
Abstract
BACKGROUND:
The impact of gravity on the existence of all living things has long been of interest to scientists. The force of the Earth’s gravity combined with hypoxia significantly affects blood circulation and blood accumulation in various parts of the human and animal body. To date, the relationship between body position and blood circulation in pulmonary circulation under hypobaric hypoxia has not been sufficiently studied.
OBJECTIVES:
Therefore, the research aims to determine the possibility of changing the body position in space on the reactions in the pulmonary circulation in the plains and highlands.
METHODS:
For this purpose, research was conducted on male Wistar rats, 44 of whom spent 150 days at an altitude of 3200 m above sea level, and 25 representatives of the control group - at an altitude of 164 m.
RESULTS:
The study revealed that gravitational redistribution of blood in mountainous conditions is less pronounced compared to the control group. This is explained by the remodeling of the vascular wall and an increase in its stiffness. It was found that a change in pulmonary artery pressure at the time of a change in body position was recorded both on the plains and in the highlands. On the plains, when the body position of rats was changed to passive orthostatic, a decrease in systolic and diastolic pulmonary artery pressure was noted, and when the body position was changed to passive anti-orthostatic, an increase in pulmonary artery pressure was observed. The increase in pulmonary artery pressure was a compensatory mechanism due to the increased stiffness of the pulmonary vasculature.
CONCLUSIONS:
The practical significance of this research is to expand the understanding of the pathogenesis of pulmonary hypertension in high-altitude hypoxia.
Introduction
The earth’s gravitational field has a significant impact on the distribution of blood volume in humans and animals. The phenomenon of blood redistribution has been demonstrated when the body’s position changes in space [1–3]. The unevenness of blood filling and blood flow in the pulmonary circulation is largely due to the forces of the earth’s gravity. Based on the analysis of the gravitational mechanism, functional zones were identified in the lungs [4, 5]. It was established that [6, 7], the stay of people or animals in high altitude conditions leads to significant changes in the pulmonary circulation, which is caused by hypoxia. Scientists [2–8] have shown that pulmonary hypertension, which develops in these conditions, is a protective mechanism that improves blood circulation in the lungs. However, changes in ventilation and blood flow in the lungs under conditions of mountain hypoxia are attributed [9] to the adaptive restructuring of lung function, and not to the process of regulation of hemodynamics by the gas composition of air.
Hypoxia is a significant risk factor for pulmonary artery remodeling and changes in pulmonary hypertension. L. Zang et al. [10] studied the role of JAK2 in vascular smooth muscle cell damage in the development of pulmonary arterial hypertension. It has also been shown [11] that macrophages can affect vascular wall remodeling by producing proinflammatory cytokines.
Changes in oxygen concentration significantly affect the growth of malignant cells and the possibility of their further metastasis. Scientist M. Reuter et al. [12] studied the response of vascular endothelial cells to hypoxia and their ability to influence the restructuring of the lung wall and the progression of metastases.
It has been studied [13] that a significant portion of the world’s population (about 350–400 million people) lives at an altitude of more than 1.5 km above sea level, and more than 100 million tourists annually climb high into the mountains (more than 2.5 km). Scientist R. Mallet et al. [14] studied the reaction of the cardiovascular system to staying in the mountains and analyzed the effect of hypobaric hypoxia on cardiovascular diseases. T. Stellingwerff et al. [15] investigated various ways to improve endurance and training quality in athletes in high-altitude conditions. In particular, he studied in detail the issue of changes in nutrition that would improve adaptation to hypoxia at low and moderate altitudes [16]. The effect of low pressure and oxygen deficiency on cognitive functions was studied in detail by Y. Li and Y. Wang [16].
After analyzing previous studies [1–16], it was concluded that the effect of hypoxia on the body of animals and humans has been repeatedly investigated works [10–14] have been devoted to the study of the effect of reduced oxygen concentration on the development of various diseases. The effect of hypobaric hypoxia on cognitive functions and nutrient absorption has also been comprehensively studied [15, 16]. It was analyzed which trace elements and in what quantities should be consumed by athletes for effective training and achievement of better results [15]. A multifaceted approach has been used to study the causes of changes in the lung vascular wall in hypertension [10–12]. At the same time, little information has been published on the effect of changes in body position in space on pulmonary circulation in high-altitude hypoxia and the ability of the body to adapt to these conditions. That is why the research aims to determine whether the change in body position in space relative to the vector of earth’s gravity affects hemodynamic reactions in the small circle of blood circulation on the plain and in high altitude conditions.
Material and methods
The research was conducted on 44 adults male Wistar rats, with an average body weight of 254±6.5 g and 210±6.1 g, which were kept in highland conditions for 60 and 150 days, respectively. The pre-imported animals (with an initial average body weight of 355±11 g) were housed in a warm room at an altitude of 3200 m above sea level (Tian Shan, Tuya-Ashu Pass). During the entire research period, the rats were on a normal diet. Immediately before the study, the animals were injected with the drug nembutal at a dose of 30 mg/kg intraperitoneally. During the experiment, some of the animals were transferred to artificial lung ventilation, for which purpose dithylin at a dose of 30 mg/kg intraperitoneally was used.
The control group of animals included 25 adults healthy male Wistar rats with an average body weight of 350±12 g and were housed on a plain (Novosibirsk, 164 m above sea level).
Electroplethysmograms, pulmonary artery, and airway pressures were recorded using a Siemens-Elemaelectromanometer.
The specific electrical resistance of the blood, hematocrit, and hemoglobin content was determined using general methods, and the number of red blood cells was counted using Picoscale P-4. The study was conducted in horizontal (lying on the back, on the right, and the left side) and vertical (first head up, then head down) positions. The moment of change in body position in space was recorded graphically. A special table was used, the angle of inclination of which was smoothly changed from 0 to 90 degrees at a constant level of phlebostatic pressure.
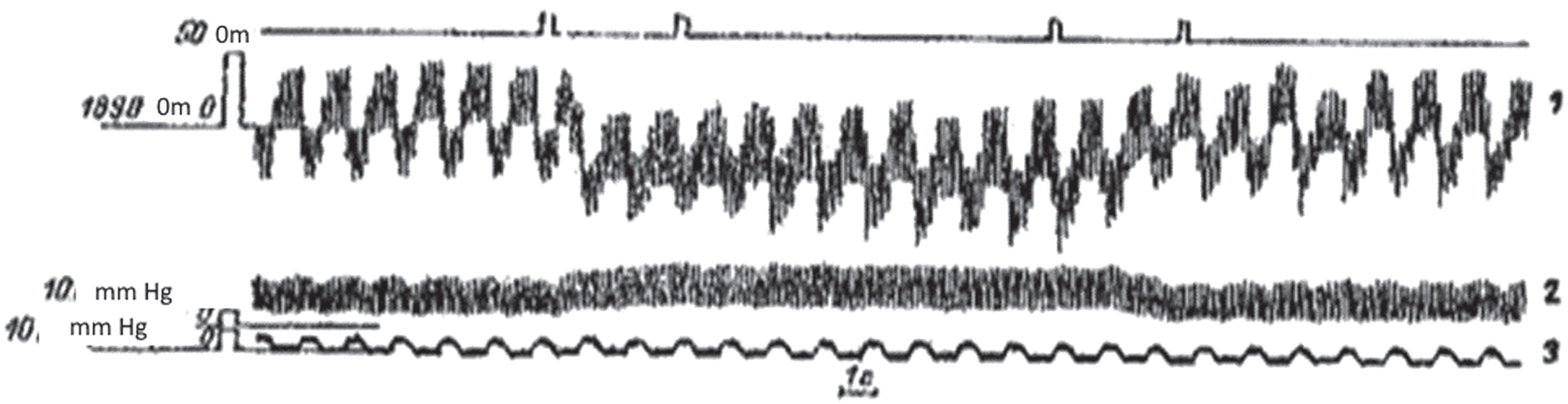
Pulmonary artery pressure was measured using a Siemens-Elema electromanometer by catheterization of the right jugular vein. Blood flow and blood filling were assessed by transbronchial electroplethysmography (in ml per 100 cm cubic lung volume) in conventionally selected lung lobes: apical, medial, and basal. In the medial and basal lobes, the dorsal and ventral surfaces of the lungs were considered (Fig. 1).

Recordings of electrocardiogram, electroplethysmogram, and pulmonary artery pressure curves. Note: 1 –electrocardiogram, 2 –electroplethysmogram, 3 –pulmonary artery pressure. Source: compiled by the authors.
The position of the electro plethysmograph sensor was monitored by X-ray examination in two projections: anterior and lateral (Fig. 2), as well as visually during the subsequent autopsy of the experimental animals.
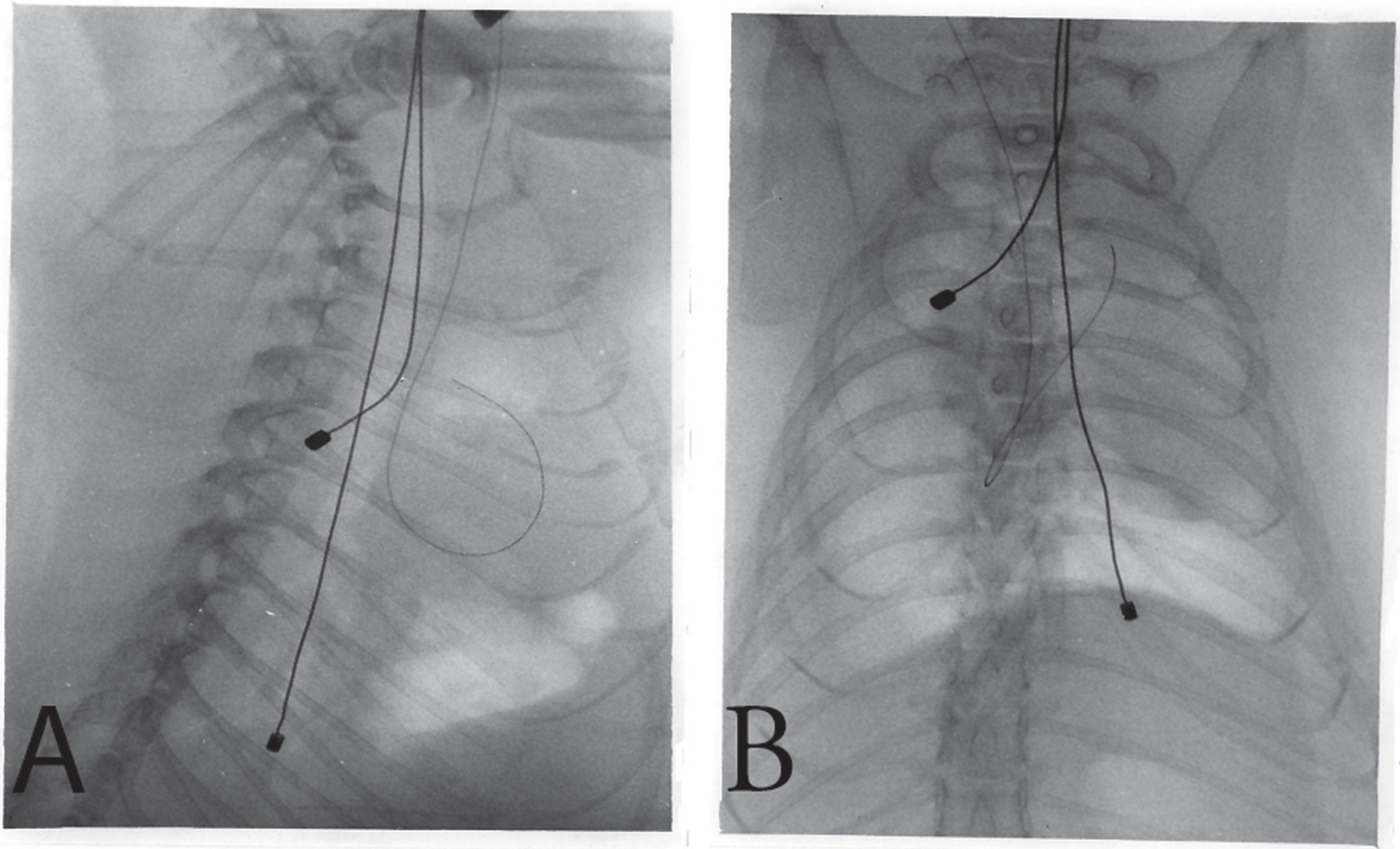
Exploratory radiography of the chest organs of experimental male rats. Note: In the presented radiograph of the rat chest in the direct (image A) and lateral (image B) projections, two electro plethysmograph probe sensors with electrodes at both ends are visible. In the area of the heart’s shadow, there is an X-ray contrast mandrel placed in the lumen of the catheter, the end of which is in the lumen of the pulmonary artery. Source: compiled by the authors.
The data obtained were statistically processed using Student’s t-test. Indicators obtained as a result of changes in body position in space were calculated as the corresponding percentage deviations compared to the baseline data. The results were statistically significant at the level of reliability (p < 0.05).
The rats were housed in a warm room at an altitude of 3200 m above sea level. This facility was equipped with controlled temperature, ventilation, and lighting to mimic the natural day-night cycle, ensuring the well-being of the rats. Electroplethysmograms, pulmonary artery, and airway pressures were measured using a Siemens-Elema electromanometer. This equipment would require calibration and maintenance to ensure accurate results. For the determination of specific electrical resistance of the blood, hematocrit, hemoglobin, and red blood cell count, standard laboratory equipment and a Picoscale P-4 were used. These stationed at a well-equipped laboratory, possibly at the base or a nearby research facility. X-ray examinations required radiography equipment to monitor the position of the electro plethysmograph sensor.
All research was carried out with consideration the Code of Practice for the Housing and Care of Animals Used in Scientific Procedures, American Association for Laboratory Animal Science and European Animal Research Association.
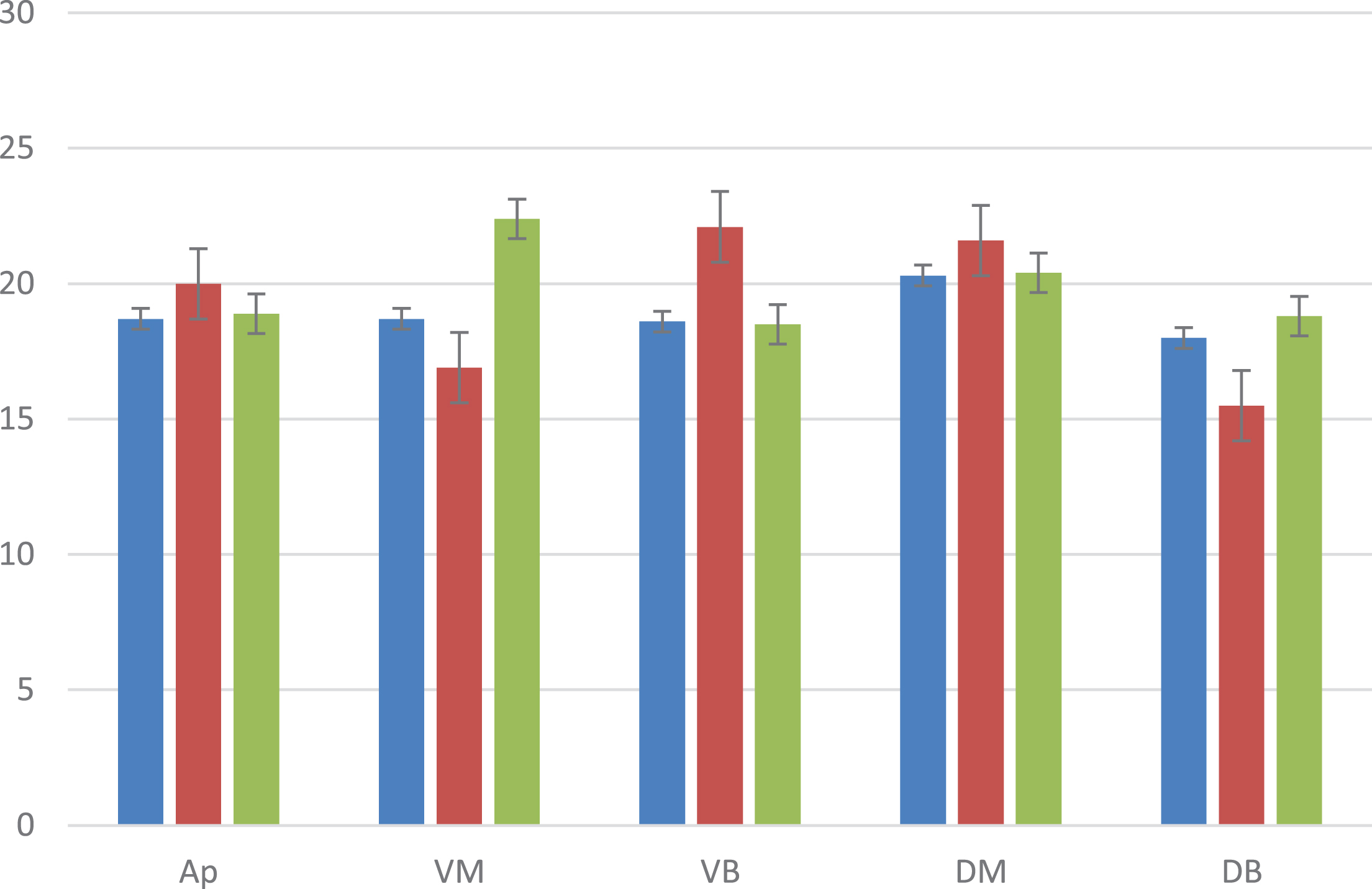
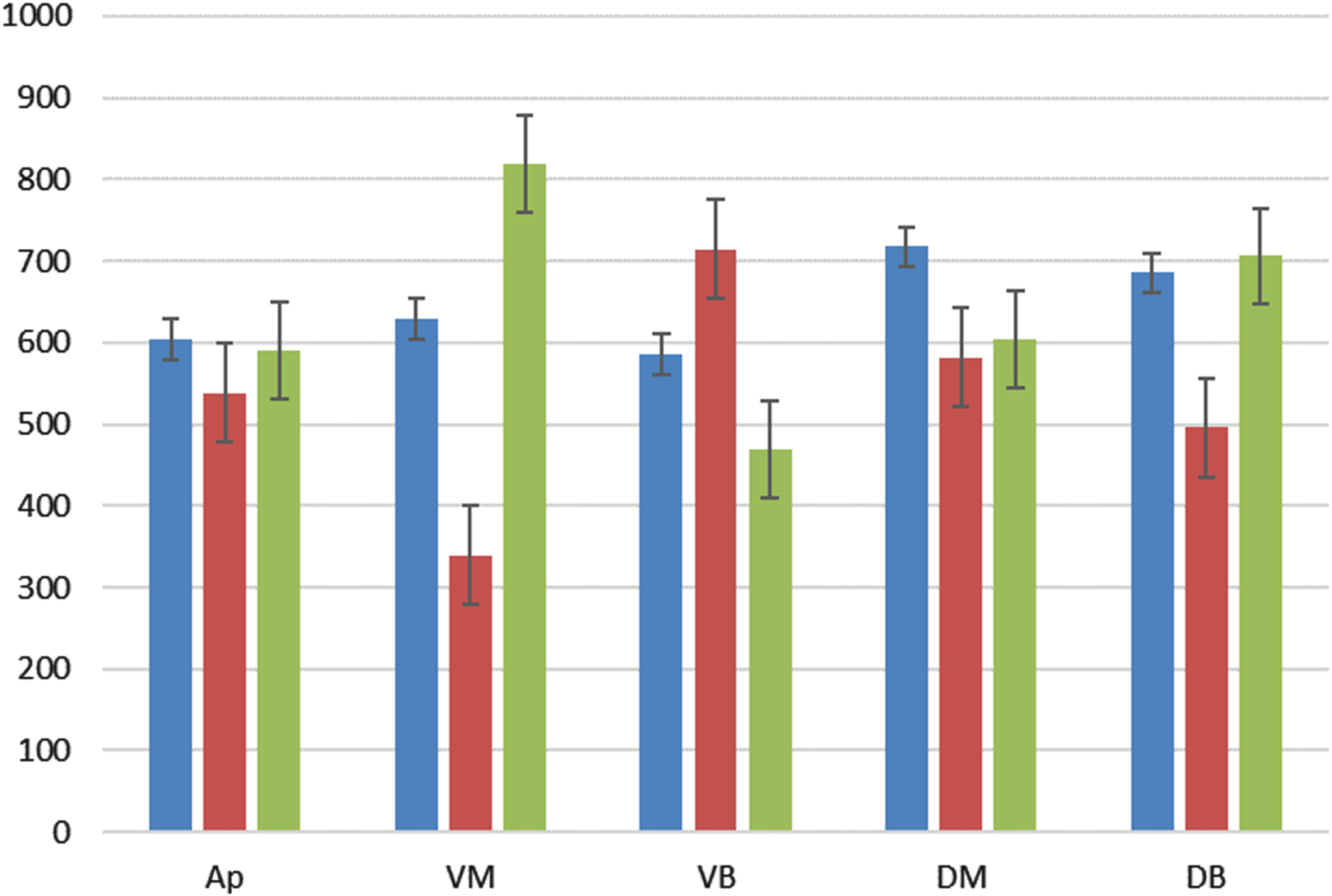
The research revealed that on the 60th day of adaptation to hypoxia in high altitude conditions, the same changes in blood filling were observed in the lung lobes of the same name, regardless of the position in which the animals were during the experiment: an increase in the anterobasal, posteromedial and apical regions, with a decrease in the posteromedial and anteromedial regions. The detected changes were statistically reliable. Changes in blood circulation had similar features. In the anteromedial, posterior-basal, and anterobasal areas, regardless of the position of the animal’s body in space, a decrease in blood circulation was noted. At the same time, in the anteromedial areas, a decrease in blood circulation was observed by 2 times or more. The increase in blood filling in the posteromedial areas was not significant (Fig. 3).

Average values of blood filling (Kv, ml/100 cm3) in different lobes of the lung in the horizontal position. Note: Ap –apical, VM –ventromedial, DM –dorsomedial, VB –ventrobasal, DB –dorsobasal. *blue –the first group; red –the second group; green –control group. Source: compiled by the authors.
The research revealed changes in the pressure in the femoral artery after a 2-month stay in the mountains (Table 1). Systolic blood pressure increased by 51%, and diastolic blood pressure remained unchanged. As a result, there was an increase in pulse pressure (on average by 79%). In the 5th month of the study, it was found that the indicators of blood filling and blood circulation in the mountains and on the plains were almost the same. However, the pressure in the pulmonary artery remained consistently elevated in the highlands (Fig. 4).
Indicators of pulmonary artery pressure, red blood counts, and body weight in rats at different periods of stay in high altitude conditions
Note: One * –p < 0.05, two ** –p < 0.01 compared to the control. All rats are at the age of 8–9 month. Source: compiled by the authors.

Pulmonary artery pressure curves and electroplethysmogram of rats at different periods of stay in the mountains. Note: a –3 days, b –60 days, c –150 days.1 –electrocardiogram, 2 –electroplethysmogram of the posterior basal lobe of the lung, 3 –pulmonary artery pressure. Source: compiled by the authors.
Rats that were horizontal on the plain (Fig. 3) showed no significant gravitational or other changes in blood filling and blood circulation in the study areas, except for a 24% difference between the anterobasal and posteromedial lung lobes. At the same time, changes in the above areas in the vertical position of the rats: head up and head down indicated gravitational differences.
Figures 5 and 6 show that when the animal’s position was changed from horizontal to passive orthotopic, there was an increase in blood filling in the anterobasal lobe of the lung, which gradually returned to baseline values after the end of the test (curve 1). At the same time, pulmonary artery pressure decreased (curve 2). The heart rate remained virtually unchanged. As a result of changing the position of the rat’s body to a passive anti-orthostatic position, a decrease in blood filling in the anterobasal lobe of the lungs was noted with a simultaneous increase in pulmonary artery pressure at a constant heart rate.

Response of hemodynamic parameters in the lungs due to changes in body position in space (passive orthostatic –90°). Note: 1 –electroplethysmogram of the anterobasal lung area, 2 –pressure in the pulmonary artery trunk, 3 –air pressure in the trachea. Source: compiled by the authors.
Response of hemodynamic parameters in the lungs due to changes in body position in space (anti-orthostatic +90°). Note: 1 –electroplethysmogram of the anterobasal lung area, 2 –pressure in the pulmonary artery trunk, 3 –air pressure in the trachea. Source: compiled by the authors.
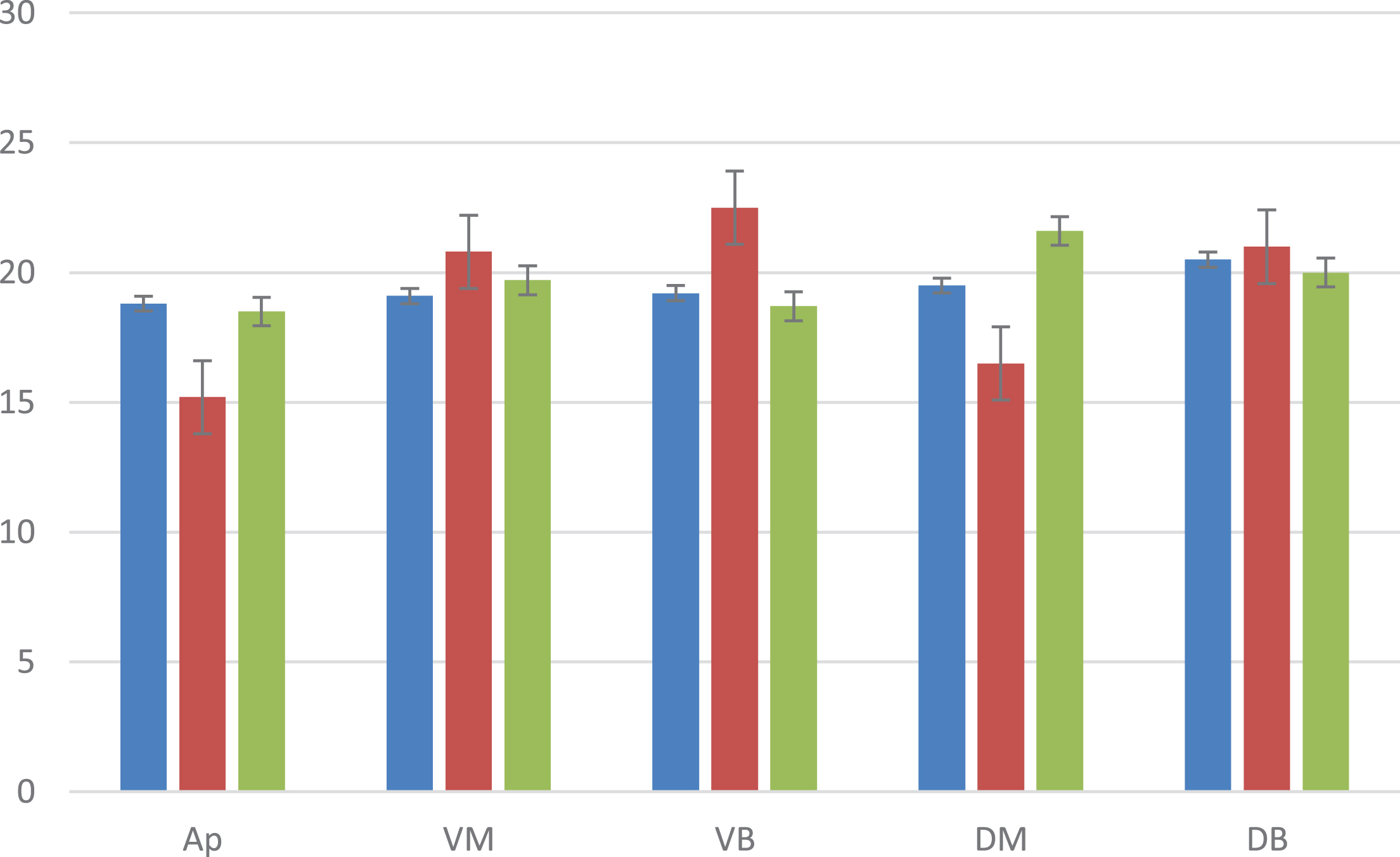
Figure 7 shows that on the plain (control group), during a passive change of position from horizontal to orthostatic, in all studied lung areas (except for the anterobasal lobes), blood filling decreased by an average of 4–5%, and in the anterobasal lobe it increased by 5%.
The average increase in blood filling in % (Kv, ml/100 cm3) in different parts of the lungs when changing the body position in space to vertical. Note: Ap –apical, VM –ventromedial, DM –dorsomedial, VB –ventrobasal, DB –dorsobasal. One * –p < 0.05, two ** –p < 0.01 compared to the control. Source: compiled by the authors.
After 60 days in the mountainous terrain, there were changes in blood distribution reactions in the apical and posteromedial regions in response to changes in body position in space. The blood filling decreased by an average of 2–4%; in the posterior basal lobe, it did not change; in the anteromedial and anterobasal lobes, it increased by 2.5–3.5%. Similar data were obtained on the 150th day of the study.
When the body position was changed to anti-orthostatic on the plain, changes in the blood filling of the lung lobes were detected in the apical (increased by 4.5%) and ventral (decreased by 3%) regions. In other areas, the reaction of decreased blood filling was weakly expressed (about 1%). Similar results were obtained after 150 days (Fig. 8).
The average increase in blood filling in % (Kv, ml/100 cm3). The reversed vertical position of the body (head down) in different parts of the lungs when changing the position of the body in space. Note: Ap –apical, VM –ventromedial, DM –dorsomedial, VB –ventrobasal, DB –dorsobasal. One * –p < 0.05, two ** –p < 0.01 compared to the control. Source: compiled by the authors.
In general, there was a positive correlation between blood circulation and blood filling. Similar changes in blood circulation and blood filling when changing the position from horizontal to orthostatic were noted on the plain and during 2 months of exposure to rats in the mountains. At 5-month exposure, blood flow did not change or increased by 7–10%, and blood filling decreased in 3 of 5 sites. Studies conducted after 5 months showed that when the body position was changed to an anti-orthostatic one, there was a smaller deviation in the average blood flow (from –6 to +6%) compared to changes on the plain (from –8 to +12%). When the position was changed from horizontal (supine) to the right or left side, blood flow and blood filling changed on the plain following gravitational mechanisms. In the left side position, the blood filling and blood flow in the left lung increased, while they decreased in the dorsal regions of the superior lungs. When the position was changed to the right side, a similar pattern was observed in the right lung. It was found that the same body positions in conditions of high-altitude hypoxia and on the plain led to the same results (Fig. 9).
The average increase in minute blood flow in % (CBF, ml/100 cm3/min) in different parts of the lungs with changes in body position in space. Upright position (head up). Note: Ap –apical, VM –ventromedial, DM –dorsomedial, VB –ventrobasal, DB –dorsobasal. One * –p < 0.05, two ** –p < 0.01 compared to the control. Source: compiled by the authors.
The change in pulmonary artery pressure at the time of the change in body position was visible both on the plains and in the mountains. In the plains, the transition to the passive orthostatic position was accompanied by a decrease in systolic and diastolic pressure, and the change in position to the passive anti-orthostatic position was accompanied by an increase in pulmonary artery pressure with approximately the same ratio of systolic and diastolic pressures (Fig. 4).
It was established that these reactions on the 60th and 150th day of stay in the mountains were almost identical, but differed from postural reactions on the plain by smaller changes in diastolic pressure in both orthostatic and anti-orthostatic positions. Therefore, the pulse pressure in the pulmonary artery during the change of position to orthostatic on the 60th and 150th day of adaptation decreased more clearly (by 22–39%) than the same on the plain (8%). When changing the position to anti-orthostatic, pulse pressure increased by 13% and 8%, respectively, and on the plain with the same test –by 8%. Thus, it was found that taking into account changes in pulse blood volume increase, the compliance of pulmonary vessels in rats with 60 and 150 days of adaptation is significantly lower than in the plain.
The research results corresponded to the general idea of regional unevenness of pulmonary circulation, following which the magnitude of the gradient in blood filling and blood flow in the lungs depends on the action of gravity and exists at any position of the body in space. However, when the rats were in a horizontal position (on their backs), both on the plains and in the mountains, no significant gravitational differences were found in either blood filling or blood flow (Fig. 10). This is probably due to the small anterior-dorsal distance in the rat lungs. Changing the position from horizontal to orthostatic or anti-orthostatic did not lead to significant changes in heart rate either on the plains or in the mountains, which distinguishes rats from larger animals and humans, in which changes in body position are accompanied by changes in minute circulation volume, primarily due to heart rate [15, 16]. In small laboratory animals, changes in the minute volume of blood circulation due to changes in body position occur due to changes in stroke volume, as demonstrated in Figs. 1 and 2 in the form of changes in the pulse amplitude of the electroplethysmogram, its decrease when moving to an orthostatic position and increase when moving to an anti-orthostatic position.

The average increase in minute blood flow in % (CBF, ml/100 cm3/min) in different parts of the lungs with changes in body position in space. Horizontal position (on the back). Note: Ap –apical, VM –ventromedial, DM –dorsomedial, VB –ventrobasal, DB –dorsobasal. Source: compiled by the authors.
Two mechanisms of blood flow and blood-filling reactions have been identified. The first is related to the outflow and inflow to the lungs from the vessels of the large circulation. It is based on the gravitational redistribution of blood mass. The second is the redistribution of blood mass inside the lungs due to the mechanism of gravity. This can be seen in the increase in blood filling and blood flow in the anterobasal areas of the lung during the transition to the orthostatic position (Figs. 3 and 4), in which, following the abovementioned, the amount of blood in the lungs should decrease, which happened, but in other areas. The phenomenon of blood flow distribution is more complex, as shown in Table 1 by the data on the topography of changes in blood flow and lung blood filling, and does not fit only into gravity schemes. Recently, there has been information about the differences in blood flow in the center and periphery of the lung lobes [4–8]. Based on the above (Figs. 5 and 6), it was concluded that a common feature of the lung response to high altitude conditions compared to the plains was a lesser severity of changes in blood filling and blood flow in the lungs after 60 and 150 days in the mountains. It has been shown [1] that in the pulmonary artery in high altitude conditions, diastolic pressure in rats remained virtually unchanged throughout the entire period of adaptation (3–300 days), while systolic pressure increased significantly. That is, it is systolic hypertension, which indicated an increase in the stiffness of the pulmonary vasculature, and not just an increase in peripheral resistance. Another piece of evidence was a decrease in vascular compliance with an increasing duration of stay in the mountains [1–7]. The data obtained on the decrease in the response of blood-filling changes to postural action after a long stay in the mountains is explained by an increase in the stiffness of the pulmonary vascular bed. At the later stages of stay in the highlands, the increase in vascular elasticity is explained by the mechanism of self-regulation according to Folkow [1], which occurs in response to prolonged pulmonary hypertension of the small circle of blood circulation. This was confirmed by morphological examination of the vessels. In the early stages of staying in the mountains, the mechanism of changes consisted of increasing vascular elasticity due to tension in the smooth muscle walls of the vessels.
The state of hypoxia can occur under several conditions: as a result of climbing mountains, the presence of various somatic diseases (obstructive apnea, acute and chronic diseases of the lungs and cardiovascular system, anemia), poisoning with a significant amount of toxic substances, and the ingress of foreign bodies into the respiratory tract. Staying in the highlands, where the atmospheric and partial pressure of oxygen is significantly reduced, leads to the development of hypobaric hypoxia [10].
T. Stellingwerff et al. [15] studied the impact of nutrition on improving adaptation to high altitude conditions in athletes. The researchers [15] concluded that training at high altitudes significantly increased the need for iron and calories. Namely, for optimal body functioning, it was necessary to increase the daily caloric intake by 300 kcal/day. To maximize the bioavailability of iron in conditions of reduced oxygen concentration, it is necessary to consider the individual characteristics of the regulation of the hormone hepcidin. It is responsible for the absorption and processing of iron by the body. To reduce the effects of oxidative stress on the body, it is necessary to consume foods rich in antioxidants. Li Yuan and Y. Wang [16] studied the effects of prolonged exposure to a high-altitude environment with insufficient oxygen on human cognitive function. Attention depression, short-term memory disorders, and general inhibition of reactions were noted. It was also concluded [16] that hypobaric and hypoxic environments affect the gut microbiome, and thus cognitive impairment can be reduced by using probiotics. The peculiarities of intestinal functioning at low pressure and oxygen content have been studied in more detail by scientists Y. Han et al. [13] and S. Ramos-Romero et al. [17] in separate independent studies. The following results were obtained from the experiments [17]: the combination of hypobaric hypoxia and low air temperature (4°C) led to an increase in hemoglobin and an increase in the number of red blood cells with leukocytes, and an increase in the concentration of enterobacteria. At the same time, the concentration of isovaleric and butyric acids in the contents of the cecum decreased. As a result of the change in intestinal microflora, the response of the immune system of the experimental animals changed significantly. This was manifested by an increase in the production of IgA and IgG, which prevented the entry, penetration, and further development of foreign microorganisms in the bloodstream. It has been analyzed [17] that the combined effect of cold and hypoxia prevented weight loss. At the same time, the isolated effect of hypoxia contributed to weight loss. This is explained [17] by a decrease in the ratio of Bacteroidetes: Firmicutes and the normalization of the concentration of Enterobacteriales and Lactobacteriales.
Tissue trauma with the subsequent development of hemorrhagic shock can cause hypoxia, inflammation, and anemia. A group of scientists led by L. Zang et al. [18] studied the effect of hypobaric hypoxia on hematopoiesis and spleen inflammation due to polytrauma. For this purpose, experiments were conducted on rats exposed to normobaric normoxia or hypobaric hypoxia for 18 hours. The results [18] indicated that muscle injury caused stress erythropoiesis regardless of pressure.
Scientists M. Brent et al. [19] studied bone density and mineralization in climbers. The study, conducted on rats, showed the following results: hypobaric hypoxia harmed femoral cortical bone; the negative effect on femoral trabecular bone was less pronounced. There was a decrease in bone strength of the middle diaphysis of the femur. In the femoral cortical bone, a decrease in bone proliferation and a decrease in the rate of bone mineralization were recorded. Thus, it was found [19] that exposure to hypobaric hypoxia contributed to a decrease in bone strength and femoral bone mass, while the manifestations of trabecular bone damage in the femur were significantly less. Accordingly, the skeletal response to hypobaric hypoxia differed between cortical and trabecular bones [19].
Under normal physiological conditions, healthy lungs are oxygenated. However, with the development of various diseases, lung tissue is damaged, ischemic, and secondary infection occurs. Normally, the respiratory system has natural barriers to detect and stop pathogens from entering the human body. One of the main components of these barriers is the epithelial tissue that lines the airways. It is capable of producing pro-inflammatory cytokines and chemokines in response to the development of an inflammatory response. L. Page et al. [20] studied the effect of hypoxia on the rate and possibility of pathogen development in the airway epithelium. The results [20] showed that chronic oxygen deficiency leads to a decrease in mucociliary clearance, deterioration of the epithelial barrier, and impaired nutrient absorption. M. Stembridge et al. [21] evaluated the response of pulmonary vessels to hemodilation in acute normobaric and chronic hypobaric hypoxia in lowlanders and permanent hypobaric hypoxemia in indigenous people of the Andes. It was found [21] that with a decrease in the concentration of red blood cells, there was an increase in vasoconstrictor effects in lowlanders. It was noted that hemodilution reduced pulmonary vascular resistance in highlanders, but the compensatory increase in cardiac output after hemodilution left the pulmonary artery systolic pressure unchanged.
Changes in oxygen concentration can significantly affect the growth rate of malignant cells and their ability to metastasize, as well as the behavior of somatic cells [22]. In their study on rats, M. Reiterer et al. [12] found that acute hypoxia increased the number of metastatic lung tumors caused by HIF-1α-dependent endothelial cell death and increased microvascular permeability. It was also found [12] that chronic hypoxia, on the contrary, delayed the growth of tumor cells to levels similar to those observed in normoxia. The removal of endothelial HIF-2α led to an increase in the vulnerability of the lung environment to the spread of tumor cells. Following this [12], it was found that the response of endothelial cells and the rate of tumor cell proliferation depended on the nature of hypoxia.
Thus, the analyzed data [10, 15–22] indicated that exposure to acute or chronic oxygen deficiency at low atmospheric pressure significantly affected all body systems. Exposure to hypoxia in high altitude conditions changed the activity of the digestive system, causing an increase in daily energy expenditure and a decrease in iron absorption [15]. There were also changes in the ratio of intestinal bacteria, which negatively affected immunity [13, 17]. Studies [16] have confirmed that prolonged exposure to low oxygen conditions significantly impaired cognitive function, deteriorated the ability to perceive and memorize new information, and caused sleep problems. Changes in hematopoiesis consisted of an increase in hematopoiesis [17, 18], and in bone tissue, a deterioration in the mineralization of certain areas was noted [19]. With chronic oxygen deficiency, there was a decrease in the protective mechanisms of the airway epithelium [20]. Scientist M. Stembridge et al. [21] noted that in the indigenous inhabitants of the highlands, the systolic pressure of the pulmonary artery remained within the physiological parameters due to a compensatory increase in cardiac output. Following the results of this study, it was found that the redistribution of blood filling due to gravity was less pronounced in the mountains. This was explained by an increase in the stiffness of the vascular wall of the pulmonary arterial bed, and, accordingly, an increase in the reactive component of hydraulic resistance. When changing the position of the body, the pressure in the pulmonary artery changed equally in the plains and highlands. Taking into account the changes in pulse pressure, it was found that the compliance of the pulmonary artery vessel wall in rats exposed to the mountains was significantly lower than in the control group. It has been shown that the increase in pulmonary artery pressure was a compensatory mechanism and occurred due to an increase in the stiffness of the pulmonary vascular bed.
Hypoxia’s influence on bodily systems has been explored extensively. J. Wang et al. [23] examined cerebral hemodynamics in neonates with hypoxic-ischemic encephalopathy, shedding light on age-specific differences using arterial spin labeling imaging. J. Zhu et al. [24] compared the effects of chronic intermittent versus continuous hypoxia on vascular endothelial function and myocardial contractility, highlighting the distinct responses based on hypoxia patterns. M. Lichtenauer et al. [25] delved into the cardiovascular impacts of moderate altitude, revealing potential therapeutic strategies against altitude-induced cardiovascular issues. C. Jung et al. [26] emphasized the central importance of microcirculation during hypoxic conditions, describing it as the battlefield for oxygen at the tissue level. Lastly, B. Hiebl et al. [27] established critical hematocrit and oxygen partial pressure values in the beating heart of pigs, offering insights for managing compromised oxygen conditions.
In summary, these studies accentuate hypoxia’s multifaceted effects, ranging from cerebral hemodynamics in neonates to cardiovascular responses in adults, highlighting the importance of understanding hypoxia for clinical purposes [28, 29].
Conclusions
Thus, the research results overall coincided with the ideas of regional blood circulation irregularities in the lungs, following which the magnitude of the gradient of blood filling and blood flow in the lungs is determined by the action of the earth’s gravity and exists at anybody position. At the same time, in the horizontal position of the rat body (lying on the back) and in the conditions of highlands and plains, no significant gravitational differences in blood filling or blood flow were found. As a result of the research, it was determined that the gravitational redistribution of blood filling and blood flow in the lungs was more pronounced on the plains than in the mountains. This is caused by an increase in the stiffness of the vascular wall of the pulmonary arterial bed, and, accordingly, an increase in the reactive component of hydraulic resistance. The change in pressure in the pulmonary artery at the time of the change in body position was visible both on the plain and in the mountains. In the flat terrain, the change in the body position of the experimental rats to passive orthostatic was accompanied by a decrease in systolic and diastolic (in percentage terms) blood pressure. At the same time, when the position was changed to passive anti-orthostatic, an increase in pulmonary artery pressure was noted with approximately the same ratio of changes in systolic and diastolic blood pressure. It was found that taking into account changes in pulse blood volume growth, the compliance of the pulmonary artery vessel wall in rats with 60 and 150 days of adaptation to high altitude conditions was significantly lower than in the control group. It has been shown that the increase in pulmonary artery pressure was a compensatory mechanism and occurred due to an increase in the stiffness of the pulmonary vascular bed. The research utilized an orthostatic test and found that it is an adequate test for studying pulmonary hemodynamics. The research results have improved the understanding of the mechanisms of pulmonary hypertension in high-altitude hypoxia. They can be used to develop effective treatments for diseases sensitive to changes in oxygen concentration.