
Abstract
BACKGROUND & OBJECTIVE:
We aimed to evaluate the effect of sitaxentan on renal microvascular perfusion via application of ultrasound microbubble contrast.
METHODS:
Male beagles were randomly divided into: Sham, cardiopulmonary bypass (CPB) and sitaxentan-infused (Sit) groups (n = 6). The ascending slope rate (ASR), area under the curve (AUC), derived peak intensity, and time to peak (TTP) were obtained via ultrasound microbubble contrast before CPB (T1), after 1 h CPB (T2), at end of CPB (T3), and 2 h after CPB (T4).
RESULTS:
Compared with the Sham group, the CPB group had lower ASR of the renal cortex and medulla at T2 - 4, higher AUC and TTP at T3 - 4, and lower derived peak intensity at T4. The ASR at T2 - 4 in the Sit group was lower, TTP was higher at T2 - 4, and AUC was higher at T3 - 4 (P < 0.05). Compared with the CPB group, the Sit group had higher ASR of the renal cortex and medulla at T3 - 4 and AUC and TTP at T3 - 4 (P < 0.05). Compared with that at T1, the ASR of the renal cortex and medulla at T2 - 4 in the CPB group was lower, and AUC and TTP were higher at T3 - 4. The ASR of the renal cortex and medulla at T2 - 4 in the Sit group was lower, TTP was higher at T2 - 4, and AUC was higher at T4 (P < 0.05).
CONCLUSIONS:
Ultrasound microbubble contrast could be effectively used to evaluate renal microvascular perfusion peri-CPB in beagles, which was prone to decrease and could be improved via pretreatment with sitaxentan.
Introduction
Patients undergoing cardiopulmonary bypass (CPB) are prone to a higher incidence of acute kidney injury (AKI) [1, 2], which accounts for the main cause of perioperative mortality [2, 3]. Studies on AKI following coronary artery bypass graft surgery using the Acute Kidney Injury Network (AKIN) classification have shown that small increases in serum creatinine level (AKIN class 1) increase the risk of end-stage renal disease by 3-fold and that of mortality by nearly 1.5-fold [4]. Therefore, early diagnosis and treatment are key to prevention and treatment [5, 6]. Renal perfusion is closely related to CPB-associated AKI, and all regions of renal perfusion decrease significantly after the initiation of CPB [7, 8]. This may because venous drainage during CPB can generate a negative central venous pressure (CVP). Vacuum-assisted venous drainage with even lower CVP might result in higher flow to maintain circulation, leading to reduced microcirculatory perfusion of the tissue [9]. Endothelin is a potent vasoconstrictor with two receptors: endothelin A receptor and endothelin B receptor. The endothelin A receptor is mainly expressed in smooth muscle cells in renal vessels, antagonists of which can selectively dilate renal vessels and improve renal microcirculation [10–12]. In contrast, the endothelin B receptor is principally involved in the clearance of endothelin, particularly in the vascular beds of the lung and kidney [13]. Sitaxentan is a kind of selective antagonist of the endothelin A receptor, which may block the vasoconstrictor effects of the receptor while maintaining the vasodilator and clearance functions of the endothelin B receptor [14]. This study aimed to use ultrasound microbubble contrast to perform real-time, non-invasive, and accurate renal microcirculation monitoring to evaluate the effect of high-selective endothelin A receptor antagonist on renal microcirculation in beagles undergoing CPB. Our findings will provide a theoretical basis for clinical medical care.
Materials and methods
Our animal protocol was approved by the Animal Care and Use Committee at Affiliated Hospital of Southwest Medical University in accordance with the requirements of the Chinese Animal Care Committee. All protocols that used animals were in compliance with the ARRIVE guidelines (https://arriveguidelines.org). Beagles were healthy, with no heart or lung disease, no anemia and hypoproteinemia, and no lung damage caused by biological and physicochemical substances.
Eighteen male beagles (10–15 kg, aged 2–4 years) were randomly divided into three groups (n = 6): Sham group (thoracotomy followed by 4 h observation), CPB group (2 h CPB followed by 2 h observation), and Sit group (sitaxentan infusion for 1 h prior to 2 h CPB, followed by 2 h observation).
Intraperitoneal injection of pentobarbital (25 mg/kg) was followed by dynamic monitoring of vital signs using the Dash 3000 monitor, including invasive blood pressure detected from femoral artery, temperature, heart rate, electrocardiogram, and percutaneous blood oxygen saturation in ears. Anesthesia was maintained after intubation with intravenous infusion of fentanyl (0.2μg/kg/min) and vecuronium (0.2μg/kg/min) after establishment of a peripheral venous channel through the superficial vein of a hind limb. Ventilation parameters were set with 10 ml/kg tidal volume and 16–20 breaths/min of respiratory rate to maintain PETCO2 at 35–45 mmHg (1 mmHg = 0.133 kPa). We did not use vasoconstrictive medication during CPB or after weaning.
When vital signs were stable, a middle incision was made to expose the major blood vessels, followed with intravenous administration of heparin (3 mg/kg). An aortic and venous cannula was placed in the right atrial appendage after the activated clotting time of whole blood was > 380 seconds; CPB was initiated after activated clotting time was > 480 seconds. St. Thomas cardioplegia (20 ml/kg) was infused 10 min after the initiation of CPB from the root of the aorta with the aortic cross-clamp to ensure a bloodless surgical field and to protect the myocardium [15]. Extra 10 ml/kg St. Thomas cardioplegia was infused every 30 minutes. CPB was performed for 2 h (32–34°C, 70–100 ml/kg/min) with 2 h aortic cross clamping; mean arterial pressure was maintained at 50–70 mmHg, and hemoglobin was maintained at > 70 g/L. The beagles were weaned from CPB after stabilizing the internal environment and hemodynamics and received protamine to neutralize heparin, followed by another 2 h of observation in the CPB and Sit groups. Then, 0.7 mg/kg sitaxentan (B29F7E10070, Shanghai Source Leaf Biotechnology Co., Ltd.) infusion was administrated for 1 h prior to 2 h CPB in the Sit group.
Renal microcirculation was evaluated via ultrasound microbubble contrast, which used the real-time harmonic supersonic imaging conditions with low mechanical index (M 10.06). The Philips iU-22 system (Philips, the Netherlands) and the probe type C5-1 were used at the following four time points: before CPB (T1), after 1 h CPB (T2), end of CPB (T3), and 2 h after CPB (T4) (Fig. 1). The 1 ml ultrasound microbubble contrast agent, which was a hexafluoride sulphur microbubble (Brac co, Italy) with a microbubble density of 2×108/ml and an average diameter of 2.5μm, was injected into the central vein followed by 5 ml of physiological saline. The data were analyzed using QLAB quantitative analysis software (Philips). Two regions of interest, renal cortex and renal cone, were selected to detect changes in the number of echoes of each pixel and contrast agent microbubbles to obtain the time-intensity curve of renal microvascular perfusion. The relevant quantitative parameters, including ascending slope rate (ASR), area under the curve (AUC), derived peak intensity (DPI), and time to peak (TTP), were obtained after Gamma Fitting I(t)=A*t*exp(-t)+c (Fig. 2) [16, 17].

Flow scheme of experimental animal procedures. Subjects were divided into three groups: Sham, cardiopulmonary bypass (CPB), and Sit groups. Sitaxentan was infused in the Sit group for 1 h prior to 2 h CPB. Renal cortex and medulla microvascular perfusion parameters were detected at the following four time points: before CPB (T1), after 1 h CPB (T2), end of CPB (T3), and 2 h after CPB (T4).

Renal microvascular perfusion parameters. A) Ascending slope rate (ASR), B) derived peak intensity (DPI), C) time to peak (TTP), and D) area under the curve (AUC) were obtained via ultrasound microbubble contrast. The decreased ASR and DPI, prolonged TTP, and increased AUC indicate decrease in renal microvascular perfusion.
Data were analyzed using SPSS 20.0 (IBM). Physiological data were assessed for time effect and treatment using Two-Way ANOVA with repeated measurement. Tukey’s test was used to adjust P value results. Unless otherwise noted, data are presented as the mean or percentage (%). Significance was defined as a two-sided P-value<0.05.
Results
Compared with that of the Sham group, the ASR of the renal cortex and medulla at T2 - 4 in the CPB group was lower, AUC and TTP were higher at T3 - 4, and DPI was lower at T4. Compared with that of Sham group, the ASR at T2 - 4 in the Sit group was lower, TTP was higher at T2 - 4, and AUC was higher at T3 - 4 (P < 0.05) (Figs. 3 4). Compared with that of the CPB group, the ASR of the renal cortex and medulla at T3 - 4 in the Sit group was higher, and AUC and TTP were higher at T3 - 4 (P < 0.05) (Figs. 3 4). Compared with that at T1, the ASR of the renal cortex and medulla at T2 - 4 in the CPB group was lower, and AUC and TTP were higher at T3 - 4. The ASR of the renal cortex and medulla at T2 - 4 in the Sit group was lower, TTP was higher at T2 - 4, and AUC was higher at T4 (P < 0.05) (Figs. 3 4).
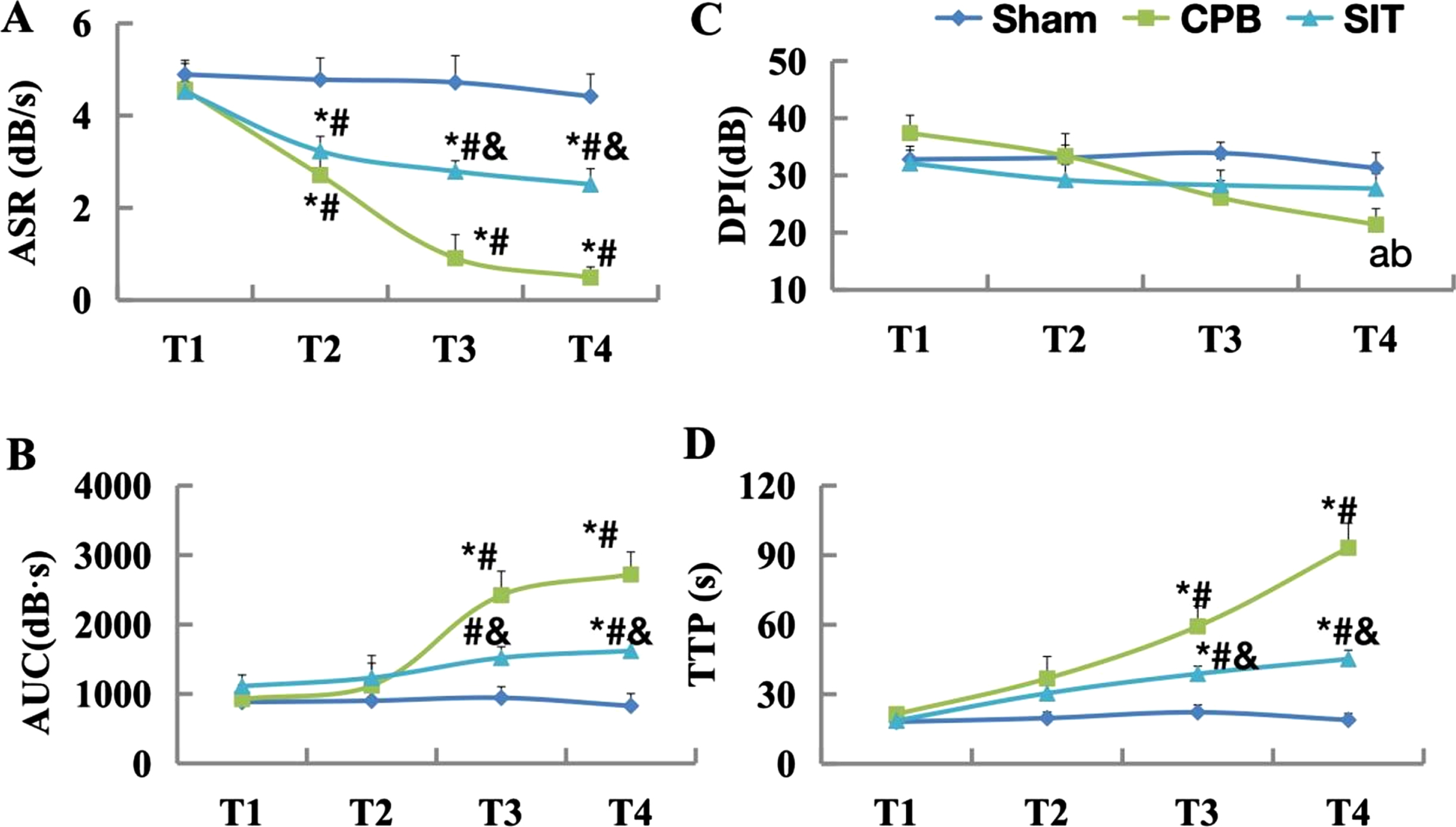
Changes in renal cortex microvascular perfusion. A) Ascending slope rate (ASR), B) area under the curve (AUC), C) derived peak intensity (DPI), and D) time to peak (TTP). *, P < 0.05 vs. T1; #, P < 0.05 vs. Sham; &, P < 0.05 vs. CPB.
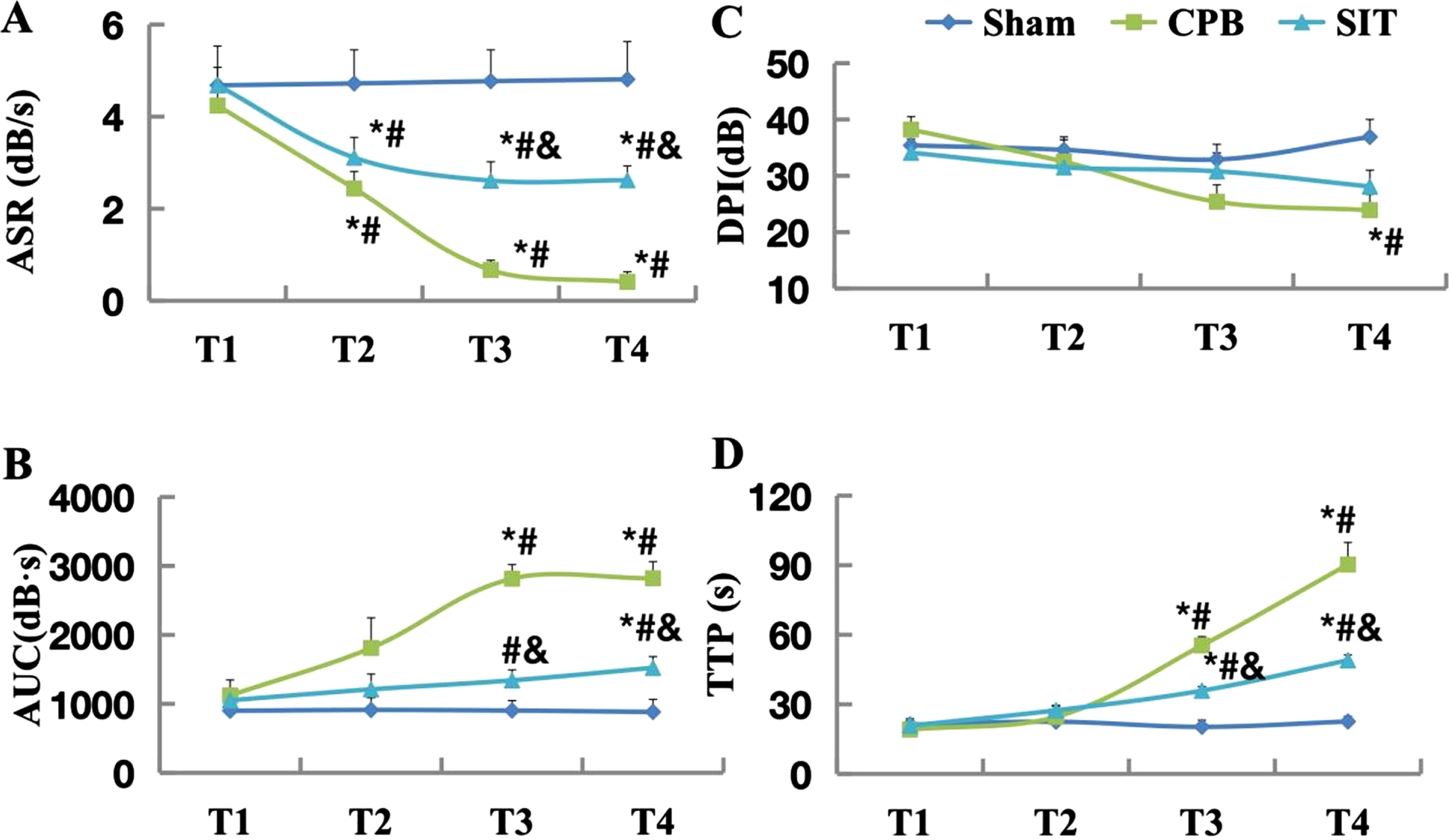
Changes in renal medulla microvascular perfusion. A) Ascending slope rate (ASR), B) area under the curve (AUC), C) derived peak intensity (DPI), and D) time to peak (TTP). *, P < 0.05 vs. T1; #, P < 0.05 vs. Sham; &, P < 0.05 vs. CPB.
AKI is a serious complication of cardiac surgery, affecting a considerable proportion of patients and increasing postoperative morbidity and mortality [18]. In previous studies, a tracer was administrated to image renal radionuclides and renal blood flow. However, this could not clearly distinguish the renal medulla and cortex blood flow and, most concerningly, exhibits radioactivity [19]. Computed tomography and magnetic resonance imaging perfusion imaging can dynamically assess renal blood flow, but such methods require large, expensive equipment and facilities [20, 21]. Ultrasound microbubble contrast can non-invasively and accurately monitor renal microvascular perfusion in real-time. The method is easy and fast to perform, there is no radiation or renal toxicity, and it can achieve the same evaluation efficiency as radionuclide imaging [8, 22]. Decrease of ASR and DPI, prolonged TTP, increase of AUC indicate decrease of renal microvascular perfusion [8, 16].
Kidney function depends on oxygen delivery, especially under the conditions of nonpulsatile flow generated by CPB. As a result of its blood supply, the kidney enters the hypoxic state under conditions of progressive acute anemia much earlier than the intestine and the heart [23]. Lannemyr et al. demonstrated that renal DO2 is decreased by 20% following hemodilution and vasoconstriction during CPB, and there is an increase in renal oxygen extraction of up to 45%, which indicates a renal oxygen supply/demand mismatch [24]. Maintaining DO2 levels above the recommended threshold during CPB improves physiological and clinical outcomes and can ensure balance between the supply and demand of renal oxygen, which has been described as goal-directed perfusion [25–28]. A recent systematic review and meta-analysis detailed the goal-directed perfusion strategy during CPB and reported that AKI stage 1 is evidently reduced, which reduces overall AKI incidence [29]. In the present study, the peri-CPB average arterial pressure was maintained above 60 mmHg, which was above the normal perfusion pressure previously identified [30, 31]. However, although this experiment met the requirements of goal-directed perfusion, AKI occurred. Ultrasound microbubble contrast showed significantly decreased ASR and DPI, prolonged TTP, and increased AUC, which indicated the deterioration of perfusion in the renal cortex and medulla. These results were in accordance with those reported from previous studies [32, 33]. The reason may be that nonpulsatile perfusion of CPB is non-physiological, and renal microvascular perfusion may also be reduced even under normal perfusion pressure [34]. The underlying cause of the changes should be investigated in detail in future studies. Sitaxentan is a kind of selective antagonist of the endothelin A receptor which is hypothesized to offer an advantage over endothelin A/endothelin B receptor blockade by allowing the endothelin B receptor in endothelial cells to release the vasodilators nitric oxide and prostacyclin and clear ET-1, while suppressing the vasoconstrictor and proliferative actions of the endothelin A receptor [35]. We selected the dosage of IV infusion of sitaxentan (0.7 mg/kg) according to a previous study [36], and administration was carried out 1 h before CPB in accordance with pre-experimental results [8]. The results of the present study showed that ASR increased and AUC and TTP decreased as detected by ultrasound microbubble contrast after pre-CPB administration of sitaxentan, which indicated improvement of renal microvascular perfusion. Barst et al. [37] reported that endothelin A might reduce renal blood flow and glomerular filtration rate without decreasing systemic arterial pressure, which could be reversed by its antagonists; these results support our study. Whether sitaxentan plays a protective effect in renal function via improvement of renal microcirculation remains unknown and requires further study. In summary, sitaxentan could improve renal microcirculation in beagles during CPB; however, the extent of potential improvements remains to be further studied.
Funding
This study was financially supported by Doctoral Research Initiation Fund of Affiliated Hospital of Southwest Medical University (19022).