
Abstract
BACKGROUND:
Arteriovenous malformations (AVMs) are vascular anomalies characterized by abnormal shunting between arteries and veins. The progression of the AVMs and their hemodynamic and rheological relations are poorly studied, and there is a lack of a feasible experimental model.
OBJECTIVE:
To establish a model that cause only minimal micro-rheological alterations, compared to other AV models.
METHODS:
Sixteen female Sprague Dawley rats were randomly divided into control and AVM groups. End-to-end anastomoses were created between the saphenous veins and arteries to mimic AVM nidus. Hematological and hemorheological parameters were analyzed before surgery and on the 1st, 3rd, 5th, 7th, 9th, and 12th postoperative weeks.
RESULTS:
Compared to sham-operated Control group the AVM group did not show important alterations in hematological parameters nor in erythrocyte aggregation and deformability. However, slightly increased aggregation and moderately decreased deformability values were found, without significant differences. The changes normalized by the 12th postoperative week.
CONCLUSIONS:
The presented rat model of a small-caliber AVM created on saphenous vessels does not cause significant micro-rheological changes. The alterations found were most likely related to the acute phase reactions and not to the presence of a small-caliber shunt. The model seems to be suitable for further studies of AVM progression.
Introduction
Arteriovenous malformations (AVMs) are vascular anomalies consisting of a feeding artery and a draining vein without an intervening capillary network connected by a high-flow nidus [1–5]. AVMs predominantly occur in the brain and spinal cord but can also manifest in other organs, such as the lungs, kidneys, on coronaries or on extremities [2, 5–7]. The clinical significance of AVMs is highlighted by the complications they can generate and the difficulties linked to their treatment. Often incidentally diagnosed, AVMs can be life-threatening due to their high shear stress, with 38–68% of new cases presenting as hemorrhage [8–10]. Other clinical manifestations include headaches and seizures [8, 9].
Understanding flow conditions in AVMs is important, as some studies suggest that changes in hemodynamics, particularly venous drainage, lead to AVM development rather than vice versa [2, 11]. During embryogenesis, anomalies in the cerebrovascular system, such as venous occlusions, stenosis, or agenesis, are thought to arise, resulting in increased cerebral venous pressure and chronic venous hypertension, which may reduce tissue perfusion and activate the hypoxia-inducible factor (HIF), VEGF, and angiogenic cascade [2, 11–13]. In addition, postnatally, venous occlusion can reopen preexisting arteriovenous connections, which can pathologically evolve into AVMs [11]. The occurrence of spontaneous growth and regression in AVMs provides evidence that the formation of these lesions extends beyond the embryonic development phase: chronic hypoxia, shear stress, exercise, or hormonal fluctuations alter AVM morphology and direct trauma regardless of the location of the AVM [4, 15].
Experimental models are employed to investigate the occurrence of perfusion pressure breakthrough, venous hypertension, and thrombosis in AVMs. Several large and small animal models are known to study AVM pathophysiology in which hemodynamic arrangement differ: e.g., various anastomosis types between the common carotid artery and the external jugular vein rete mirabile, rete-cavernous fistula model, end-to-end anastomosis between the superficial temporal artery and the middle cerebral artery and end to side anastomosis between the superficial temporal artery and the dorsal sagittal sinus, femoral vein graft connected to a cortical branch of the middle cerebral artery and the superior sagittal sinus, radiosurgery models, teleangiectasia models, transgenic arterio-venous fistula models [16–25]. However, their hemodynamic effect can be acute and significant.
The presence of arteriovenous shunt in various sizes and localization may affect micr-rheological parameters. Previous studies demonstrated significantly increased red blood cell aggregation, and impaired deformability that also alters over the postoperative weeks after performing artificial carotid-jugular, femoral or saphenous arteriovenous [26–29] and portacaval shunts [30]. The magnitude of changes varied depending on the artificial shunt’s size, geometry and localization. Concerning AVM, since they are usually differ in size as well, it is not known what the size and vascular morphology of the AVM is that cause not only hemodynamic but hemorheological disturbances, as well.
In this study the aim was to establish a model that cause only minimal micro-rheological alterations, compared to other AV models, being feasible for studies on AVM progression.
Materials and methods
Experimental animals
The experiment was registered by the University of Debrecen Committee of Animal Welfare (UDCAW) and approved and by the National Food Chain Safety Office (registration Nr. 25/2016/UDCAW, 25/2022/UDCAW) in accordance with the national (Act XXVIII of 1998) and EU (Directive 2010/63/EU) regulations. Sixteen female outbred CD® (Sprague Dawley) rats (Charles River Laboratories International, Inc., 12-week old, bodyweight: 293.21±10.33 g) were used in the study. The rats were housed in a conventional microbiological status animal facility, in standard cages (1354 G Eurostandard Type IV, 595 x 380 x 200 mm, floor area 1820 cm2, Tecniplast, Italy), in alternating day and night light conditions in a 12 h cycle, and were given unrestricted access to commercially available rodent chow (SAFE® D132 autoclavable complete universal vegetal diet for rats, mice and hamsters) and tap water.
Experimental protocol (operative techniques and samplings)
Rats were anesthetized using a mixture of ketamine (100 mg/kg), atropine (0.05 mg/kg), and xylazine (10 mg/kg) intraperitoneally [31, 32]. The depth of anaesthesia was assessed by monitoring the absence of pain: pinching the toe on the hind limb (loss of pedal reflex) and pinching the tail. The pattern and depth of respiration and color of mucus membranes were also evaluated. The entire operation and measurements were completed within about 60–70 minutes. For maintaining the anesthesia ketamine was used when it was required. We then gave the rats an intravenous heparin injection (80 IU/bwkg) to prevent thrombotic events. For the operations sterile instruments were used.
Animals were randomly divided into a Control group, referred to as sham-operated (n = 8), and to an AVM group (n = 8). A 26-gauge cannula was inserted into the lateral tail vein for blood sampling. The lower abdomen and inner thighs were shaved and disinfected using povidone-iodine (Betadine, Egis Pharmaceuticals PLC, Hungary). The surgical site was isolated with sterile gauze before making a 3-cm oblique incision above the right knee joint. In the AVM group, the procedure involved saphenous veins and arteries with diameters between 0.3–0.4 mm. We atraumatically dissected the vessels and performed distal ligation and proximal clipping of both the artery and vein, which made cutting the vessels easier. The vein was cut more distally than the artery for flexibility and space during the remaining surgical steps. The vessels were washed with heparin and carefully mobilized to a suitable position.
For end-to-end anastomosis procedure we used 3/8 serosa (taper) needles with 10/0 non-absorbable polyamide-6 thread. The first stitch was used to place the initial suture at the 12 o’clock position (180°, away from the operator) on both vessels, the next was placed on the opposite end of the vessel, at the 6 o’clock position (0°, closest to the operator). The third stitch was located midway in between. After securing the threads they were knotted to close the anastomosis’ front wall. The vessels were flipped, and final stitches were placed in the middle of the back wall to complete the anastomosis. We tested the anastomosis for any leakage by removing the proximal microvascular clip from the venous side and checking for flaws. If none were found, we removed the arterial microvascular clip, temporarily placed subcutaneous fat on the anastomosis to improve coagulation if necessary, and performed the double occlusion or ‘milking test’ to assess patency [33]. Skin closure was done using a 4/0 absorbable polyglecaprone thread with a 3/8 cutting needle and continuous sutures.
In the Control, as a sham-operated group, skin incision and atraumatic vessel preparation were performed without anastomosis. The rats remained anesthetized for 60 minutes, which was the time required to complete the anastomosis in the AVM. The skin as the AVM group was closed in the same manner. For postoperative analgesia tramadol (15 mg/kg, i.p., Contramal 50 mg/ml; Teva Pharmaceutical Industries Ltd., Israel) was used for three consecutive days.
Besides perioperative samplings (before and just after the operation), blood samples (300μl each) were collected from the lateral tail vein via a 26-G cannula under short anesthesia on the 1st, 3rd, 5th, 7th, 9th, and 12th postoperative weeks. The blood was collected into Vacutainer tubes (BD Vacutainer® tubes, 5.4 g K3-EDTA, 3 ml). At the end of the follow-up period the animals have been over-anesthetized.
Laboratory measurements
A Sysmex K-4500 automate (TOA Medical Electronics Co., Ltd., Japan) was used to measure hematological parameters. The following parameters were analyzed in this study: RBC count (1012/L), white blood cell (WBC) count (109/L), platelet number (109/L), hematocrit (%), hemoglobin concentration (g/L), and mean corpuscular volume (fL).
To measure erythrocyte aggregation, a Myrenne MA-1 erythrocyte aggregometer device (Myrenne GmbH, Germany) was used, based on the light-transmittance method to express the aggregation index values [34, 35]. M 5 s and M 10 s were tested at 0 s–1 share rate as well as M1 5 s and M1 10 s aggregation indices at a shear rate of 3 s–1 were determined.
A LoRRca MaxSis Osmoscan ektacytometer (Mechatronics BV, The Netherlands), based on laser-diffractometry method, was used for the erythrocyte deformability assessment [34]. For each test, 10μl blood was suspended in 2 ml of polyvinyl-pyrrolidone (PVP) and phosphate-buffered saline (PBS) solution (viscosity = 27 mPa.s, osmolality = 300 mOsm/kg, pH = 7.3). The elongation index (EI) of the RBCs in the function of shear stress (SS, range: 0.3–30 Pa) was determined [34, 35]. For comparing the EI-SS curves, raw data, EI values at 3 Pa were used, and by the parameterization of the EI-SS curves (Lineweaver-Burke analysis), the maximal EI (EImax), the shear stress at half-EImax (SS1/2), and their ratio (EImax/SS1/2) were calculated [35, 36].
Statistical analyses
The Mead’s resource equation method was used to determine the sample size. The statistical analysis was carried out using GraphPad Prism 9 software. Data distribution with normality test was checked for all comparisons. Depending on the normality of data distribution, for inter-group comparison at a given time point Student t-test or Mann-Whitney RS test, and for intra-group comparison Kruskal-Wallis and Dunn’s method of ANOVA tests were applied.
Results
Bodyweight increased in both groups as animals aged over the 12-week follow-up period (Control group: from 299.2±4.55 g to 355±13.88 g, 18.56±6.16%; AVM group: from 287.25±8.66 g to 334.89 g, 16.56±3.22%).
Hematological parameters
Table 1 summarizes the absolute and relative (compared to own base) hematological values. Most of the significant changes in the hematological parameters were observed during the 1st p.o. week, wherein both groups had a marked decrease in the red blood cell count, hematocrit, and hemoglobin concentration. These values normalized by the end of the 12-week follow-up period. Leukocyte count increased after surgery in both groups, and it remained elevated until the 7th p.o. week in the AVM group. Values normalized at the end of the follow-up period in both groups The platelet count was significantly higher in the AVM group on the 5th p.o. week compared to the preoperative status, however, we did not find significant difference between the groups (Table 1).
Alterations of white blood cell count (WBC, 109/L), red blood cell count (RBC, 1012/L), hematocrit (Hct, %), hemoglobin concentration (Hbg, g/L), mean corpuscular volume (MCV, fL) and platelet count (Plt, 109/L) in Control and AVM group during the follow-up period of 12 weeks
Alterations of white blood cell count (WBC, 109/L), red blood cell count (RBC, 1012/L), hematocrit (Hct, %), hemoglobin concentration (Hbg, g/L), mean corpuscular volume (MCV, fL) and platelet count (Plt, 109/L) in Control and AVM group during the follow-up period of 12 weeks
Means±S.D.
Figure 1 shows the changes of RBC aggregation indices. The alterations in M 5 s, M1 5 s, M 10 s and M1 10 s aggregation indices were not uniform over the follow-up period. We found a kind of fluctuation in the values with wide individual alterations, resulting in a large deviation of data. In the AVM group values were often increased and remained elevated until the 9th p.o. week, however, without significant differences (Fig. 1).

Alteration of red blood cell aggregation index values: M 5 s (
Figure 2 shows the cumulative elongation index –shear stress curves in Control and AVM group. The standard deviation of EI values were small, the curves were almost overlapping, without significant differences. In Table 2 we summarized the comparative data of the EI-SS curves. EI at 3 Pa showed a slight, non-significant decrease in AVM group by the 1st p.o. week, together with a moderate increase in SS1/2 and so a decrease in EImax/SS1/2 values. Otherwise, the values were comparable between the two groups.
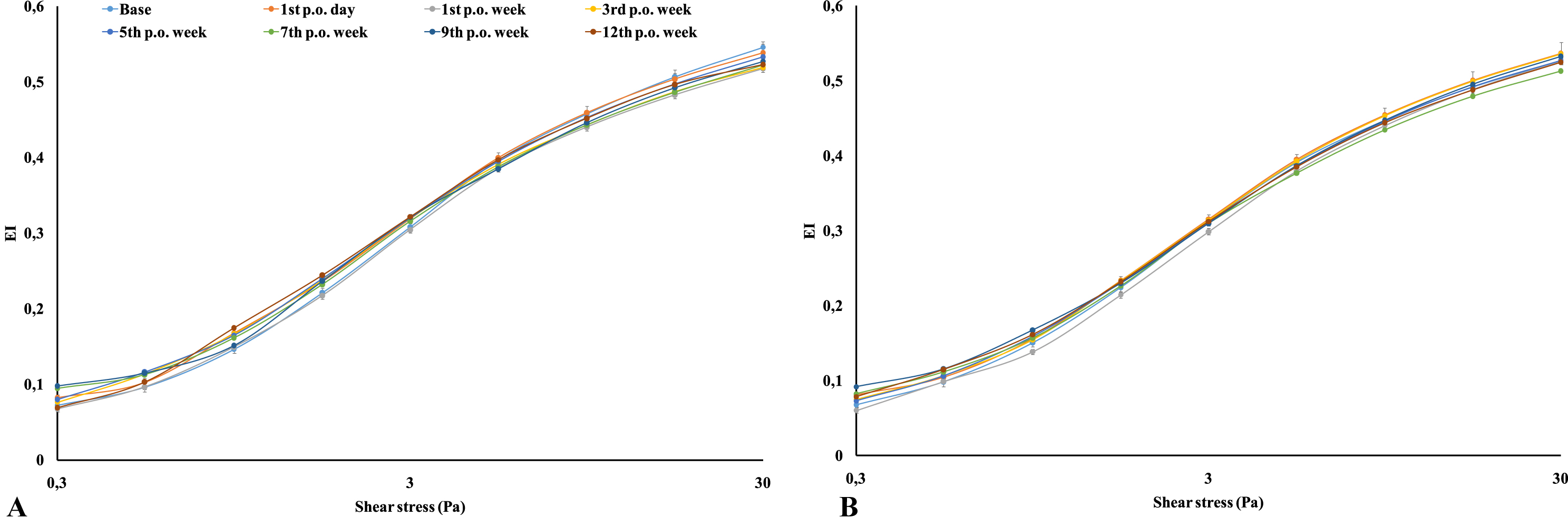
Elongation index (EI) –shear stress (SS, Pa) curves of the Control (
Comparative parameters of RBC elongation index (EI) –shear stress (SS) curves in Control and AVM group during the 12-week follow-up period
means±S.D.
Several experimental studies have investigated the hemodynamic and few the rheological changes that occur in AVMs. However, the main challenges of the experimental AVM models are inaccurate representation of AVM, “steal” phenomenon, hemodynamic load on the circulatory system, limited data of the pathological role in AVM rupture [4, 25]. In many AVM in the clinical practice systemic hemodynamic changes are not seen. Therefore, establishment of a feasible model is important to investigate the pathophysiology and progression of AVMs being comparable with the clinical cases.
The primary goal of our study was to establish a model with minimal micro-rheological effects, mimicking a small, still asymptomatic AVM that can be studied further to investigate the factors that play a role in the progression, enlargement and destabilization of the AVM.
The results showed that hematological and hemorheological parameters did not alter significantly in the AVM group compared to the sham-operated Control group. However, supposedly related to the acute phase reactions, immune/inflammatory mediated processes leukocyte count increased in the early postoperative period. We also observed slight decrease in red blood cell count, hematocrit and hemoglobin weeks. It was seen in the sham-operated group as well. Anesthesia (repeatedly over the follow-up period due to sampling) and the related immobilization, recovery period, blood samplings, surgical interventions (skin incision, tissue preparation, sutures, wound healing process in both groups) may explain these changes, including the irregular but slight increase in RBC indices and the transiently and moderately decreased RBC deformability [37–39].
In other rat models using artificial arteriovenous shunt on larger caliber vessels, the hemorheological alterations were much more obvious and significant. In case of carotid-jugular shunt. Technically and relatively, it is easier than the recent saphenous AVM model. In the carotid-jugular fistula model RBC deformability significantly impaired by the end of the 6-week follow-up period. The membrane (mechanical) stability test [40] showed much more lower deformability values after applying mechanical stress compared to sham-operated group [28]. Therefore, that model cannot be used for AVM progression studies, since its prompt hemodynamic and hemorheological effects are highly significant that would overlap other mechanisms. However, the aim of that carotid-jugular fistula model was to follow-up the maturation of the shunt, not as an AVM model.
In another rat model the superficial inferior epigastric vein was used to perform an arteriovenous connection in the femoral region. Hematocrit, red blood cell count, and hemoglobin significantly decreased by the 1st p.o. week, RBC aggregation significantly increased by the 5th week [29].
The mechanisms of micro-rheological disturbances in those cases include the previously mentioned acute phase related immune/inflammatory processes, alterations in the oxygenation level (depending on caliber and the magnitude of the blood mixing), and altered shear stress at the site and in the vicinity of the shunts [38, 39].
Conclusion
The presented rat model of non-congenital, small-caliber AVM created on saphenous vessels does not cause significant micro-rheological changes compared to other models using artificial arteriovenous shunts of different locations and sizes. The changes found are most likely related to the acute phase reactions and not to the presence of a small-caliber shunt. Therefore, the model seems suitable for further studies of AVM progression, enlargement or destabilization under different conditions (e.g., disturbed/altered angiogenesis and vascular remodeling, hypertensive and/or diabetic rat models). Based on our results, it can be also recommended that using this model the investigation on AVM progression (triggered by various conditions) should be started after at least a 12-week of maturation.
Footnotes
Acknowledgments
The authors are grateful to the technical staff of the Department of Operative Techniques and Surgical Research, Faculty of Medicine, University of Debrecen.
Conflict of interest
The authors declare no conflict of interest.
Ethical statement
The authors comply with the Ethical Guidelines for Publication in Clinical Hemorheology and Microcirculation as published on the IOS Press website and in Volume 63, 2016, pp. 1-2. of this journal.
Funding
The study was supported by the National Research, Development and Innovation Office (NKFI-1 “OTKA” K-139184).