
Abstract
OBJECTIVE:
Our research sought to investigate the relationship between initial ablation ratio (IAR) and internal composition of benign thyroid nodules treated by microwave ablation (MWA).
MATERIALS AND METHODS:
Patients who underwent MWA at the Affiliated Hospital of Jiangsu University from January 2018 to December 2022 were enrolled in our research. All the patients were followed up for at least one year. We analyzed the relationship between IAR at 1 month of solid nodules (solid >90%), predominantly solid nodules (90% >solid > 75%), mixed solid alongside cystic nodules (75% >solid > 50%) as well as volume reduction rate (VRR) at 1, 3, 6 and 12 months follow-up.
OBJECTIVE:
The mean IAR of the solid nodules (solid >90%) was 94.32±7.87%,#x0025;, that of the predominantly solid nodules (90% >solid > 75%) and mixed solid alongside cystic nodules (75% >solid > 50%) were 86.51±6.66% and 75.19±4.97%,#x0025;, respectively. Almost all the thyroid nodules were significantly decreased in size after MWA. After 12 months of MWA treatment, the average volume of the aforementioned thyroid nodules decreased from 8.69±8.79 to 1.84±3.11 ml, 10.94±9.07 to 2.58±3.34 ml, 9.92±6.27 to 0.25±0.42 ml, respectively. The mean symptom and cosmetic scores of the nodules showed significant (p < 0.000) improvement. The rates of the complications or side effects of MWA against the above-mentioned nodule types were 8.3% (3/36), 3.2% (1/31) and 0% (0/36), respectively.
CONCLUSIONS:
The application of the IAR to quantify the success rate of thyroid nodule microwaves in the short term demonstrated that IAR was related to the internal components of the nodule. Although the IAR was not high when the thyroid component was mixed solid and cystic nodules (75% >solid > 50%), the final therapeutic effect was still satisfactory.
Keywords
Introduction
Thyroid nodule is a common disease in the global [1, 2]. With the development of imaging technology, the detection rate of thyroid nodules is also increasing and has even reached 70% due to the high-frequency ultrasound as the diagnosing tool [3–6]. Although most thyroid nodules are benign, some signs, such as symptoms of partial compression, can cause cosmetic problems [3, 7]. Conventional wisdom holds that surgery is the preferred treatment for benign thyroid nodules. During recent years, ultrasound (US)-guided thermal ablation (TA) technology (including radio frequency, microwave, laser, etc.) have been recommended by several guidelines as alternative methods to surgery for benign thyroid nodules, with the features of less trauma, rapid recovery, repeatability, beautiful features, better preservation of thyroid function and improvement of life quality [8–11].
Microwave ablation (MWA) is a novel type of local TA technology, which exhibits characteristics including fast heating, strong coagulation capacity and large ablation area, and has become a satisfactory alternative option for thyroid nodules [3]. To our acknowledge, there is paucity of data as extensive literature and patent search showed only two articles on the IAR of thyroid nodules. There was one study on the quantitative analysis of the success rate of ablation via IAR, while the other work investigated the recurrence of nodules after ablation with IAR as the form of measuring the success of treatment [12, 13].
The purpose of this study was to evaluate the effectiveness of the IAR in the MWA of thyroid benign nodules, as well as investigate whether the IAR of thyroid benign nodules of different components also showed differences after the MWA.
Materials and methods
Patients
Our research was conducted according to Declaration of Helsinki and approved by approved by the Ethics Committee of the Affiliated Hospital of Jiangsu University (SWYXLL20190225–2). Written informed consent was obtained from each of the patients before MWA, and the patients’ identities were protected. All the patients in the study signed informed consent. A retrospective design of study was employed for this study. We selected a total of 88 patients who were treated with percutaneous MWA from January 2019 to December 2022, and these enrolled patients were closely followed up for one year. The inclusion criteria were as follows: (1) nodular diameter of >2 cm with a progressive growth trend; (2) patients with symptomatic or cosmetic problems; (3) benign pathological results from two independent US-guided fine-needle aspiration (FNA) [14]. (4) no other neck treatment; (5) reluctance to undergo surgery for cosmetic or psychological reasons; (6) follow-up for one year or more and (7) normal serum thyroid function. The exclusion criteria were included: (1) severe coagulation dysfunction; (2) dysfunction of multiple organs; (3) predominantly cystic nodules (solid components <50%).
US and ablation equipment
The ultrasonic diagnosis of thyroid nodules was performed with Mylab Twice (Italy, Esaote) color Doppler US diagnostic instrument (LA523-type high frequency linear array, frequency range: 4–13 MHz) before ablation and during each follow-up. The MWA therapy instrument used in this study was the KY-2000 2450 MHz microwave system (Kangyou Medical, Nanjing, China) with the output power set at 35 W. A 16G (KY-2450A-1 type), Teflon-coated, internal-cooled microwave antenna with a 3-mm active tip at 28–32°C temperature stability and a 10 cm shaft length was applied in our research, which was specifically modified for the ablation of thyroid nodules [15]. In order to prevent the shaft from overheating and cause skin damage, a squirming pump was applied to circulate the cooled saline through a double channel in the shaft.
Pre-ablative assessment
Symptomatic and cosmetic problems
The symptomatic scores in patients with nodules could be self-measured using a scale of 0–10 points. The cosmetic scores were evaluated by an experienced physician and ranged from 1 to 4: (1) no palpable mass; (2) palpable mass but no cosmetic problems; (3) cosmetic problem on swallowing only or detected by an experienced physician; and (4) a readily detected cosmetic problem [16].
Pathological examination
The nodules of all the patients underwent at least two separate fine-needle biopsies prior to MWA to confirm that the nodules were benign. If necessary, a coarse needle biopsy is acceptable.
Ultrasonic examination
Ultrasound examination plays a key role in describing the target nodule location, size, echogenic features and relationship between the nodules and the important surrounding structures. At the same time, experienced ultrasound doctors graded the CDFI status of nodules: (1) no color signal in the nodule; (2) color signals in <25% of the nodule; (3) color signals in 25–50% of the nodule and (4) color signals in >50% of the nodule [17]. The maximum diameter of each nodule was recorded (a) while the other two orthogonal diameters were determined (b and c). The volume of the nodule was calculated using the formula: V = πabc/6 and will be recorded as V0.
Laboratory examination
Laboratory examinations included whole blood tests, blood coagulation tests, fT3, fT4, TSH and serum calcitonin.
Procedure
The patient was placed in a supine position with the neck fully exposed, and a small pillow was placed on the neck to relieve the discomfort that may occur during the ablation process. After conventional disinfection, towel spread and 2% lidocaine local anesthesia coupled with normal saline isolation was used to protect the surrounding important tissues and organs for ablation. When the nodule had cystic portion, we aspirated the fluid first as much as possible, and then MWA was performed for the remaining solid portion [13, 18]. Moving-shot technique was applied to ablate the target nodules, while simple communication was performed on the patients during the ablation process to ensure that the recurrent laryngeal nerve was not damaged. More importantly, our entire operation was carried out in real time under US. After ablation, a small ice bag was necessarily used to cover the front part of the patient’s neck for at least 30 min of observation. Each patient was hospitalized for one night to ensure no early complications occurred.
Post-ablation evaluations and subsequent follow-up
After MWA, the patients should be returned to the hospital for thyroid US examination, namely the size of ablation area, internal echo, blood flow and contrast-enhanced US at 1, 3, 6 and 12 months, respectively. At the same time, symptom and cosmetic scores should be reviewed at each follow-up. The volume of each follow-up was calculated as Vt, V a , V3, V6 and V12, appropriately.
The volume reduction was calculated as follows: volume reduction ratio (VRR)% = ([initial volume–final volume]×100)/initial volume. Treatment was considered an effective definition of VRR >50%.
The IAR was calculated as: IAR = Va/Vt, where Vt was defined as the total nodule volume, Va was defined as an ablated nodule volume that presents as the unperfused area i.e. the area that is not active with contrast-enhanced US at the first follow-up. For instance, if the Vt is 10 mL and the Va is 6 mL, the ablation ratio is calculated to be 60%. However, the IAR was measured only at the first follow-up (1 month after ablation).
Statistical analysis
Data analysis was performed with SPSS statistical software, version 25.0 (SPSS Inc. Chicago, IL, USA). Values for quantitative variables were expressed as the mean±SD. Between these three groups, the Fisher’s Exact Test was used to analysis the data on gender while the paired-samples t-test was performed to compare, the age, the maximal diameter, the volume, the symptomatic and cosmetic scores as well as the vascular score and the ablation time before the MWA. In the completely solid nodules (solid >90%), predominantly solid nodules (90% >solid > 75%) or mixed solid and cystic nodules (75% >solid > 50%) group, one-way ANOVA was applied to compare the nodular symptomatic and cosmetic scores, maximal diameter and volume as well as VRR at each follow-up. The Chi-square test was applied to the number of patients in achieving therapeutic success between the three groups. A P-value less or equal 0.05 (P≤0.05) was considered statistically significant.
Results
A total of 88 patients (15 males and 73 females) with 103 nodules were enrolled in this study. The clinical features of the benign thyroid nodules in the three groups before treatment are listed in Table 1.
Summary of patients’ demographic data and nodules
Summary of patients’ demographic data and nodules
PS: Values are presented as the mean±SD (range). BTNs: benign thyroid nodules, M/F: male/female, Pts.: patients, cm: centimeter, ml: milliliter.
In the completely solid nodules (solid >90%) group, the mean volume of the ablated nodules at the 1st, 3rd, 6th and 12th month were 8.40±7.48 ml, 5.12±5.31 ml, 3.11±4.17 ml, and 1.84±3.11 ml (P = 0.000, Table 2), respectively, wherein all of them were significantly less than that before the ablation. The VRRs were also calculated, and the reduction of volumes after the MWA at the 1st, 3rd, 6th and 12th month were 14.03±13.29%,#x0025;, 36.75±10.81%,#x0025;, 58.94±18.08%,#x0025;, 75.89±16.73% (P = 0.000, Table 2), respectively. In addition, the symptomatic and cosmetic scores were significantly improved after MWA, from 1.56±1.83 to 0.89±1.19 and 2.11±0.92 to 1.67±0.72, respectively (P = 0.000, Table 2). In this group, the treatment of two patients were unsuccessful. In one case, the calculated IAR was 85.71%,#x0025;, while the VRR was computed to be only 39.51% at 12 months follow-up. In another case, the IAR was calculated to be 87.22%,#x0025;, and the computation of VRR was only 33.93% at 12 months follow-up.
Outcomes for thyroid nodules after MWA ablation(intro-observer)
PS: cm: centimeter, ml: milliliter, IAR: initial ablation ratio, VRR: volume reduction ratio.
In the predominantly solid nodules (90% >solid > 75%) group, the mean volume of the ablated nodules at the 1st, 3rd, 6th and 12th month were 9.23±9.11 ml, 6.53±6.46 ml, 4.04±4.70 ml, and 2.58±3.34 ml (P = 0.000, Table 2), respectively. The corresponding VRRs after the MWA at the 1st, 3rd, 6th and 12th month were 20.66±16.55%,#x0025;, 43.99±11.42%,#x0025;, 67.64±14.26%,#x0025;, 80.62±15.39%,#x0025;, respectively (P = 0.000, Table 2). Noticeably, the symptomatic and cosmetic scores were substantially improved after MWA, from 2.19±1.70 to 0.97±0.98 and 2.16±0.90 to 1.65±0.71, respectively (P = 0.000, Table 2). In this group, one patient was unsuccessfully treated, while the estimated IAR was 89.47%,#x0025;, and the computed VRR was only 38.39% at 12 months follow-up.
In the mixed solid and cystic nodules (75% >solid > 50%) group, the mean volume of the ablated nodules at the 1st, 3rd, 6th and 12th month were 8.77±5.88 ml, 3.47±2.46 ml, 1.23±1.21 ml and 0.25±0.24 ml (P = 0.000, Table 2), respectively. The corresponding VRRs after the MWA at the 1st, 3rd, 6th and 12th month were 11.35±17.22%,#x0025;, 63.63±11.49%,#x0025;, 87.08±8.84%,#x0025;, 97.89±2.66% (P = 0.000, Table 2). Likewise, the symptomatic and cosmetic scores were significantly improved after MWA, from 2.19±1.70 to 0.97±0.98 and 2.16±0.90 to 1.65±0.71, respectively (P = 0.000, Table 2). Most importantly, all the patients in this group were treated successfully.
Figure 1 reflects the positive correlation between VRR and time during the follow-up of the three groups. Of course, each nodule is completely ablated, so the absorption rate was high. However, the VRR of the mixed solid and cystic nodules group in the three groups was the best. Figures 2 and 3 show that the therapeutic success rates at the 3-month follow-up were 5.55% (2/36), 32.25% (10/31), 83.33% (30/36), and at the 6-month follow-up were 61.11% (22/36), 87.09% (27/31) and 100% (36/36), respectively. In other words, it could be seen from the three and six months follow-up after MWA that the components in the nodules are closely related to the therapeutic success rate.

Reflects the positive correlation between VRR and time during the follow-up of the three groups.
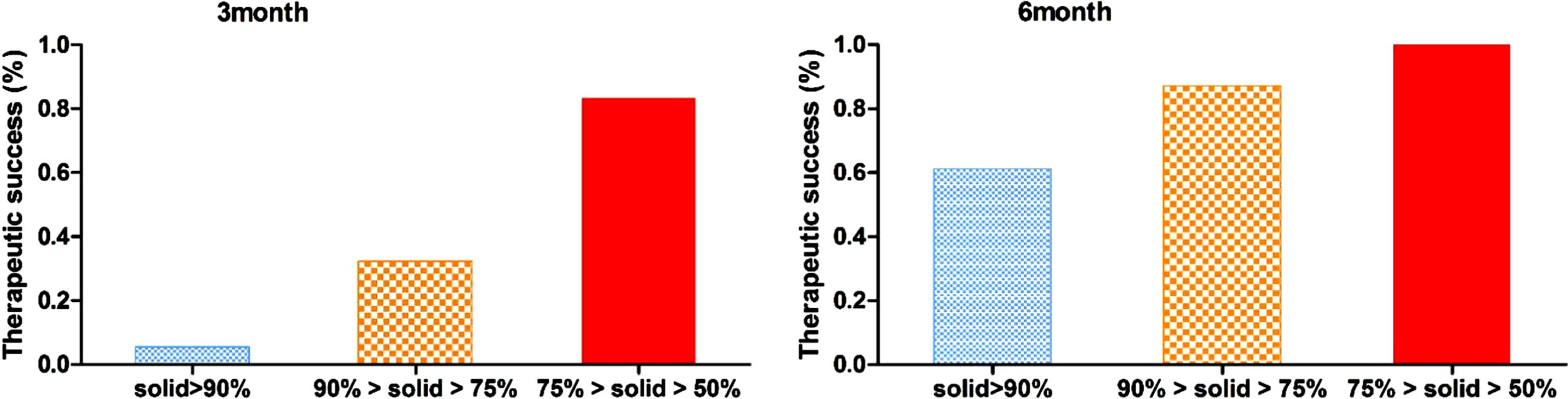
Shows the therapeutic success rates at the 3-month and at the 6-month follow-up.
Table 3 depicts the relationship between the VRR at the final follow-up and the IAR in the three groups. The IAR was calculated to be 94.32±7.87% in the completely solid group, 86.51±6.66% in the predominantly solid group, and 75.19±4.97% in the mixed solid and cystic group. The inter-observer of IAR was reflected in Fig. 4.
IAR and Nodule volume changes according to the follow-up periods(inter-observer)
The complications and side effects are summarized in Table 4. The overall complication rate was 4.5% (4/88), while the complication rate was 10.7% (3/28) in the completely solid nodules group and 3.6% (1/28) in the predominantly solid nodules group, but no complications occurred in the mixed solid and cystic nodules group. Noticeably, all the complications recovered spontaneously after a few months without any medication. At the same time, there were no delayed complications during the follow-up.
Complications or side effects
With the transformation of medical models and the development of medical technology in recent years, patients not only have the desire to cure tumors, but also hope to maintain the aesthetics of the neck as much as possible after surgery, and the treatment of thyroid nodules has been gradually development in the direction of minimally invasive [19–21].
Ethanol ablation (EA) is the earliest minimally invasive interventional therapy for the treatment of benign thyroid nodules. The principle is to cause coagulative necrosis of the thyroid tissue and thrombosis of small blood vessels. This method is effective for cystic thyroid nodules, but not solid or solid thyroid nodules, mainly due to the uneven dispersion of ethanol in solid nodules or local alcohol loss due to abundant blood flow in the nodules, resulting in incomplete ablation. With the development of ablation therapy in recent years, local TA techniques such as radiofrequency ablation (RFA), laser ablation (LA), and MWA have been gradually applied to clinically treat benign thyroid nodules, which have achieved good results [22]. Compared with the RFA and LA, MWA produces higher energy, and has a wide range of ablation, shorter treatment time and more complete tumor inactivation. It is more advantageous in treating large volume thyroid nodules. Jeong et al. [23] first used the VRR to estimate the change in nodule volume after ablation. Feng et al. [16] reported that the VRR of thyroid nodules after MWA for one year was about 45.9%. Besides, Yue et al. [24] performed MWA for 222 patients with thyroid nodules, wherein the volume of ablation lesions at 6th postoperative month and the volume of nodules before ablation were compared. The results showed that 82.3% of the nodule VRR exceeded 50%,#x0025;, and 30.7% of the nodules that disappeared at the 6th month after the operation. It could be seen that the VRR is an effective long-term evaluation index for thyroid nodules MWA therapy, rather than a short-term efficacy evaluation index. Jung’s study proposed to use the IAR index to assess the short-term efficacy of microwave ablation of benign thyroid nodules, thereby quantifying the success rate of the treatment. However, his research was based solely on the size of the nodules and color Doppler US techniques, which will lead to limitations in the result of the IAR.

Reflects the inter-observer of IAR.
Elastography is the most noteworthy of the new technologies in recent diagnostic US systems and able to reveal the differences in the elastic properties of soft tissues [25, 26]. Szintigraphy of the thyroid gland is still one of the most important preoperative diagnostic procedures [27]. Contrast-enhanced ultrasonography (CEUS) is a potential tool to investigate the microvascular flow of different tissues/organs, which displays the microvascularity of cancer tissue and achieves better temporal and spatial resolution [1, 28]. The present work was based on the composition of thyroid benign nodules and the use of CEUS to complement the IAR study. Noticeably, the composition of the nodules are divided into three groups, viz., completely solid nodules (solid >90%), predominantly solid nodules (90% >solid > 75%), and mixed solid and cystic nodules (75% >solid > 50%). Both color Doppler US and CEUS techniques could observe the damage of blood perfusion in the ablation zone as well as the perfusion of new blood flow after operation. However, compared with color Doppler US, the CEUS provides a more accurate and intuitive US image that accurately reflects the difference in blood perfusion between the ablation zone and surrounding glandular tissues. Other studies have reported that CEUS can accurately determine the ablation zone and identify the areas of residual incomplete ablation. Thus, the clear display of perfusion of CEUS prevents the patient’s secondary treatment because of incomplete ablation, which does not only reduce the pain of re-operation, but also avoids the risk of various complications caused by re-treatment. Therefore, we applied CEUS to measure the size of Va, which in turn reduced the error of the IAR.
Despite the results obtained, there are some limitations of this study. Firstly, this is a retrospective analysis. Secondly, the sample size is small and the follow-up time is short. Thirdly, inability to establish whether the reperfusion image on the CEUS is related to the IAR. In future studies, we aim to establish prospective studies with an increase sample size and a longer follow-up.
Our current study has demonstrated a negative correlation between the IAR and the final VRR (P < 0.001), although this result is based on the proportion of solid components in the nodule. The higher the ratio of solid components, the higher the IAR, but the lower the VRR. The final VRR was 75.87±16.73% in the completely solid group, 80.62±15.39% in the predominantly solid group, and 97.89±2.66% in the mixed solid and cystic group. Besides, we could apply the IAR index to predict the long-term efficacy on the MWA of nodules based on the proportion of the solid components, and to determine whether secondary ablation is needed in the short-term.
Conflict of interest
The authors report no conflict of interest.
Footnotes
Acknowledgments
This work was supported by the Sixth Phase “169 Project” Scientific Research Project of Zhenjiang City (Grant No. YLJ202104), the Social Development Program of Zhenjiang City (Grant No. SH2022066), and Medical Education Collaborative Innovation Fund of Jiangsu University (Grant No. JDY2022002).