
Abstract
BACKGROUND:
Resistance exercise induces thrombocytosis and increases platelet activation and function. These changes might be related to exercise variables including exercise intensity and type.
OBJECTIVE:
We compared the effects of traditional resistance exercise (TRE) and circuit resistance exercise (CRE) on cellular markers of platelet activation and function.
METHODS:
In this crossover study ten healthy male (mean±SD: age, 25.6±2.4 years) subjects performed TRE encompassed 3 sets of 10 repetitions at 100% of 10-RM (10 repetition maximum) for 6 exercises, and CRE protocols included 3 sets of 10 repetitions at 100% of 10-RM for all 6 exercises consecutively, in two separate weeks. To measure platelet indices, PAC1, CD41a, CD42b and CD62P three blood samples were taken before, immediately after exercise, and after 30 min recovery.
RESULTS:
Lactate concentration, blood pressure, platelet count (PLT), and mean platelet volume (MPV) were significantly (p < 0.05) increased following both resistance exercise trials. Significant increases in PAC1, and CD62P; and significant reductions for CD42b and CD41a were detected following both REs (p < 0.05). However, changes in PAC1 and CD62P were significantly different between the two protocols (p < 0.05), with higher increases detected following CRE.
CONCLUSIONS:
Acute RE increases platelet indices and platelet activation; and that CRE results in higher platelet activation than TRE, probably due to exercise-induced increases in shear stress.
Introduction
Imbalance in the hemostasis system is one of the major leading causes of cardiovascular disease, which can lead to thrombosis and heart attack [1]. Platelets contribute to hemostasis through adhesion, activation, and formation of platelet plug [2]. The main physiological functions of platelets are to preserve hemostasis, prevent blood loss and maintain vascular integrity [3, 4]. On the other hand, uncontrolled thrombosis or platelet dysfunction leads to blood vessel obstruction and cardiovascular complications [3, 5]. Platelets play their role through interactions between external tissues (blood and endothelial) and their surface glycoproteins including complex GPIb/IX/V, integrin receptor of αIIbβ3 (GPIIb/IIIa) and P-selectin (CD62P) [6, 7].
The acute and chronic effects of exercise on hemostasis have been extensively investigated and reviewed [8–10]. A strong association between increases in level of physical activity and improvements in platelet activation and functions has been indicated [2].
Resistance training is a type of exercise training that is prescribed not only for athletes, but also for healthy individuals and patients with different types of diseases (cardiovascular, metabolic and etc) [11–13]. However, studies into effects of resistance exercise on platelet activation and functions are limited [1, 14–17]. For example, Creighton et al. (2013) demonstrated that responses of platelet activation to resistance exercise is reduced in resistance trained individuals, as shown by a reduction in plasma concentrations of B-TG in resistance trained group [15]. On the other hand, acute resistance exercise has resulted in thrombocytosis and platelet activation [1, 14] in an intensity related manner [1].
Based on manipulating exercise variables (i.e. intensity, duration, and rest intervals), various resistance exercise protocols with specific objectives could be designed [11]. Different resistance exercise protocols induce various hormonal and metabolic responses [18–20]. Traditional resistance training (TRT) involves completing 1 to 3 sets of exercise with moderate to heavy loads and long recovery periods after each set [11]. Studies have shown greater strength increases with longer rest periods between sets compared to short rests, (e.g., 2–3 min vr 30–40 s) [11]. This type of exercise is associated with substantial increases in bone and muscle mass and strength [21–23], which are important for improving the muscular function and health in both athletes and clinical populations [24, 25].
Circuit weight training (CWT) is another type of resistance exercise that combines the stresses of both aerobic and resistance exercise and consists of performing a predetermined set of exercises (a circuit) for a certain period of time or for 10–15 repetitions with short rest (5–30 s) periods [26, 27]. CWT can maintain and improve cardiovascular fitness [28–31], body composition [29], muscular strength [28, 29], and muscular endurance [29–31]. This method of training attempts to increase exercise intensity by having no rest between exercises and shortening the rest between sets. It has been suggested that healthy individuals produce the same muscular performance under a traditional resistance exercise (TRE) and circuit resistance exercise (CRE) session, though; the cardiovascular response to the CRE is significantly greater [32]. These data suggest that a CRE using moderate to heavy loads might elicit greater cardiovascular stress and complications than TRE.
An important goal of clinical exercise and athletic training programs is to optimize strength, muscle mass, and body composition, while improving cardiovascular fitness. Nowadays, resistance exercise is a part of rehabilitation programs in clinical settings for different populations.
Few studies have focused upon the responses of platelet activation and function to resistance exercise [1, 14], though, to our knowledge no study has investigated and compared the effects of resistance exercise type (particularly CRE) on these variables. Therefore, the purpose of our study was to determine the effects of CRE and TRE, and consequently compare these effects. Investigation of possible differences between these two types of resistance exercise could lead to optimal exercise prescriptions and provide greater insight into the underlying cellular mechanisms for responses of platelet activation to CRE and TRE.
Although, our study investigates the effects of moderate intensity resistance exercise, because of the participants’ fitness status (untrained healthy), this intensity is considered high, and based on the shorter rest period and higher cardiovascular responses in CRE session, our hypothesis is that changes in platelet activation and function following CRE would be greater than TRE.
Materials and methods
Participants
Ten healthy men (mean±SD: age, 25.6±2.4 years, height, 176±6 cm; weight, 76.0±4.8 kg; BMI, 24.6±1.1 kg/m2) voluntarily participated in the study. Exclusion criteria included having blood or platelet disorders, taking any platelet related medications, having a history of weight training, and joint problems or medical conditions that stop them from participating in a resistance exercise program (confirmed by a physician).
Participants were informed about the design of the study with possible risks and discomfort that might result from the study. Thereafter, the participants signed the written informed consent to participate in the study, which was approved by the University’s Ethics Committee (IR.SBU.REC.1399.058). The study was conducted according to the Declaration of Helsinki.
Study design and experimental protocol
Two familiarization sessions were designed to habituate participants with the testing procedures and resistance exercise protocols. The main aim of these sessions was to familiarize participants with different resistance exercises using weight-training machines and to carry out initial measurements for height, weight, and body composition. During the familiarization sessions, it was ensured that all participants performed the correct technique for all exercises before taking part in the maximum strength test (10-RM, ten repetitions maximum). Since the participants were untrained and in order to prevent injury, the 10-RM test was utilized to determine the participants’ maximum strength. Participants were asked to report to the laboratory in a separate session to determine 10-RM for six exercises, including chest press, leg extension, shoulder press, leg press, lat pull down and leg curl, which all were performed by using different weight training machines.
In this session, prior to performing the main exercise test, a general warm-up (5 min cycling on a stationary bike) and a specific warm-up (one set of 8 repetitions with light weight) were performed by all participants. For each exercise, the initial weight was mutually agreed between the participant and the researcher and was lifted 10 times using the correct technique. The weight was increased progressively until an unsuccessful trial occurred. The largest weight successfully lifted using the correct technique for each exercise was considered as the 10-RM (Table 1). Between each set and exercise, 2–3 min rest was given.
Values of the weight (Kg) corresponding to different exercise type
Values of the weight (Kg) corresponding to different exercise type
Participants were asked to return to the laboratory in two separate sessions (7-day washout) to perform the TRE protocol and a CRE workout. Participants were advised to avoid any physical exercise at least 24 hours prior to the test. In order to control the nutrition effects, they were provided with a standard low-fat breakfast two hours prior to the exercise. All the sessions were performed at the same time of day (08:00–10:00).
For both exercise trials, a general and specific warm-up similar to the 10-RM test was performed. In the TRE trial participants performed 3 sets of 10 repetitions at 100% of 10-RM for each exercise with one-minute rest between sets and exercises. In the CRE trial participants performed one set of 10 repetitions at 100% of 10-RM for all 6 exercises consecutively (no rest between exercises) and repeated the circle 3 times. In this trial, 3 min rest was allowed between sets. Both trials were followed by 30 min rest in the seated position. Blood pressure measurements and three blood samples were taken immediately before and after exercise, and after 30 min recovery. All participants performed both exercise protocols in a crossover manner.
Eight milliliters of blood was collected from an antecubital vein, with minimum stasis, after 20 min rest in a seated position, immediately after exercise, and after 30 min recovery. Blood samples were transferred in three tubes (the first tube contained EDTA, and the two other tubes contained sodium citrate) and were transferred to the laboratory for further assessment. The EDTA blood was used to assess hematocrit, hemoglobin, platelet count (PLT), mean platelet volume (MPV), and platelet distribution width (PDW) by using a Coulter Counter (Celltac Es MEK-7300, Nihon Kohden). Plasma volume was calculated from hematocrit and hemoglobin values by using Dill and Costill’s equation. For P-selectin assessment, blood was added to a tube containing sodium citrate 3.8% (dilution, 9:1). In order to prevent activation, 0.8 ml acid citrate dextrose (ACD) was added and gently mixed. Tubes were immediately centrifuged at 200 g for 20 min at 25°C (room temperature). After centrifugation, two-thirds of the upper PRP was separated slowly and dispensed into three microtubes.
Thereafter, 15μl of paraformaldehyde (PFA 1%) was added to microtubes as fixator and incubated for 10 min. Then, 5μl P-selectin (CD62P) antibodies conjugated by PE (PE anti-human CD62P, monoclonal BD Biosciences, CA, US) was added to the first and second microtubes, while, 5μl isotype control was added to the third microtube. Tubes volume increased to 1.5 mL by using Phosphate-Buffered Saline. All microtubes were placed on a shaker in dark condition and maintained at room temperature for 30 min. Flow cytometric analysis of 10,000 events in platelet area/sample was performed using a flow cytometer (BD FACSCalibur, US). A similar method was used for determining the PAC1 (activated GP IIb/IIIa complex), CD41a (platelet GPIIb/IIIa complex), and CD42b (glycoprotein Ib alpha, GPIbα). Blood lactate levels were also measured by using a lactometer (EKF Co. England).
Statistical analysis
Data were analyzed by using SPSS statistics for windows, version 22.0. Shapiro-Wilk test was used to determine the normality of data. For PLT, MPV, PDW, LAC, CD62P repeated measure analysis of variance (2×3) was used to compare the changes in response to two resistance exercise protocols. When ANOVA indicated the presence of a significant difference, Bonferroni’s post-hoc test was used to identify which mean differences were statistically significant. The significance level was set at P < 0.05.
Result
Both exercise trials produced a significant (P = 0.001) increase in blood lactate concentration with significant differences (P = 0.001) being observed between the two protocols (Table 2).
Mean (±SD) values of platelet indices, lactate and blood pressure
Mean (±SD) values of platelet indices, lactate and blood pressure
PLT, platelet count; PDW, platelet distribution width; MPV, mean platelet volume; LAC, lactate; BP, blood pressure. *Indicates a significant effect of exercise, and $ indicates a significant difference between TRE and CRE protocols.
Reductions in plasma volume were detected following both trials (11.5% and 12.1%, TRE vs CRE) with no significant differences being observed between the two protocols (P > 0.05). For this reason, although exercise-induced hemoconcentration occurred following both exercise trials, the platelet indices were not corrected for changes in plasma volume. Blood pressure increased significantly (P < 0.05) in response to resistance exercise and decreased to a level lower than baseline during recovery (post-exercise hypotension occurred). Increases in BP following CRE were higher than TRE trial (9.5% vs 7.7%), though, this difference did not reach the statistical significance level (Table 2).
A main significant effect of exercise (increases) were found for both PLT (F2,18 = 58.963, P = 0.001) and MPV (F2,18 = 15.390, P = 0.001), though, no significant interaction (session×time) was detected (Table 2). Data analyses revealed a main significant effect of resistance exercise for PAC1 (F2,18 = 131.780, P = 0.001), CD62P (F2,18 = 228.193, P = 0.001), CD42b (F2,18 = 24.377, P = 0.001), CD41a (F2,18 = 37.992, P = 0.001). PAC1 and CD62P increased significantly (P < 0.05), whereas, CD42b and CD41a reduced significantly (P < 0.05) following resistance exercise (Figs. 1–4). Changes in PAC1 (F2,18 = 23.368, P = 0.001), and CD62P (F2,18 = 8.012, P = 0.003) were significantly different between TRE and CRE protocols, with, increases being higher following CRE (Figs. 1, 2). However, changes in CD42b (P = 0.401) and CD41a (P = 0.922) were not related to the type of resistance exercise (P > 0.05).
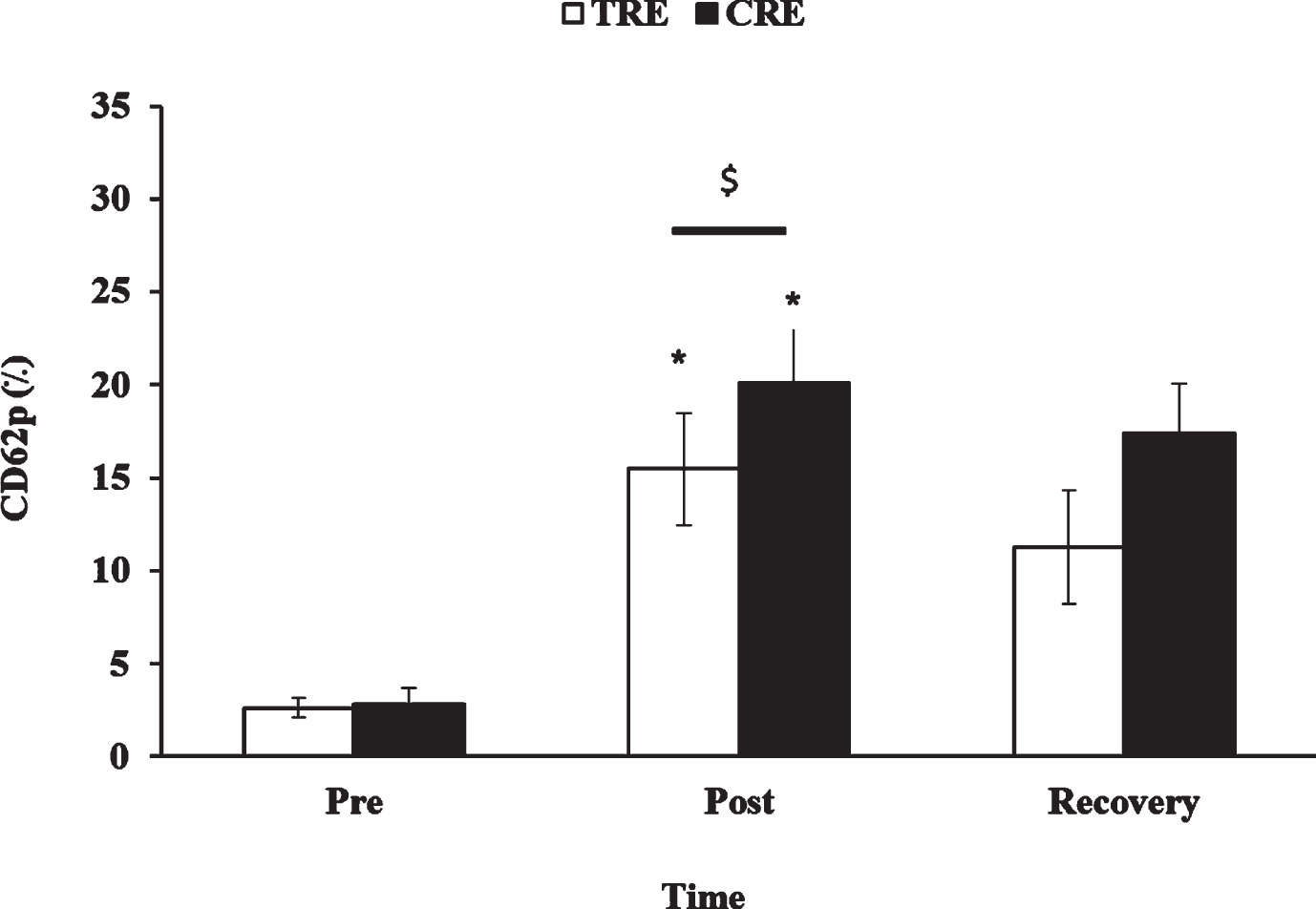
Mean (±SD) values for CD62p before exercise, immediately after exercise, and after recovery. *Indicates resistance exercise effect, and $ indicates the significant difference between the two protocols.
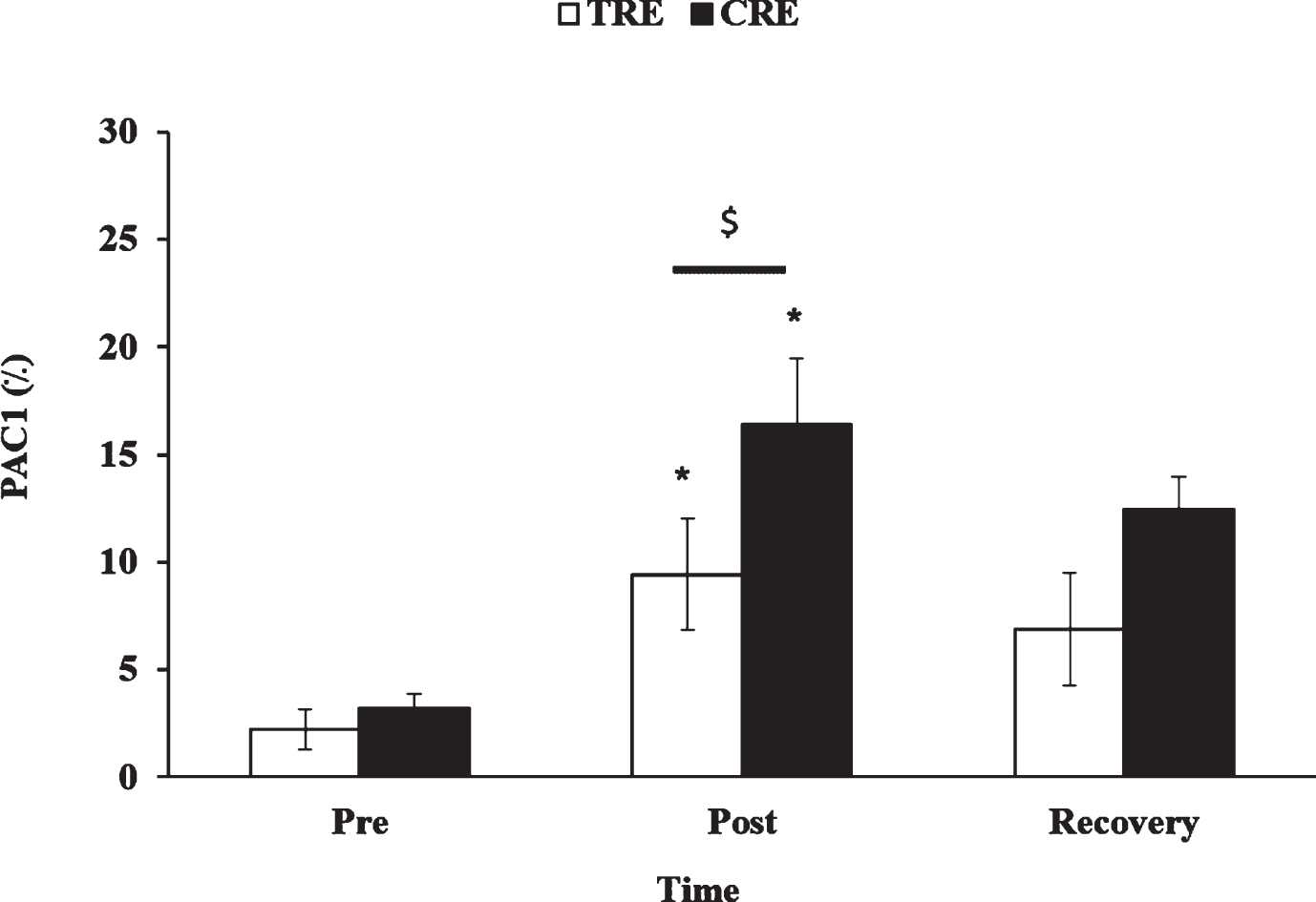
Mean (±SD) values for PAC1 before exercise, immediately after exercise, and after recovery. *Indicates resistance exercise effect, and $ indicates the significant difference between the two protocols.
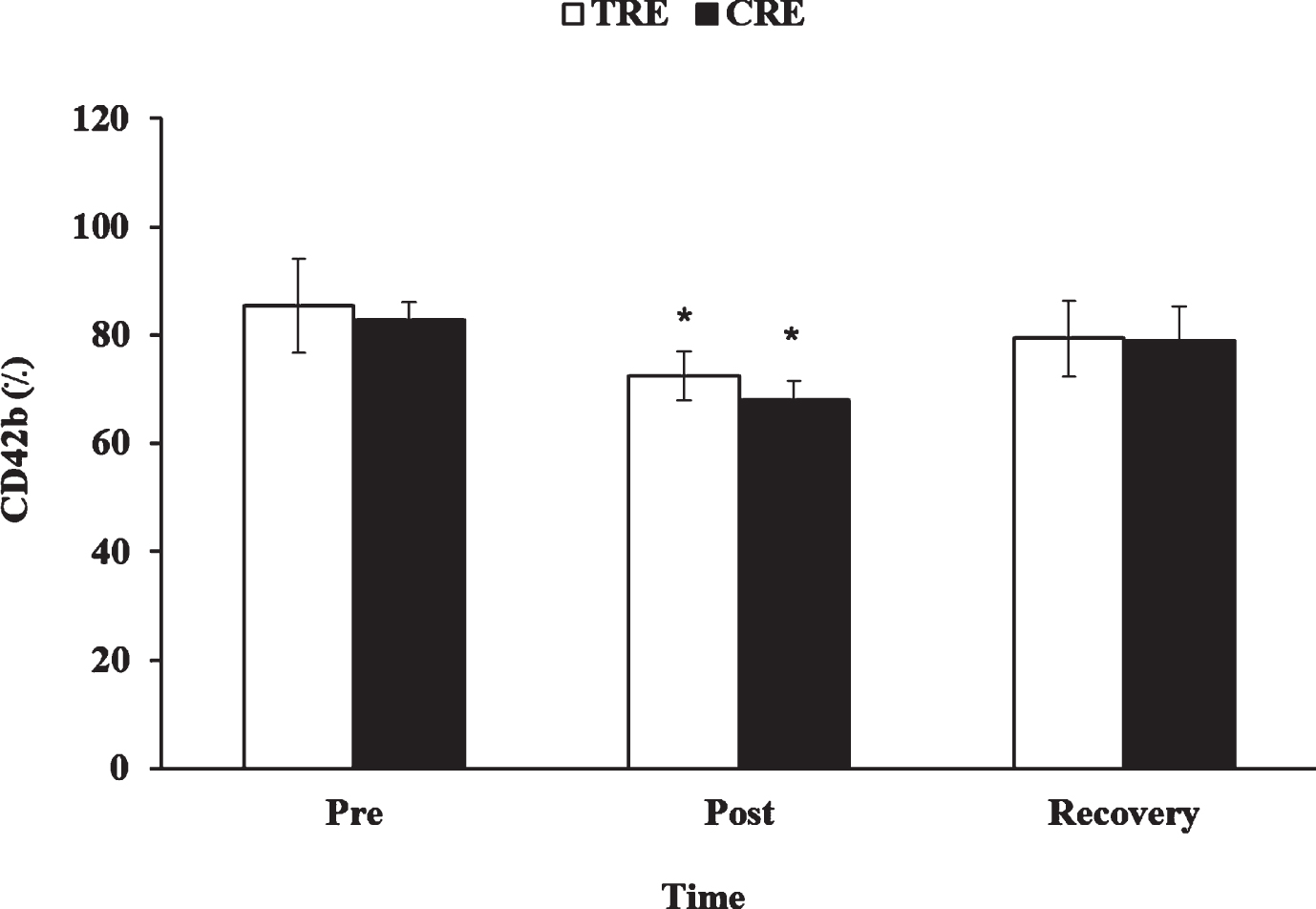
Mean (±SD) values for CD42b before exercise, immediately after exercise, and after recovery. *Indicates resistance exercise effect.
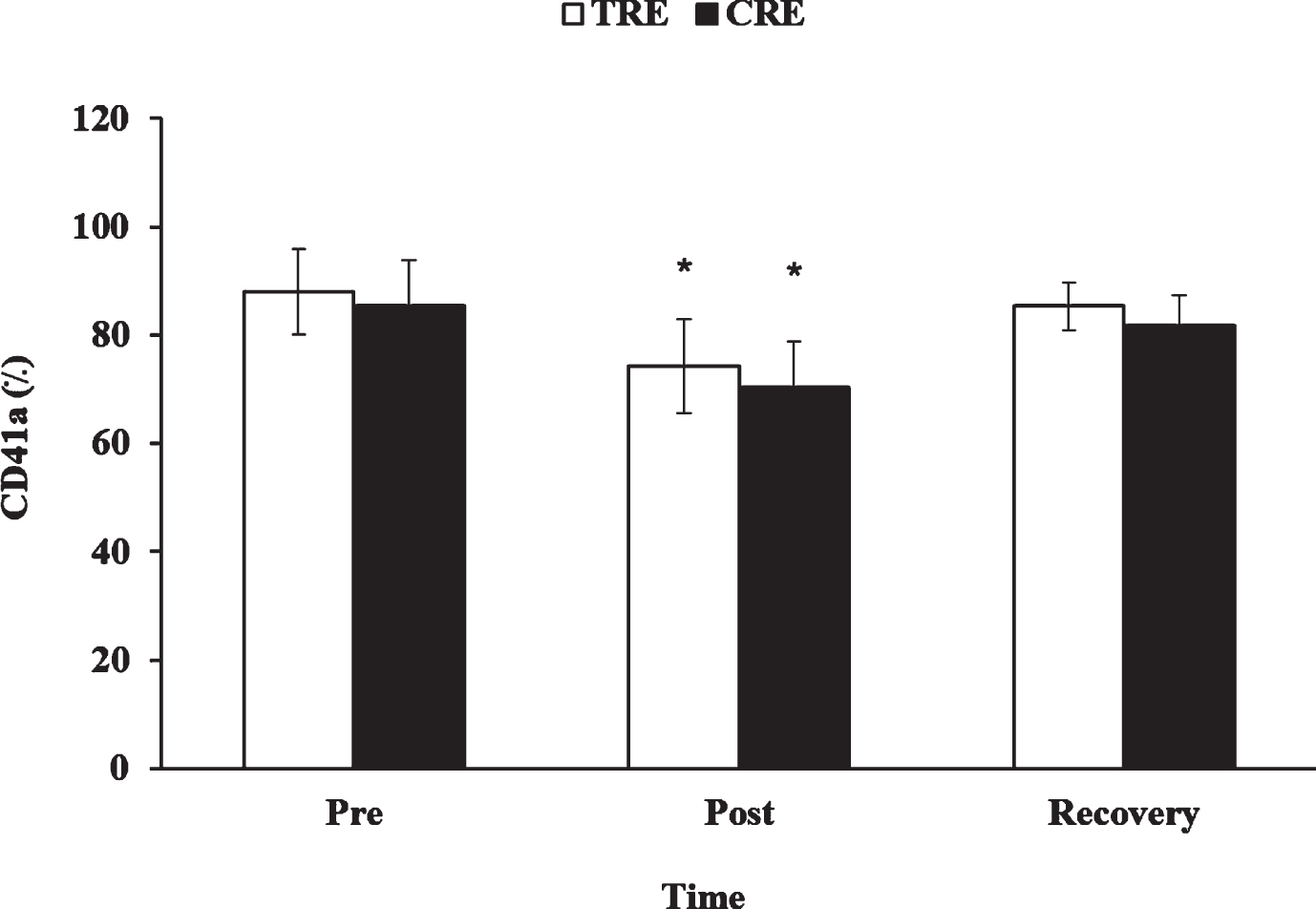
Mean (±SD) values for CD41a before exercise, immediately after exercise, and after recovery. *Indicates resistance exercise effect.

Immunofluorescence images for CD62P and PAC1 before exercise, immediately after exercise, and after recovery in two exercise trials.
Platelets play a pivotal role in blood hemostasis and their effects on health and vascular disease have been proven. There are some studies in the literature investigating the effects of acute resistance exercise on platelet indices (PLT, MPV, PCT, and PDW) and function (platelet aggregation) [1, 14]; however, no study has examined the effect of resistance exercise and its type on cellular markers of platelets including PAC1, P-selectin (CD62P), CD41a and CD42b. Therefore, the present study is the first study to address this by comparing the effects of traditional and CRE protocols.
We found a significant increase in PLT and MPV after both resistance exercise protocols. These findings are in agreement with our previous studies [1, 14] that confirmed transient increases in PLT following acute resistance exercise, which returned to the baseline after 30 to 60 min recovery. Increases in PLT have been attributed to the fresh release of platelets from the spleen, bone marrow, and lungs, and exercise-induced hemoconcentration [1]. In the present study plasma volume changes were 11.5% and 12.1% following traditional and CRE, respectively, which are in line with changes (9–14%) reported previously in response to different resistance exercise protocols [1, 34]. Since there was no significant difference between the plasma changes following the two trials data are not corrected for exercise-induced hemoconcentration. Since one of the main determinants of changes in PLT following exercise is exercise-induced hemoconcentration [1], the lack of differences between the two protocols for PLT and MPV might be attributed to similarity in plasma volume changes found following the two protocols.
Platelet production and clearance in physiological and pathological conditions is controlled in a complex and multifaceted mechanisms [35]. During exercise, several mechanisms, such as the release of epinephrine and decrease in the platelet NO content, cause platelet activation [8]. Platelet activation initiates the process of platelet clearance, which in pathological conditions is performed by macrophages [35]. Of course, platelet clearance and replacement in non-pathological conditions also occurs at the rate of 1011 platelets per day [35]. Platelet activation and increase in epinephrine, along with the removal of activated platelets from the blood circulation, caused fast release of platelets from their storage (bone marrow and spleen). During exercise, the higher rate of platelet activation than release and clearance has caused a significant increase in platelet activation index after exercise compared to baseline. However, with the cessation of exercise and decrease in platelet activation and increase in platelet clearance and replacement rate, the amount of activation index has decreased, though, in our data it did not reach the baseline levels. In addition, it should be noted that the release of platelets from platelet storage depends on exercise intensity, and the intensities used in our study appear sufficient to induce platelet release.
P-selectin (CD62P) is an important marker of platelet activation and a key adhesion molecule mediating cell-cell attachments of platelets to leukocytes [36]. By binding to its receptor on the leukocyte surface (PSGL-1) stimulates leukocytes and eventually inflammation [36]. In our study, both resistance exercise trials increased p-selectin, with higher increases (platelet activation) found after CRE. No previous study has investigated the effects of acute resistance exercise on P-selectin, and findings regarding the acute effects of endurance exercise are contradictory, depending on the exercise protocols [2]. However, the majority of previous studies have demonstrated increases in P-selectin following high intensity exercise [37, 38]. For example, Hilberg et al. (2008) demonstrated that platelet reactivity and platelet-leukocyte conjugate formation increase following exercise in an intensity-related manner [37]. Our findings support these because in the present study TRE was performed at 80% of 1-RM with 2 min rest, and CRE was performed at 65% of 1-RM with no rest following repetitions, therefore, both protocols could be considered as high intensity.
It has been proven that changes in CD62P are highly dependent on shear stress [39]; therefore, one of the main mechanisms that could be used to justify increases in CD62P in the present work is exercise-induced increases in shear stress. In addition, Boeno et al. (2019) have recently shown that moderate intensity resistance exercise induces a pattern of shear stress, stimulating the influx of endothelial calcium (Ca2 +) and activity of endothelial nitric oxide synthase (eNOS) [40].
During exercise, increases in cardiac output and blood flow to the exercising muscles elicit an increase in shear stress [41, 42], which, in turn, affects endothelial function [43]. On the other hand, high shear stress induces changes in the expression of platelet membrane glycoproteins such as PAC1, CD62P, GPIb/IX, and GPIIb/IIIa. Platelets are activated by high shear stress directly and independently, and the activation may be mediated by these glycoproteins.
In this study we found an increase in platelet activity (marked by increases in CD62P) was specifically associated with an increased platelet expression of PAC1 after exercise, suggesting that this change likely plays a major role in the exercise-induced increase in platelet function.
Platelet activation includes a series of cascade reactions that initiate with the binding of agonist to the receptor and cessation with platelet aggregation, and secretion. Platelet aggregation is the last step of GPIIb/IIIa complex (Integrin αIIb/βIII) activation and requires the expression of fibrinogen receptor on the platelet surface. Integrin αIIb/βIII is known as the common platelet receptor for fibrin and fibrinogen and plays a role in platelet aggregation. CD41a (GPIIb/IIIa complex), the most abundant platelet adhesive molecule, and CD42b (GPIbα) are known as a markers of platelet activation. The increase in exercise-induced shear stress causes a change in the expression of platelet membrane glycoproteins [44, 45].
In contrast to PAC1 and CD62P, CD41 and CD42b decreased in response to resistance exercise. These findings support those of Aurigemma et al. (2007) who showed increases and decreases in CD62P and CD41 following treadmill exercise stress test, respectively [46]. In spite of this, we expected similar changes in CD41 and CD62P because both CD41 and CD62P receptors are released by platelet alpha-granules [47]. The justifications for the different responses of CD41 and CD62P to exercise cannot be elucidated from our data, though, one possible explanation might be related to a different mechanism of platelets activation, where leukocytes–platelet aggregates might be seized from the circulating blood into the vessel wall, favored by an increased expression of adhesion molecules. However, previous studies have highlighted some other reasons to justify conflicting results including differences in participants’ characteristics (patients or normal) [8, 47].
In our study, we found that increases in CD62P and PAC1 were higher following CRE compared to TRE. This finding is expected because CRE might have resulted in more physiological stress because firstly, the subjects were untrained and 65% of 1-RM is still considered high intensity for this group [11], secondly, no rests were allowed between exercises in CRE that might lead to repeated episodic increases in shear stress [40, 48], and thirdly our findings proved that lactate concentration and blood pressure both were higher after CRE compared to TRE. Therefore, probably exercise-induced shear stress and activation of α2-adrenergic receptors in CRE protocol have been higher than TRE, because of continuous stress and activity that might mediate increases in platelet Ca2 + and α-granules exocytosis, which in turn results in translocation of P-selectin to the surface of platelets and activation of GPIIb/IIIa [37, 38].
Platelet activation is an ordered sequence of events that begins with the binding of an agonist to its receptor and ends with platelet shape change, aggregation, and secretion [8]. Platelet aggregation represents the final step of a complex activating sequence [49], and requires the expression of receptors for fibrinogen on the platelet surface [49] (platelet membrane glycoprotein (GP) IIb-IIIa, as the PAC1 specific antigen). In vitro, platelet activation was determined by fluorescent PAC1 binding and flow cytometry [50]. Exponential relationships were observed between PRP aggregation and platelet PAC1 expression, as percentage or relative fluorescence intensity [49]. For this reason, in this study, PAC1 was considered as evidence for platelet aggregation and no platelet aggregation test was performed.
Based on the findings of the present study the following conclusions can be drawn: (1) moderate to high intensity resistance exercise results in platelet activation and platelet hyper reactivity in sedentary individuals, (2) platelet activation following continuous moderate resistance exercise (circuit RE) is more pronounced than higher intensity resistance exercise with rest periods employed after each exercise, and (3) probably increases in shear stress following resistance exercise plays an important role in mediating changes in platelet activation and endothelial function in response to acute resistance, that warrants future studies.
Footnotes
Acknowledgments
The authors would like to thank all subjects for their enthusiastic participation in this investigation.