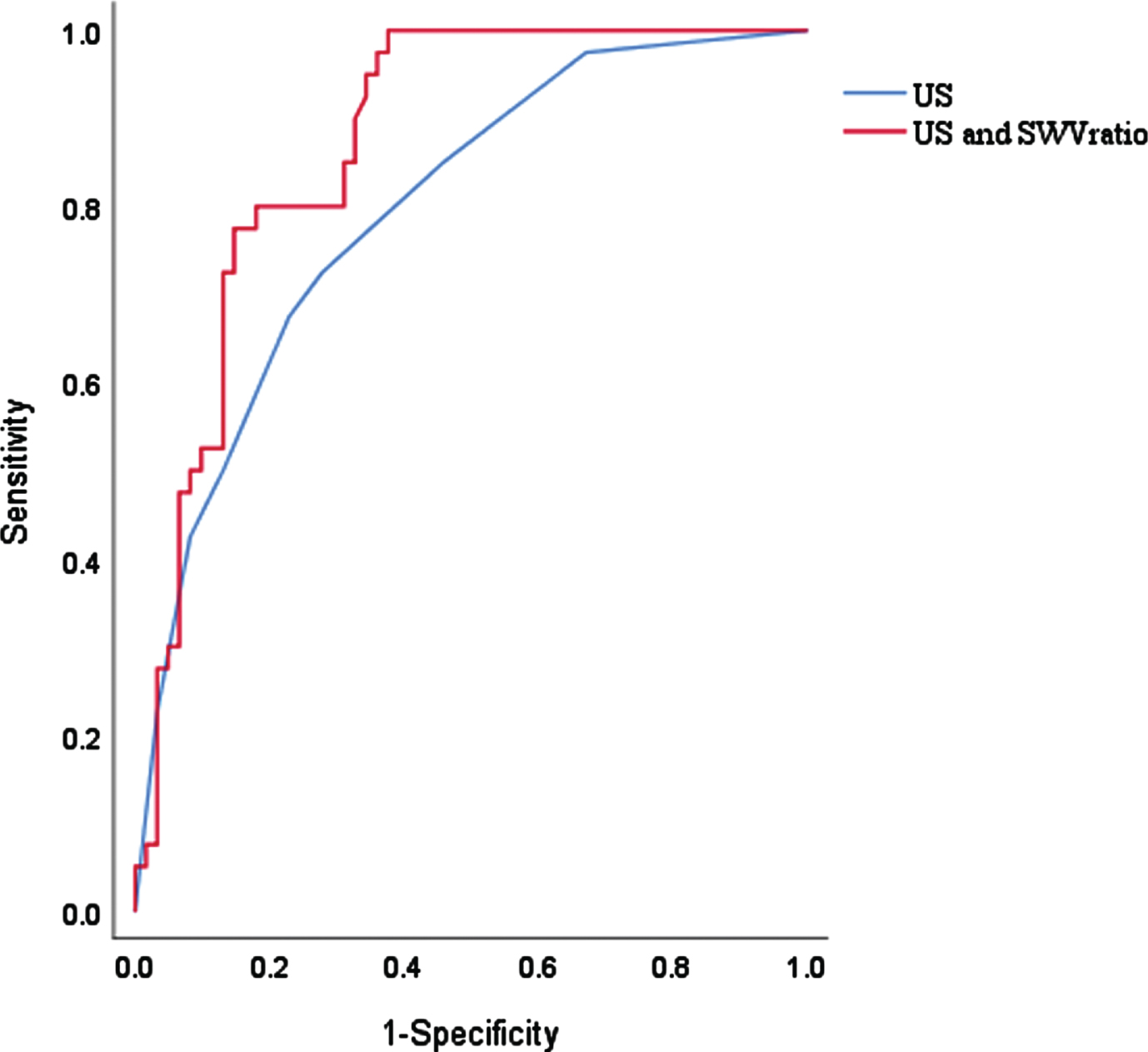
ROC for the discrimination of the nomogram.
The presence of metastatic lymph nodes (LNs) in PTC patients may increase the incidence of local recurrence, and regional and distant metastasis, and affect the disease-free and overall survival rates [7, 19]. Even though preoperative neck US has played a crucial role in the diagnosis of CLNM, the detection rate of CLNM by the conventional US is unsatisfactory [20]. In our study, the occult metastasis rate of CLN in patients with PTC was 39.6% and among the preoperative conventional US parameters, taller-than-wide-shape, capsule contact, and microcalcification were identified to be the independent prognostic factors to predict CLNM. Our study showed that the sensitivity and specificity of the independent conventional US prognostic factors for the evaluation of CLNM are 72.5% and 72.13%, respectively. Multiple independent studies have been conducted in the past to identify the risk factors for CLNM in PTC, but no consensus has been reached. It has been reported that the tumor size, echogenicity, wider-than-tall shape, and ETE, were significantly associated with CLNM [21, 22]. However, the expertise of the operator significantly affects the accuracy of the diagnosis. Therefore, novel complementary techniques and risk factor models are required to improve the diagnostic performance and prediction of CLNM.
SWE is a new tool that has been used to quantitatively evaluate tissue stiffness with reasonable repeatability [23, 24]. Studies have indicated that SWV exhibited a significant association with CLNM [17, 26]. Our study indicated that SWV mean and SWV ratio were correlated with CLNM in the univariate analysis, though SWV mean was not an independent factor for predicting CLNM in multivariate analysis. Further, SWV ratio was found to be a better predictor of CLNM (0.717; 95% CI = 0.616 to 0.819) compared to SWV mean (0.709; 95% CI = 0.610 to 0.795), though the difference was not statistically significant. These findings from our study are consistent with previous literature [26]. However, in a recent survey of 116 PTC patients with BRAFV600E mutation, the SWV ratio showed no association with CLNM [27]. This contrasting result reported by Xu et.al could potentially be due to the differences in the population included in the study, as PTC patients with BRAFV600E mutation alone were enrolled in their study [27].
A multivariate logistic regression analysis indicated that microcalcification, taller-than-wide shape, capsule contact, and SWV ratio > 1.3 were significant predictive variables for CLNM. The preoperative diagnostic nomogram model developed in this study used four variables to predict CLNM potential, including microcalcifications, height-width shape, capsular contact, and SWV ratio. Our nomogram prediction model has excellent detection capabilities. In the training set, the AUC of the nomogram prediction model was 0.87, and its prediction performance was better than that of the conventional US risk factor prediction model.
Our study has a few potential limitations. This study is a single-center retrospective analysis with a limited sample size, which might have skewed the results. The application of nomograms requires rigorous validation which in general involves large-scale multi-institutional studies to ensure the accuracy and reproducibility of the results. Further, our study did not include long-term follow-up of patients. Prospective studies with long-term follow-up are essential for an accurate assessment of the utility of the SWE elasticity index as a predictor of CLNM in PTC patients.
In conclusion, this retrospective study identified that microcalcification, taller-than-wide shape, capsule contact, and SWV ratio > 1.3 predicts CLNM risk in patients with PTC. The nomogram developed based on conventional US imaging and SWV ratio has the potential for preoperative CLNM risk assessment. This nomogram could serve as a useful clinical tool for active surveillance and treatment decisions.
Footnotes
Acknowledgments
The study was supported in part by Grant 20204Y0343 from Shanghai Municipal Health Commission, Shanghai, China.