
Abstract
INTRODUCTION:
It is rare for intraductal papilloma (IDP), a benign papillary tumor, to occur in the sublingual gland (SLG).
CASE SUMMARY:
A 55-year-old man incidentally found a painless mass in his left submandibular region (SMR). He had a history of two surgeries for bilateral SLG cyst. Contrast enhanced ultrasound (CEUS) and magnetic resonance imaging (MRI) were performed. The patient received trans-cervical excision of left residual SLG in combination with excision of left submandibular gland (SMG). The postoperative course was uneventful and no signs of recurrence during 5 months of follow-up.
DISCUSSION:
For a SMR mass, extraoral type of IDP in SLG should be considered in the differential diagnosis.
Introduction
The World Health Organization (WHO) in 2017 recognized 11 different benign epithelial salivary gland tumors [1]. Intraductal papilloma (IDP) of the sublingual gland (SLG) is a rare histological subtype. There are no previous reports of extraoral type of IDP in SLG and with a history of two surgeries for bilateral SLG cyst. Herein, we presented a case of extraoral type of IDP in SLG mimic other salivary lesions in a 55-year-old male.
Informed consent of the patient and the approval from the institutional ethical committee (NO. 20220304) have been obtained for this report. We present the following case in accordance with the CARE reporting checklist.
Case report
A 55-year-old man incidentally found a painless mass in his left submandibular region (SMR) in October 2021. Since then, the mass appeared to increase in size for 1 month. On physical examination, a mobile mass measuring about 3.5×5 cm was palpable in the left SMR. He was admitted to hospital with a symptom of discomfort in the neck. He reported no family history of salivary cancer and no respiratory distress. The contrast enhanced ultrasound (CEUS) showed a cystic solid mass in the left SMR, the solid component was hyper-enhanced and the cystic component was non-enhanced (Fig. 1). The left submandibular gland (SMG) was normal. Magnetic resonance imaging (MRI) revealed a distinct T2-high intensity area localized in SMR, which was measured 3.4×6.4×5.7 cm, a 2 cm nodule with T2-low intensity inside the mass (Fig. 1). Subsequently, trans-cervical excision of left residual SLG in combination with excision of left SMG was performed. The mass was from residual SLG under the oral floor muscle intra-operation. The pathologic diagnosis was IDP of the SLG (Fig. 1). The postoperative course was uneventful and no signs of recurrence during 5 months of follow-up.
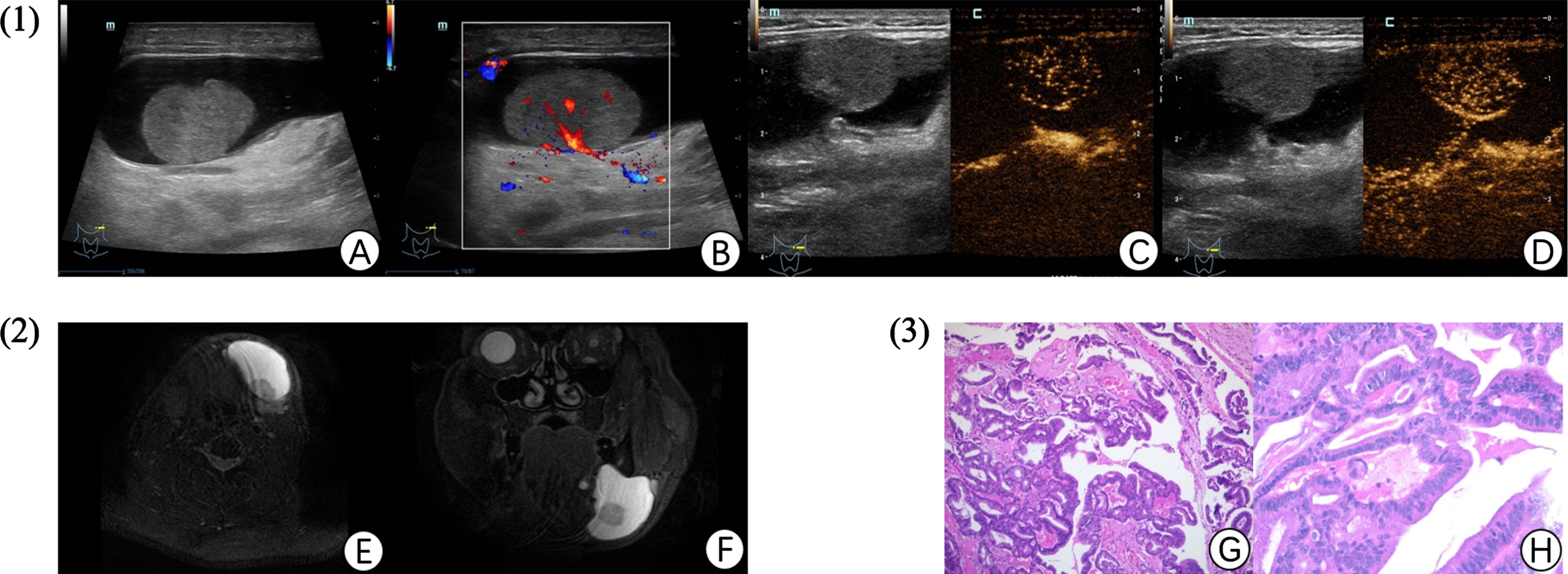
Contrast enhanced ultrasound (CEUS), magnetic resonance imaging (MRI) and hematoxylin-eosin staining (HE) of the mass in left submandibular region (SMR). (A) sonography disclosed a well-defined mixed echogenic mass containing solid and cystic components. (B) Color Doppler showed that abundant blood flow signals could be seen in the solid part. (C) CEUS showed a cystic solid mass in the left SMR, the solid component was slightly hyper-enhanced at 18 s and the cystic component was non-enhanced. (D) the solid component enhancement was slightly wash out at 43 s. (E) Axial T2-weighted image showed the left-sided cervical mass with well-defined margins, and no evidence of infiltration of the surrounding structures. (F) Coronal T2-weighted image showed a nodule with T2-low intensity inside the mass. (G) HE staining showed the cystic lumen was filled with papillary tumor proliferation (magnification, 100×). (H) The tumor surface was lined with a single layer of cuboidal epithelial cells (magnification, 400×).
We report a case of extraoral type of IDP arising from the SLG. To our knowledge, extraoral type of IDP occurring in the SLG is rare. The aetiology of IDP is unknown but a possible association with masticatory trauma has been proposed [2]. Histologically, IDP has a delicate papillary network of cell-lined vascular fronds and the papillae partly fill the cystic cavity. In this case, the IDP of SLG presenting submandibular mass is because the mass was extending beyond the mylohyoid through a congenital dehiscence in the mylohyoid or between the mylohyoid and hyoglossus along the deep lobe of the SMG.
According to a previous report [3–5], CEUS and MRI are helpful for evaluating the location, internal features, and behavior of the mass; however, it is difficult to make a diagnosis of this mass preoperatively through radiologic studies because IDP arising from the SLG are very rare and atypia [6]. In our case, the CEUS and MRI findings were not the same. CEUS images showed the solid part was enhanced, while the MRI images showed the solid part was not enhanced. Because the CEUS was a real time examination.
There were some limitations in this case. On one hand, this was a retrospective study, the partial data was not complete. On the other hand, we have not displayed a gross histopathological photograph of the surgical excision and clarify the positional relationship between the epithelium of the salivary duct and the intraductal papilloma.
Extraoral type of IDP in SLG is a rare disease that should be considered in the differential diagnosis of salivary lesions. A complete SLG resection and long-term follow-up should be recommended for recurrent case.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors declare that there is no conflict of interest.