
Abstract
BACKGROUND:
In coronary artery disease (CAD), an alternative way of improvement of blood circulation in the ischemic area of the myocardium is coronary collateral circulation. Our study aimed to investigate the rheological parameters of blood and nitric oxide (NO) content in patients with various degrees of collateral development and the likelihood of the influence of blood fluidity on collateral angiogenesis.
METHODS:
We studied patients with stable CAD who underwent elective coronary angiography and a control group with the same mean age. We investigated patients with different degrees of developing collaterals and those without them. In studied patients, the blood plasma viscosity, aggregability, and deformability of erythrocytes, as the main indicators of blood rheology. We recorded content of stable metabolic end products of nitric oxide (NOx).
RESULTS:
Results of the studies showed that in the blood of studied patients with CAD erythrocyte aggregation was increased and NO content decreased compared to the control level; NO content was as lower, as less was the number of developed collaterals was recorded.
CONCLUSION:
In this work, the role of the aggregation ability of erythrocytes and the endothelial origin of NO in the direct and feedback regulatory mechanism of angiogenesis in patients with CAD are discussed.
Keywords
Background
Coronary artery disease (CAD) along with chronic respiratory and oncological diseases, is a leading cause of adult death worldwide. Although CAD mortality has gradually declined over the last decades in developed countries, it still causes about one-third of all deaths in people older than 35 years; mortality from CAD to continue increasing in developing countries. This indicates the need for implementing effective primary prevention approaches for complications of CAD (myocardial infarction, unstable angina with concomitant disability and mortality) worldwide and identifying risk groups and the possibility of improvement in the course of the disease. The exacerbation of coronary heart disease, characterized by a high risk of myocardial infarction and sudden death [1], is related to damage to the atherosclerotic plaque, which causes the ingress of thrombogenic substances from the lipid core into the bloodstream, that in turn, leads to activation and adhesion of platelets [2] mediated by alterations in the carbohydrate composition and spatial structure membrane glycosylated proteins [3–5] that leads to an increased tendency to thrombosis. However, changes in coronary circulation cannot be attributed to platelet-associated factors alone. Damage to the surface of the endothelium triggers an increase in the release of inflammatory factors in blood plasma; neutrophils are the first to react to damage [6], producing inflammatory mediators and free oxygen radicals [7, 8]. In addition to platelet and neutrophils factors, in blood flow regulation the erythrocytes play a special role by changing their aggregation ability as well as deformability, which can be considered a therapeutic target.
In CAD, an alternative way of improvement of blood circulation in the ischemic area of the myocardium is coronary collateral circulation [9]. In more than 30% of patients with ischemic heart disease, collateral coronary blood flow prevents the development of myocardial ischemia during short-term occlusion of the coronary arteries [10]. The collateral coronary blood flow can compensate for myocardial blood supply during coronary artery stenosis by 75–80% [1, 11]. Well-developed collateral coronary blood flow in patients with coronary heart disease provides a reduction in the infarction zone, as well as an increase in survival [11–13]. However, the mechanisms contributing to the development of collateral circulation remains debatable.
The development and structuring of collateral blood flow are associated with the inflammatory process [14]. In the pathogenesis of any pathological process, especially in the event of inflammation, rheological changes (such as hematocrit, aggregation, and deformability of erythrocytes) in the blood together with vascular factors [15] determine the fluidity of the blood, which is involved in the architectonics of the blood supply [14] and undoubtedly, play a special role in collateral angiogenesis. Their functional role in collateral circulation has not been sufficiently studied.
Recent evidence has shown that arteriogenesis is regulated by nitric oxide (NO), angiogenic factors, and shear stress. NO-mediated increase in vascular conductance allows for a rise in collateral-dependent blood flow to the tissue distal to the occlusion. NO production is critical to the efficacy of therapeutic arteriogenesis is achieved by the delivery of exogenous angiogenic growth factors (VEGF, FGF-2). The critical role of NO in therapeutic arteriogenesis is independent of NO-mediated changes in vascular conductance and implies a central role in arteriogenic signalling events.
Nitric oxide is involved in the regulation of vascular resistance, mediating the vasodilating effects of endothelium-dependent vasodilators (acetylcholine, bradykinin, histamine).
It inhibits the formation of the endothelial vasoconstrictor factor endothelin - I and the release of norepinephrine by the endings of sympathetic neurons, prevents the excessive effects of other vasoconstrictors (angiotensin II, thromboxane A2). Due to this, NO is involved in the regulation of vascular tone and blood flow, systemic hemodynamics and microcirculation [16, 17].
Changes in the geometry of the vascular bed due to vasodilation to a change in the rheological properties of blood [18], especially its viscosity [19]. As experiments with erythrocyte models showed, the quantitative and qualitative composition of erythrocytes determines the degree of blood viscosity. At high flow rates (in the arterial network), or at high rates (in capillaries), the maintenance of blood flow is determined by the ability of erythrocytes to change their shape [20]. The degree of deformation of erythrocytes depends on the external forces acting on the cells and their deformability [10]. Blood viscosity also depends on aggregation [20–22]. Human erythrocytes are sensitive to induced and constitutive forms of nitric oxide. Erythrocytes themselves can synthesize nitric oxide [23]. Nitric oxide synthesized in erythrocytes may be involved in the regulation of the physiological behaviour of erythrocyte as well as external nitric oxide [23]. Nitric oxide may have a regulatory effect on the deformability and aggregation of erythrocytes [24].
Thus, the rheological properties and the content of nitric oxide are in a certain way cross-values. But there is no reliable information about the quantitative state of collaterals and rheological factors, the content of nitric oxide in patients with CAD.
Our study aimed to investigate the rheological parameters of blood and nitric oxide (NO) content in patients with various degrees of collateral development.
Materials and methods
Patients
We studied 82 patients (60 males and 22 females, mean of ages 56±2.3 years) with stable coronary artery disease who underwent elective coronary angiography. Criteria for inclusion in the study: all patients had stenosis in one or more coronary arteries with a diameter of more than 1.5 mm and narrowing of the lumen by 50% was observed. Exclusion criteria from the study: myocardial infarction, vasospastic angina, severe circulatory failure (NYHA IV); oncology, autoimmune diseases, pronounced dysfunction of the respiratory organs, kidneys, liver, decompensated diabetes mellitus, arterial hypertension that cannot be treated. For comparison, we examined a control group of apparently healthy male and female volunteers (male:female - 3 : 1).
In studied patients and control group volunteers, the blood plasma viscosity, aggregability, hematocrit, and deformability of erythrocytes, as the main indicators of blood rheology, were investigated. The study protocol was proved by the Ethical Committee of the Multidisciplinary Science High School [extract from protocol #202005001]. Original informed consent, which was agreed upon with the directorate of the polyclinic and hospital unit, was signed by each patient. In all patients, the state of collateral blood flow in the myocardium was assessed using coronary angiography [Siemens AR pheno, Germany]. Quantification of coronary collaterals was performed according to the modified Rentrop method [25]. In clinical practice, there is a scale for assessing the collateral network: 0-1 point - poorly developed collaterals, 2-3 points - well-developed collaterals [25, 26]. Patients were divided into subgroups depending on the number of collaterals: in the I subgroup (0 points) there were 20 patients, in the II subgroup (1 point) there were 8 patients, in the III subgroup (2 points) there were 24 patients, in the IV subgroup (3 points) there were 26 patients.
Investigate of RBC aggregation index by “Georgian Technique” (EAI)
We used the “Georgian Technique” to investigate the RBC aggregation index. The erythrocytes aggregation index counts as the area of aggregated erythrocytes divided by the full area of the erythrocytes in the volume unit. Blood samples were centrifuged and about 0.1 ml of blood was diluted at 1 : 200 in its plasma in the Thoma pipettes preliminary rinsed with 5% sodium citrate solution (660 mosmol/l; pH = 7,5) without the addition of any other anticoagulants to the blood under study. We used sodium citrate for sputtering from the inside of tubes and melangeurs (rinse the tube and melangeurs) for blood as part of the “Georgian Technique”.
Sodium citrate is a universal anticoagulant (buffer compound that prevents pH change), a well-established main transfusion anticoagulant for blood and its components, is part of the know-how of “Georgian Technique”, which is direct and accurate.The quantitative index of erythrocyte aggregation, which was assessed with a special program at the Texture Analysis System (TAS-plus, “Leitz, Germany), represented itself the relationship between the aggregated and unaggregated red cells [27, 28].
Investigate of RBC deformability index (EDI)
Evaluation of the erythrocyte deformability index was performed with an aid of the nucleopore membrane filter method, which is based on assessing the velocity of the erythrocytes’ passage through the very small pores (5μm, which is a diameter of the smallest capillary) of the filter, at constant pressure (10 cm of water column) and temperature (37°C). The pure erythrocytes were obtained by centrifuging the blood sample at 3000 g for 15 min. The resulting plasma was aspirated with a micropipette and the remaining blood cells were added with bovine serum albumin (0.2 mg per 5 ml) dissolved in the phosphate buffer. Then the blood was centrifuged a second time at turn over/m for 15 min. The precipitated erythrocytes, as well as a thin layer of leukocytes and thrombocytes, were separated with the help of the phosphate buffer. To purify the blood from leukocytes and platelets, we used a round, with a uniform distribution of the filtered medium, a filtering membrane made of a multilayer modified polyester with a spatial structure (Lidkor, Russia). This procedure was repeated three times. Purified erythrocyte mass was diluted in the phosphate buffer, with a hematocrit of 10%. Evaluation of the deformability index implied measuring the velocity of the erythrocyte passage through the filter (mm/min) was recorded. The high-quality polycarbonate filters (with 5μm diameter pores) were used in measuring procedures. Measuring RBC filterability by weighing the amount of RBC filtered through micropore membranes is performed on washed RBC resuspended in phosphate-buffered saline. The filtration step was performed using gravity alone and the amount of the filtered suspension is referred to the filtration of PBS alone through the same membrane. A reproducibility was same as used Dormandy technique (5.3 vs. 5.6 %) [29].
Investigate blood plasma viscosity
Blood plasma viscosity was examined in the capillary viscometer at 37°C, where the movement of plasma in the capillaries is induced by the force of gravity [30]. We use viscosimeter BKcy-4 (Bulgary).
Investigate total NOx level in blood serum
The level of NOx in the blood serum samples was determined by a modified method by Miranda et al. [31]. We recorded the content of stable metabolic end products of nitric oxide (NOx). As the first step, sample deproteinization was achieved by adding equal volumes of 0.3M NaOH to 100μl of blood serum. It was mixed well and incubated for 5 min at room temperature. Then 100μl of 5% ZnSO4 was added, mixed well, and incubated for an additional 5 min at room temperature. After the incubation, the mixtures were centrifuged at 3000 rpm at 4°C for 15 min. An aliquot of 100μl of the clear supernatant was then mixed with 200μl of Griess Reagent, which was prepared just before the assay and contained 0.25% VCl3, 0.1% sulfanilamide, and 0.05% N-(1-Naphthyl)-ethylenediamine (NEDD) in 0.5 M HCl. The reagent blank was the same but contained 100μl of distilled water instead of the sample. The mixture was incubated for 30 min at 37°C and absorbance was measured at 540 nm with a microplate reader (Multiscan GO, Thermo Fischer Scientific, Finland). The standard curve for NaNO2 was used to calculate the total NO concentration in the samples [32].
Statistical analysis
We used Origin 8.1 for Mac for calculated two independent samples T-tests, and Kruskal-Wallis’s test.
Results
Coronary angiography results
In Figs. 1–4 the angiograms of patients without and with different degrees of development of collaterals (according to Rentrop classification) are shown.
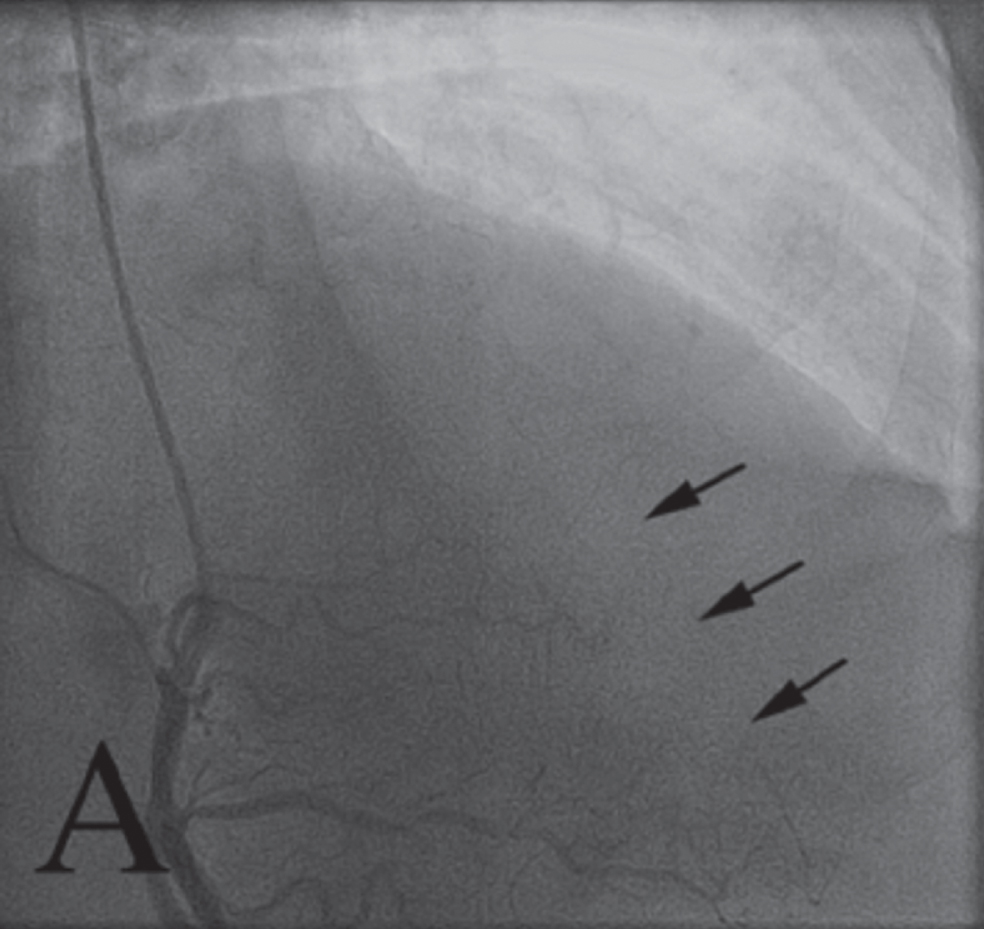
Example A. It is of coronary angiography of a patient from I subgroup. The patient has 0 degree of development of collaterals according to Rentrop classification (Rentrop Grade 0). Rentrop Grade - left anterior descending artery chronic total occlusion with no visible collaterals from the right coronary artery donor vessel, arrows indicate left anterior descending artery (not seen)).
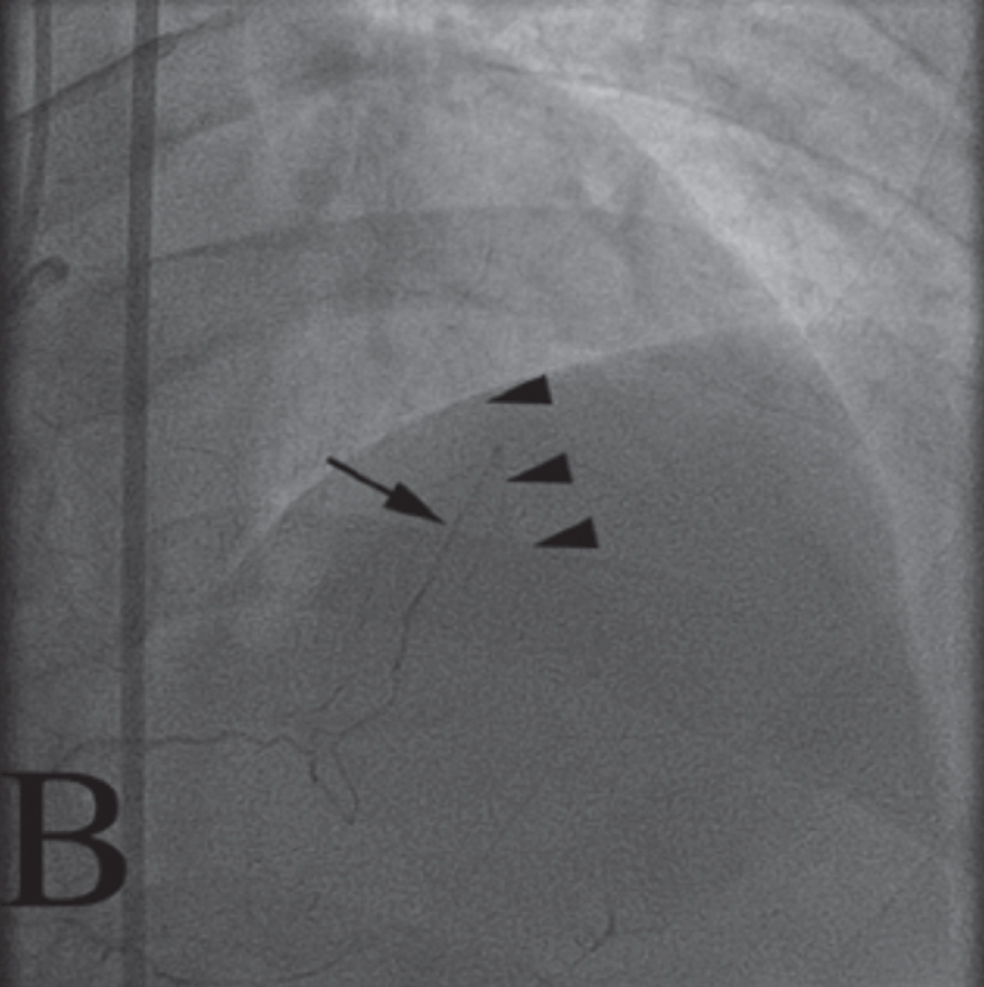
Example B. It is of coronary angiography of a patient from II subgroup. The patient has 1st degree of development of collaterals according to Rentrop classification (Rentrop Grade 1). Rentrop Grade 1 - collateral (arrow) from the right coronary artery to left anterior descending artery (arrowheads).
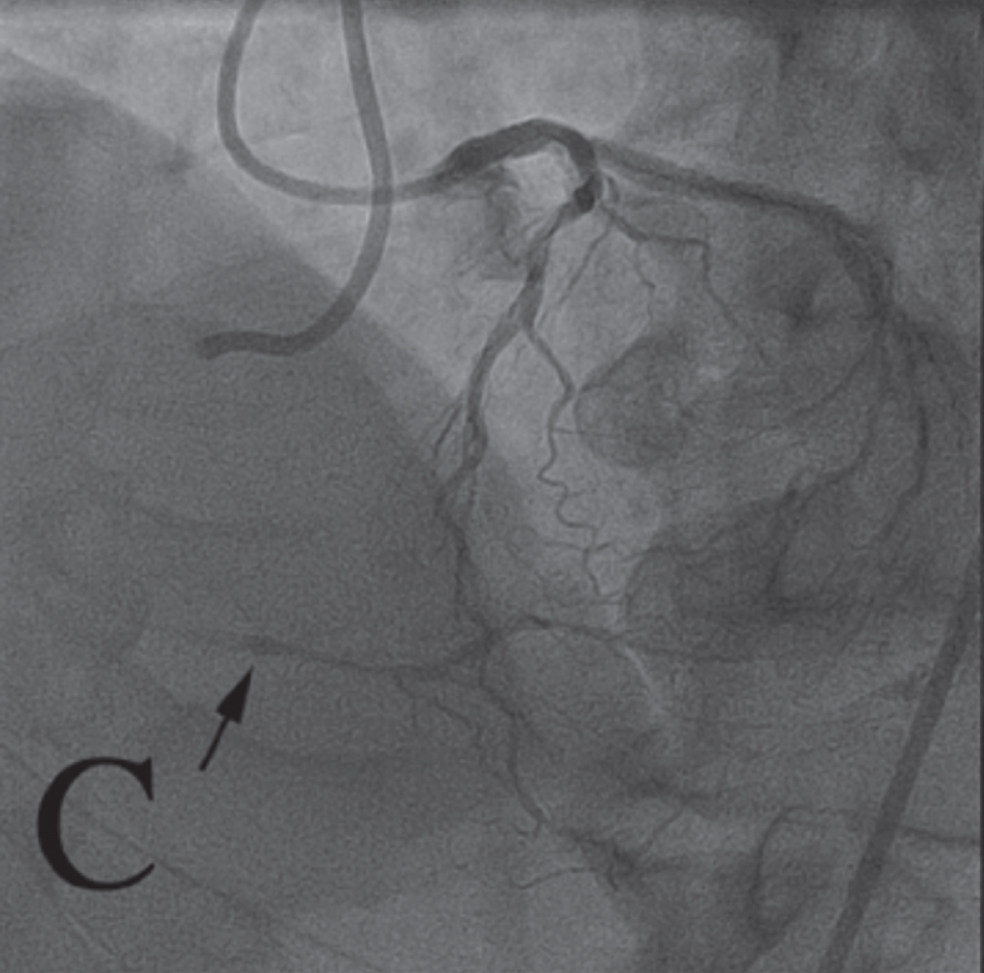
Example C. It is coronary angiography of a patient from III subgroup. The patient has 2nd degree of development of collaterals according to Rentrop classification (Rentrop Grade 2). Rentrop Grade 2 - collateral from left anterior descending artery to right coronary artery resulting in partial filling of the right coronary artery chronic total occlusion (arrow).
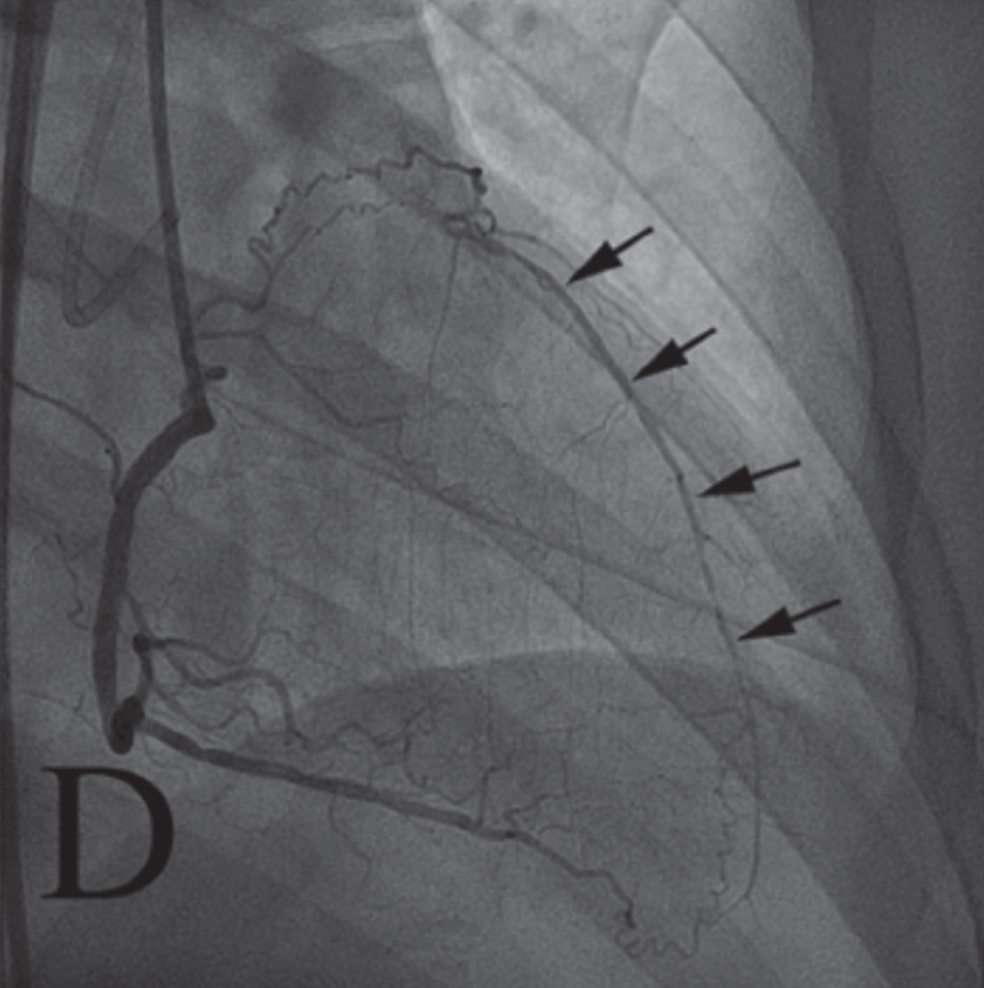
Example D. It is coronary angiography of a patient from the IV subgroup. The patient has 3rd degree of development of collaterals according to Rentrop classification (Rentrop Grade 3). Rentrop Grade 3 from the right coronary artery resulting in complete filling of left anterior descending artery chronic total occlusion (arrows).
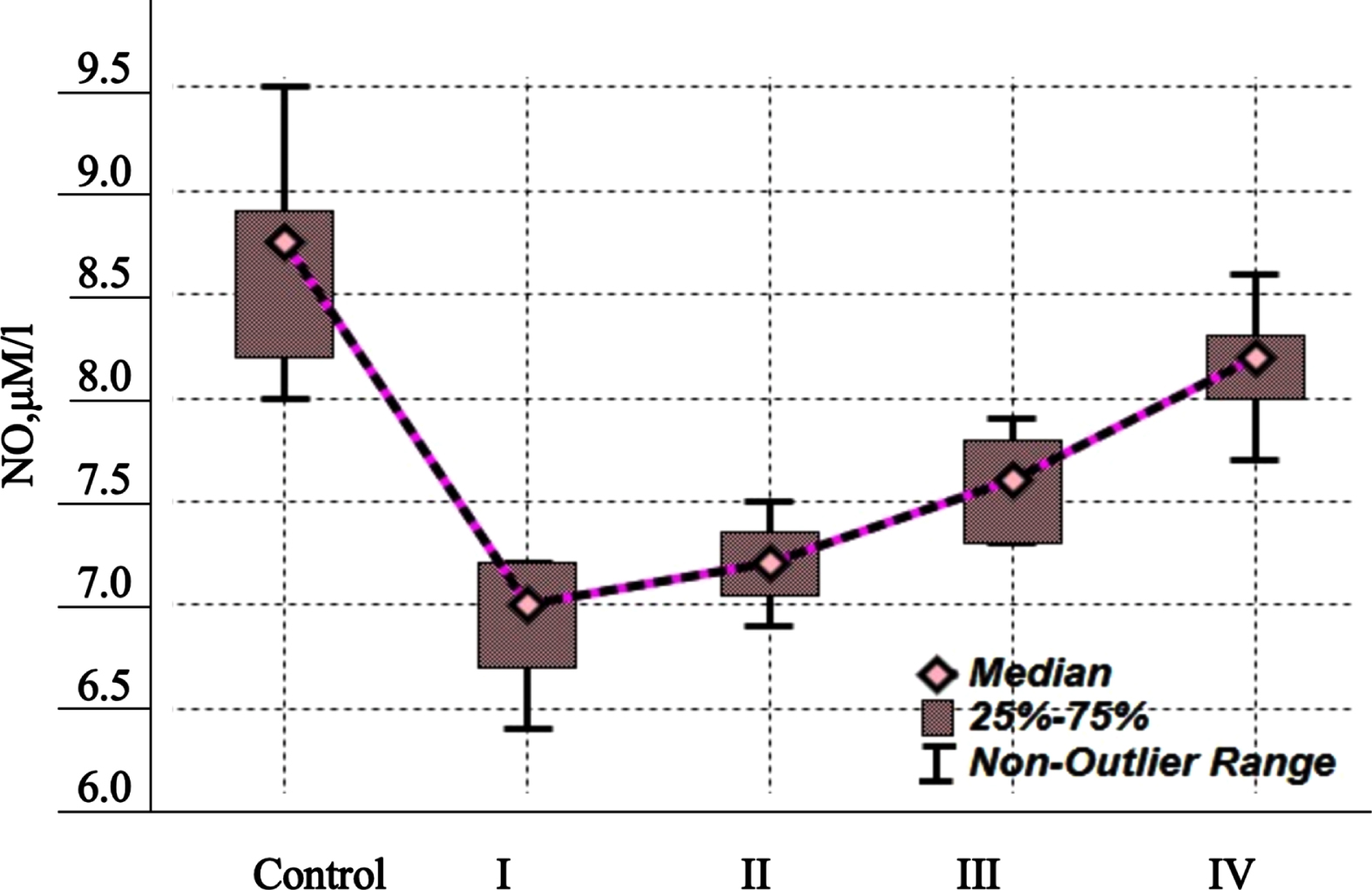
The indicators of NO (μM/l) content in the blood serum of studied patients with CAD and different numbers of developed collaterals. H = 34.880; p**.
In all patients with CAD, the erythrocyte aggregability index, erythrocyte deformability index, and blood plasma viscosity were studied (Table 1). As seems from the data introduced in Table 1, the EAI in patients of groups III and IV (with 2-3 collaterals located distal to the stenosis/occlusion) was statistically significantly increased in comparison to the EAI level in healthy volunteers (pIII - 0=*; pIV - 0=*); in patients from groups II and I (with 1 visible collateral and without visible collaterals) EAI increased importantly in comparison to data of patients from III-IV groups and healthy volunteers (pII - 0=*; pI - 0=*).
The insights of erythrocyte aggregability index (EAI), erythrocyte deformability index (EDI), and blood plasma viscosity in patients with CAD with different numbers of collaterals
The insights of erythrocyte aggregability index (EAI), erythrocyte deformability index (EDI), and blood plasma viscosity in patients with CAD with different numbers of collaterals
Note: EAI –erythrocyte aggregation index, EDI –erythrocyte deformability index, Vpl –plasma viscosity. M±m.
The insights of the EDI and blood plasma viscosity in the blood of the patients with CAD (groups I, II, III, IV) did not change in comparison to the control level.
The indicators of NO content in the blood serum of studied patients with CAD and different numbers of developed collaterals are shown in Fig. 1. As seems from the data introduced in Fig. 1, in the studied patients with CAD the content of NO decreased compared to the control, the content of NO was as lower, as less developed collaterals were recorded (F = 19.46, p < 0.001).
Discussion
On obstruction of a major artery, the presence of a collateral circulation as a natural-bypass system provides retrograde perfusion of the tissue distal to the occlusion. Thus, the native conductance and subsequent expansion of the collateral circulation in disease have tissue/life-saving significance.
In the last 50 years, several studies have been carried out that have demonstrated a close relationship between the state of collateral blood flow and prognosis in patients with CAD. In the study by E. K. Kim et al. patients with myocardial infarction and well-developed collateral circulation have lower levels of mortality and morbidity [33]. In patients with good collateral blood flow, the area of infarction is significantly smaller than in patients with poor blood flow, which can be considered an independent predictor of a larger infarction area [34–36].
Assessment of collateral circulation provides additional information for determining the risk of cardiovascular complications in patients with coronary heart disease. Therefore, it is especially important to study the factors involved in the development of collateral blood flow, as well as the development of alternative methods for improving the blood supply to ischemic tissues [37].
According to our study results, in patients with CAD with poorly developed collaterals, erythrocyte aggregation was increased by almost 80% compared to the control, while in patients with well-developed collaterals, aggregation was only 35% more intense than in control. Usually, the alterations in erythrocyte aggregability are correlated with the plasma viscosity [32], however, in our study, this correlation was not revealed, and the relation of EAI with erythrocyte deformability in all subgroups of patients also was not detected.
The number of subjects does not make it possible to reliably state this with great accuracy, but we can reliably tell erythrocyte aggregation is correlated with count of collateralies.
The obtained data can be interpreted that increased aggregation of erythrocytes is not a facilitative condition for the formation of collaterals, and it is also possible that the growth of collaterals (many clathers) prevent an abnormal increase in the aggregability of erythrocytes. Both views confirm the connection of processes, thereby emphasizing the duality and significance of aggregation.
The increased erythrocyte aggregation prevents the formation of new collaterals, which is very important for a favourable outcome of the disease. The number of anastomoses directly depends on the course of the disease, therefore, all studies and recommendations, exogenous therapy (including antiplatelet agents, lipid-lowering, and antianginal drugs), facilitating a reduction in aggregability and improvement in blood fluidity and can become the basis for stimulating collateral angiogenesis are valuable.
In normal tissues at rest, fluctuations of flow and shear stress in the midzone of native collaterals are negligible due to too little or no pressure gradient between the cross-connected arterial trees [38].
Obstruction of a conduit artery creates a pressure gradient across the collaterals that induces a large increase in shear stress. An acute increase in shear stress upregulates eNOS expression and phosphorylation and promotes its intracellular translocation in endothelial cells [39, 40]. NO-induced relaxation of arteries vascular smooth muscle [41] which then outwardly remodels in response to chronic dilation. If an obstruction is continuous, over the subsequent days-to-weeks collateral outward remodelling ensues forming large, tortuous, conduct arteries (arteriogenesis - a new blood vessel formation from the pre-existing vascular bed).
It was demonstrated that eNOS may be involved in collateral remodeling and physiologic angiogenesis [42] that constitutes a naturally occurring, compensatory response to tissue ischemia [43]. NO is important for the early steps of neovascularization - endothelial cell proliferation and/or migration, Arteriogenesis is inhibited by diabetes, dyslipidemia, atherosclerosis, hypertension, oxidative stress, aging, smoking and other diseases, characterized by impaired endothelial nitric oxide synthase (eNOS) activity and/or NO bioavailability, collectively termed “endothelial dysfunction”.
According to our study results, the NO content in the blood serum of studied patients with CAD decreased compared to the control level, and was as lower, as less developed collaterals were recorded. These results agree with the above literature data.
In the series of studies, there was tested the relation between blood serum NO content and EAI [44]. It was shown that an increase in NO content in the blood decreases the aggregability of erythrocytes. The underlying mechanisms at the origin of these phenomena are unclear but might involve membrane/cytoskeletal protein nitrosylation or oxidative stress modulation [45].
On the other hand, RBC aggregation may have an impact on endogenous NO production by endothelial cells. It has been established that blood flow and wall shear stress in the vascular system stimulate NO synthesis by endothelial cells [46], and decreased blood flow suppressed eNOS expression and flow-mediated dilation responses in small arteries [47]. Decreased blood flow is associated with increased RBC aggregation and ultimately results in reduced wall shear stresses [48]. Of course, there must be considered the alterations of perfusion pressure and the dilatory ability of the vascular system [39], also axial migration of RBC away from blood vessels towards central flow streamlines during enhanced RBC aggregation resulting in a less-viscous, plasma-rich region near vessel walls and decreased wall shear stress affecting NO-related mechanisms in the vascular system [36].
Thus, based on the results of our studies, it follows that in the blood of studied patients with CAD erythrocyte aggregation was increased and NO content decreased compared to the control level; NO content was as lower, as less was the number of developed collaterals was recorded; count of catalateralies in patients with CAD had net link of degree of agregation of erythrocyte: the more collaterals were developed, the less erythrocyte aggregation was, but it always exceeded the control values. In this work, the role of the aggregation ability of erythrocytes and the endothelial origin of NO in the direct and feedback regulatory mechanism of angiogenesis in patients with CAD are discussed.
In this work, the fact of change of the erythrocytes aggregation ability and NO are showd, as well as direct and feedback links and assumptions about involment that factors in colateralies development proces in patients with CAD are discussed.
Further use of these approaches and research protocols involving for large number of patients of various age groups will be able give special ruls for menegmentes of Ptients with CAD. The simultaneous study of the rheological properties of blood and NO in blood serum in patients with CAD will enable faster and more effective management of patients, and can also form the basis of personification, which is the main link for the success of cardiac procedures.
Our research has an applied character. Modern methods of biomedicine and a multidisciplinary approach to the study of patients with acute coronary syndrome make it possible to study the intimate biological basis of collateral circulation, identify mechanisms that limit the development of collaterals, which will serve as the invention of new methods for assessing the state of collateral blood flow, and the development of therapeutic agents to improve the state of the collateral network.