
Abstract
OBJECTIVE:
To investigate the clinical value of platelet and inflammatory factor activation in vascular endothelial injury in hypertension.
METHODS:
A total of 120 hypertension patients diagnosed in our hospital from December 2019 to June 2021 were enrolled as study objects (Hypertension group); besides, another cohort of 60 healthy people undergoing physical examination at the same period were recruited as the controls (Control group). Next, the baseline clinical characteristics of subjects in the two groups were recorded and compared. Specifically, a hematology analyzer was adopt for detecting the mean platelet volume (MPV), platelet distribution width (PDW) and platelet hematocrit (PCT); ELISA for the level of IL-6, IL-8 and TNF-α; PHILIPS EPIQ 7 C (a device assessing endothelial vasodilator function in a non-invasive fashion) for reactive hyperemia index (RHI); univariate and multivariate regression analysis for risk factors triggering endothelial dysfunction; and Spearman correlation analysis for the correlation of platelet activation indicators and inflammatory factor level with vascular endothelial function.
RESULTS:
Compared with the Control group, the patients in the Hypertension group exhibited higher levels of MPV, PDW, PCT, inflammatory factors (IL-6, IL-8 and TNF-α) and lower RHI. Moreover, Spearman correlation analysis showed a significant negative correlation of MPV, PDW, PCT, IL-6, IL-8 and TNF-α level with RHI level. In addition, univariate and multivariate regression analysis presented that MPV, PCT, IL-8 and TNF-α were risk factors for vascular endothelial dysfunction.
CONCLUSION:
The activation of platelet and inflammatory factor is closely related to vascular endothelial function injury in patients with hypertension. To be specifically, platelet and inflammatory factor activation can effectively reflect the vascular endothelial function injury in patients with hypertension and has high clinical value.
Keywords
Introduction
Hypertension is a multifactorial chronic non-communicable disease with complex mechanisms, affecting more than 1.2 billion individuals worldwide [1]. About 50% of deaths from cardiovascular and cerebrovascular diseases are closely related to hypertension, and hypertension is the main chronic risk factor leading to death of them [2]. Actually, hypertension-related complications have become a huge burden on global public health, and hypertension have become one of the important public health problems seriously threatening human health [3]. What’s more, hypertension is a common cause of renal failure, myocardial infarction, stroke, heart failure, and even death. Approximately 90–95% of hypertension belongs to essential hypertension, which has been considered as the result of a combination of genetic and environmental factors [4, 5]; however, the specific mechanism is not clear.
Studies have reported that vascular endothelial cell injury not only plays an important decisive role in the occurrence and development of hypertension but also is one of the basic pathological changes of hypertension; and the pathological processes of hypertension mainly include vascular endothelial injury, smooth muscle cell proliferation, vascular remodeling and inflammatory response, and so on [6–8]. Chemokines can promote the production of inflammatory factors. For example, the inflammatory factors like TNF-α, IL-1, IL-6, and IL-17 can induce vascular endothelial damage, thereby resulting in inflammatory cell accumulation and infiltration and endothelial tissue dysfunction; long-term poor prognosis may cause endothelial contraction and relaxation dysfunction, and then induces hypertension [9]. Additionally, platelet activation, prominent in hypertensive patients, can inhibit vascular injury repair and increase incidence of cardiovascular complications [10, 11]. Nevertheless, there are few relevant researches on the clinical value of platelet activation and inflammatory response in endothelial injury in hypertension. Therefore, the objective of this study was to investigate and analyze the clinical value of platelet activation inflammatory response indicator in the assessment of vascular endothelial function injury in hypertension.
Methods
Patient collection
This study enrolled 120 patients diagnosed with essential hypertension (Hypertension group) and 60 healthy individuals who underwent physical examination (Control group) in our hospital from June 2021 to June 2022. Inclusion criteria were shown as follows: All subjects (1) completed relevant examinations and were diagnosed with hypertension (systolic blood pressure higher than 140 mmHg, or diastolic blood pressure higher than 90 mmHg); (2) were older than 45 but younger than 85 years; (3) had no previous history of obvious food or drug allergy and no contraindications to the drugs in this study; (4) had euthymia, without cognitive impairment; (5) had no history of liver and kidney function damage, nervous system lesions, and no history of cardiovascular and cerebrovascular diseases. As for exclusion criteria, patients were excluded from this study if they (1) had secondary hypertension; (2) were diagnosed with myocardial infarction and heart failure; (3) suffered from combined trauma and infection; (4) received antihypertensive treatment before 30 days of treatment or suffered from malignant tumor disease; (5) had heart, liver, kidney and other dysfunction; (6) had cardiovascular and cerebrovascular diseases, hyperthyroidism and diabetes; (7) suffered from poor coagulation, psychiatric disorders, severe cognitive impairment, or language barriers; (8) had taken antiplatelet agents recently. All subjects received routine basic treatment, including weight control, control of the sodium intake in food, less intake of food rich in high fat and fatty acids, smoking cessation, alcohol avoidance, relieving mental stress. Besides, the patient was also given volume expansion, oxygen inhalation and other symptomatic treatments. Finally, the general information of patients was recorded. By the way, this study was approved by the Ethics Committee of Dongguan People’s Hospital (KYKT2022-036), and all patients signed the informed consent form.
Detection of platelet activation indicators
Firstly, all subjects were drawn 5 mL fasting peripheral venous blood. After standing at ambient temperature for 2 h, the blood was centrifuged at 3500 rpm for 10 min, followed by the collection of the supernatant. Next, by virtue of a hematology analyzer, the mean platelet volume (MPV), platelet distribution width (PDW) and platelet hematocrit (PCT) in the serum of subjects were measured, respectively.
Detection of inflammatory factors
A total of 5 mL fasting peripheral venous blood was collected form the subjects, and the serum was separated by centrifugation. Subsequently, blank wells, standard wells and sample wells were set in a 96-well plate; except the blank well, 100 uL standards and samples (duplicate wells) were added into the other two wells, respectively. After mixing well, the microtiter plate was covered, and the mixture was incubated at ambient temperature; after 2.5 h, the liquid was removed and 300 uL washing solution was added into each well; after washing 4 times, the washing solution was absorbed. Next, 100μL biotin-labeled antibody was added, shaken and mixed well; after another 1-h incubation at ambient temperature, the liquid was discarded, the above washing steps were repeated, and the plate was washed for four times then dried. Later, the prepared streptavidin solution was added into each well, shaken and mixed well, then incubated for 45 min; the liquid was absorbed, the above washing steps were repeated, and the plate was washed for 4 times then dried. Subsequently, 100 ul of tetramethylbenzidine (TMB) reagent solution was added into each well, shaken and mixed well, followed by the color development at ambient temperature in the dark. After 30 min, the stop buffer was added, and the above reaction was discontinued. Next, the 96-well plate was placed in a microplate reader, and the optical density (OD) of each well at 450 nm was measured. Finally, the levels of IL-6, IL-8, and TNF-α were calculated by plotting a standard curve based on the OD values of the standards.
Vascular endothelial function examination
Endothelial function was evaluated by reactive hyperemia index (RHI) using Endo-PAT2000 device (ITAMAR, Israel) [12]. In brief, all patients were measured in the early morning in a fasting state. After resting for at least 15 minutes, the hands were placed at heart level in all cases. A transducer attached to the Endo-PAT2000 device was mounted on the index finger of both hands, and the sphygmomanometer cuff was mounted on one arm for baseline measurements. Brachial artery flow was then blocked by inflating the cuff for 5 min. Finally, the vasodilatory response before and after flow block was assessed by changes in fingertip artery flow.
Statistical analysis
SPSS 25.0 was utilized for data treatment, measurement data were expressed as mean±standard deviation (SD), and enumeration data were expressed by n or %. In addition, t-test was adopted for comparison among multiple groups; and χ2 test for comparison between two groups. Spearman correlation analysis was performed to investigate the association of platelet activation parameters and inflammatory factor level with RHI levels; univariate and multivariate logistic regression analyses to predict risk factors of endothelial dysfunction in patients with hypertension. P < 0.05 was considered statistically significant.
Results
General information
Clinical baseline characteristics between the two groups were compared. Briefly speaking, there were no significant differences in age, gender, duration of hypertension, smoking history, alcoholism history, low-density lipoprotein, fasting blood glucose, creatinine, white blood cell count, neutrophil count, total protein and plasma albumin between the Hypertension and Control groups. Hence, there was a comparability between the two groups. Besides, patients in the Hypertension group had much higher body mass index (BMI), systolic blood pressure, diastolic blood pressure, total cholesterol, triglycerides, high-density lipoprotein and C-reactive protein (CRP) than those in the Control group (Table 1).
Clinical baseline characteristics of the patients in both groups
Clinical baseline characteristics of the patients in both groups
Platelet function indicators and inflammatory factor level between the two groups were further compared. Shortly speaking, the median levels of MPV, PDW and PCT and the overall fluctuation of the data in the Hypertension group were significantly higher than those in the Control group; the above outcome suggested a certain degree of correlation between the activation of platelets and the changes of blood pressure, i.e., the activation of platelets may be related to the increase of blood pressure (Fig. 1A–C). Moreover, compared with the Control group, Hypertension group exhibited obviously increased median level of inflammatory factors such as IL-6, IL-8 and TNF-α (p < 0.05), and differences were statistically significant. Besides, the overall level fluctuation of IL-6, IL-8 and TNF-α was also higher in the Hypertension group than in the Control group (Fig. 1D-E).

Comparison of platelet function indicators and inflammatory cytokines levels in the two groups. A–C, A hematology analyzer was adopted for assessing the mean platelet volume (MPV) (A), platelet distribution width (PDW) (B) and platelet hematocrit (PCT) (C); D–F, ELISA for the level of IL-6 (D), IL-6 (E), TNF-α (F) in patient plasma, **P < 0.01 vs. Control GROUP.
The comparison of vascular endothelial function indicators between the two groups were performed. The outcomes showed that the median value of RHI in patients of Hypertension group was much lower than that in the Control group (Fig. 2).
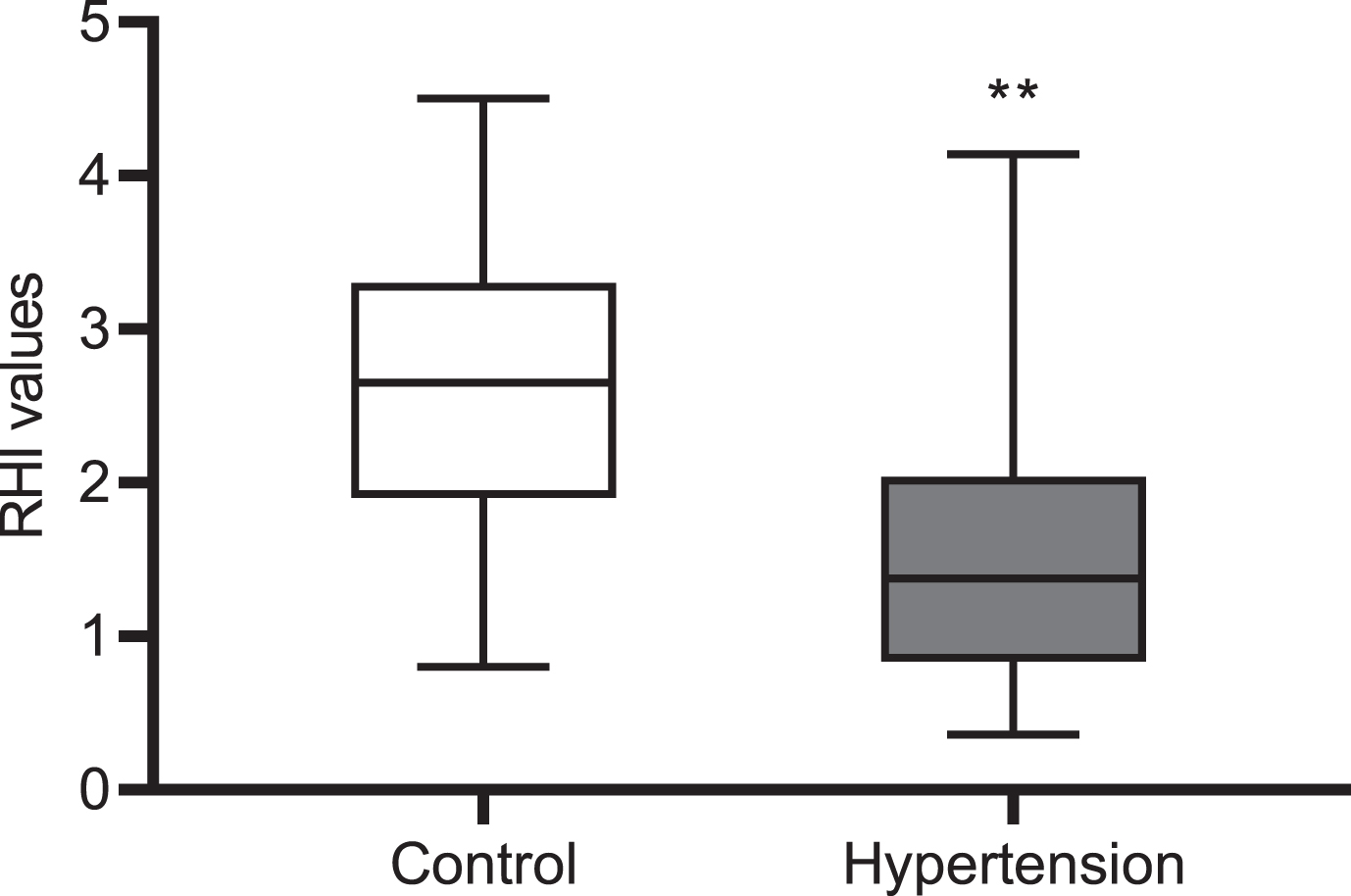
Comparison of vascular endothelial function indicators between the two groups. Endothelial function was evaluated by reactive hyperemia index (RHI) using Endo-PAT2000. **P < 0.01 vs. Control group.
Spearman correlation analysis was employed to investigate the correlation of platelet function indicators and inflammatory factor level with RHI. In brief, platelet function indicators MPV (r=–0.4381, p < 0.001), PDW (r=–0.2237, p = 0.014), and PCT (r=–0.3785, p < 0.001) were significantly negatively correlated with RHI to some extent (Fig. 3A–C). The above finding suggested that the activation of platelets may lead to further impairment of endothelial function, thereby further reducing RHI values. In addition, inflammatory factors IL-6 (r=–0.2199, p = 0.016), IL-8 (r=–0.4738, p < 0.001) and TNF-α (r=–0.3025, p < 0.01) were significantly negatively correlated with RHI to some extent (Fig. 3D–F).

Correlation analysis of platelet function indicators and inflammatory factors with reactive hyperemia index (RHI) in patients with hypertension. A–F, Spearman correlation analysis for the relationships of reactive hyperemia index with the mean platelet volume (A), platelet distribution width (B), platelet hematocrit (C), IL-6 (D), IL-8 (E) and TNF-α (F).
Univariate and multivariate logistic regression analyses were performed to investigate the effect of platelet activation indicators and inflammatory factors on endothelial dysfunction. The results of univariate logistic regression analysis suggested that, compared with normal patients, patients with elevated MPV (OR = 1.862, 95% CI: 1.168–3.625), PDW (OR = 1.385, 95% CI: 0.985–2.568), PCT (OR = 1.598, 95% CI: 1.105–3.044), IL-6 (OR = 1.245, 95% CI: 0.952–3.057), IL-8 (OR = 2.255, 95% CI: 1.205–4.362) and TNF-α (OR = 1.652, 95% CI: 1.158–3.582) had an increased risk of endothelial function injury, indicating that MPV, PDW, PCT, IL-6, IL-8, and TNF-α were risk factors for endothelial dysfunction. Furthermore, multivariate logistic regression analysis showed that there were significant differences in MPV, PCT, IL-8 and TNF-α (Table 2).
Univariate and multivariate Logistic regression analyses
Univariate and multivariate Logistic regression analyses
After vascular endothelial cell injury, many active substances will be released to destroy cell homeostasis. Upon the destruction of the cell homeostasis, the blood pressure is increased due to the decreased bioavailability of nitric oxide (NO) and the weakened synthesis of endothelin (ET) [13, 14]; moreover, the overexpression and accumulation of growth factors, adhesion molecules, and inflammatory factors can also change vascular structure and increase the risk of cardiovascular diseases, such as hypertension [15]. Although the etiology and pathogenesis of hypertension are not clear now, the role of platelet activation and inflammatory response in vascular endothelial injury in hypertension has gradually become a research hot spot. Relevant studies have shown that vascular endothelial cell injury in hypertension is closely associated with platelet and inflammatory factor activation [16–18]. Therefore, platelet activation and inflammatory response may become a breakthrough point in studying the pathogenesis of hypertension.
The stimulation and damage to the body can promote platelet activation, induce inflammatory response, and then encourage a variety of cardiovascular diseases [19, 20]. A study by Wang et al. [21] pointed out that sepsis could promote the activation of platelets, result in endothelial cell injury, promote extracellular traps and microthrombosis of neutrophils, exacerbate septic coagulation and inflammatory response, induce the occurrence or aggravation of disseminated intravascular coagulation (DIC), and then cause organ damage. Studies by Gkaliagkousi et al. [22] claimed that patients with hypertension were accompanied by platelet activation and dysfunction in vivo. Larrousse et al. [23] also stated that activated platelets played an important role in the occurrence and development of salt-sensitive hypertension. However, the specific molecular mechanism of platelets still needs further exploration. In this study, the indicators of platelet activation in the Hypertension group included obviously increased MPV, PDW and PCT level. Besides, Spearman correlation analysis revealed a negative correlation of the level of MPV, PDW and PCT with RHI. Moreover, univariate logistic regression analysis indicated that MPV, PDW, and PCT were risk factors of endothelial dysfunction; multivariate logistic regression analysis showed that MPV and PCT were risk factors of endothelial dysfunction. The outcomes of logistic regression analyses suggested that abnormal activation of platelet indicators was closely correlated with vascular endothelial function injury in patients with hypertension. A series of findings of the above further verified that high level of platelet activation can aggravate endothelial injury, results in decreased vascular endothelial function and vasodilator dysfunction, thereby bringing about a progressive increase in blood pressure in patients.
CRP is an acute reactive protein secreted by the liver [24], which can regulate inflammation and counteract protease in the inflammatory response. Related reports [25] have claimed that CRP can increase the number of vascular endothelial cells, thicken endarterium, and induce atherosclerosis. Alizadeh Dehnavi et al. [26] evaluated the inflammatory response in 439 male visceral obese patients with type 2 diabetes and cardiovascular disease. Specifically, in the common carotid artery and common carotid duct, increased maximum wall thickness was significantly associated with elevated CRP level. In this paper, CRP changes in Hypertension and Control groups were compared and analyzed by t-test, and statistically significant differences could be observed between the two groups. This paper further suggested that elevated CRP was closely associated with arterial wall thickening, and specifically, increased CRP decreased elasticity of arterial wall, and then resulted in a progressive increase in blood pressure.
TNF-α, derived from activated mononuclear macrophages, can promote the activation and aggregation of white blood cell at the inflammatory site, accelerate the release of platelet factors, induce the production and release of IL-6 and IL-8 by fibroblasts and monocytes, damage to vascular endothelial cells, promote smooth muscle cell proliferation, encourage white blood cell extravasation and adhesion, and ultimately lead to increased vascular resistance and blood pressure [27]. In this paper, Spearman correlation analysis results exhibited that CRP, IL-6, IL-8 and TNF-α level was notably increased in Hypertension group; and IL-6, IL-8 and TNF-α levels were negatively associated with RHI. The findings of Spearman correlation analysis indicated that the higher the level of inflammatory factors, the worse the vascular endothelial function in hypertensive patients. Sun et al. [28] revealed that in patients with diabetic nephropathy, inflammatory factor level was closely related to vascular endothelial function; and the occurrence and deterioration of atherosclerosis caused by inflammatory response was also an important factor leading to death in patients with diabetic nephropathy. In addition, logistic regression analysis was performed to analyze the correlation of IL-6, IL-8 and TNF-α with endothelial dysfunction in this study. On the one hand, the univariate analysis showed that IL-6, IL-8, and TNF-α were the risk factors for endothelial dysfunction; on the other hand, the multivariate analysis indicated that IL-8, TNF-α were risk factors for endothelial dysfunction. In short, the outcomes of logistic regression analysis in this paper suggested a close link between abnormal expression of inflammatory factors and vascular endothelial function impairment in patients with hypertension.
There are some shortcomings in this study. First, endothelial impairment is also associated with other factors such as microcirculatory disorders, so more parameters need to be set in the study; in addition, only indirect parameters of platelet activation were measured, and more direct activation indicators (e.g., CD61, CD62P, CD63) need to be further assessed.
Conclusion
In summary, platelet activation and inflammatory response are closely related to vascular endothelial function impairment in patients with hypertension. The combined detection of the above two indicators has high clinical value for the prediction and diagnosis of vascular endothelial function injury in patients with hypertension.
Declaration of interest
The authors declare no conflict of interest.
Authors’ contributions
Zheng-wei Jian and Guan-shen Huang designed the study. Zheng-wei Jian and Xiao-ming Zhang analysed the data. Xiao-ming Zhang and Guan-shen Huang wrote the manuscript.