
Abstract
OBJECTIVE:
To explore the prognostic impact of contrast-enhanced ultrasound (CEUS) features for initially unresectable colorectal liver metastases (CLMs) in a clinical setting of conversion therapy.
METHODS:
Between March 2015 and November 2020, consecutive patients with CLMs who received conversion treatment were prospectively enrolled. All participants underwent liver CEUS at baseline. The primary endpoint was conversion resection rate (R0 and overall resection). Secondary endpoints were objective response rate (ORR), overall survival (OS), and progression-free survival (PFS).
RESULTS:
104 participants who completed conversion treatment were included. CEUS enhancement pattern was correlated with index lesion (size and echogenicity), primary (site, differentiation, perineural invasion, and RAS genotype) and serum (CA19-9 level) characteristics (P = <0.001–0.016). CEUS enhancement pattern was significantly associated with R0 resection rate, ORR, PFS, and OS (P = 0.001–0.049), whereas enhancement degree was associated with PFS and OS (P = 0.043 and 0.045). Multivariate analysis showed that heterogeneous enhancement independently predicted R0 and overall resection (P = 0.028 and 0.024) while rim-like enhancement independently predicted ORR and OS (P = 0.009 and 0.026).
CONCLUSION:
CEUS enhancement pattern was significantly associated with tumor characteristics and clinical outcomes following conversion therapy, and thus might be of prognosis impact for initially unresectable CLMs.
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide and is ranked second in cancer mortality [1]. Liver is the most frequent site of CRC metastases, with 15% –25% of patients having synchronous liver metastases (LMs) at diagnosis and a further 30% developing metachronous LMs [2]. For patients with liver-limited metastases, when complete removal of LMs can be achieved, the reported 5-year-survival rates can reach 55% [3]. Unfortunately, <20% of patients are surgical candidates at diagnosis [4]. Over the past decade, systemic therapy has been reported to downsize LMs and facilitate secondary resection [5, 6]. Although survival times are slightly shorter for those patients who undergo secondary resection than for those patients with initially resectable LMs, they are far better than if resection was not carried out at all [7]. The survival benefits of secondary resection have led to the introduction of conversion therapy (following hepatectomy after responding to systemic therapy) into clinical practice [8].
Contrast-enhanced ultrasound (CEUS) is a useful modality for detection and characterization of LMs [9, 10] and a valuable addition to contrast-enhanced CT for CRC staging [11]. However, metastatic colorectal cancer (mCRC) is a heterogeneous disease, and colorectal LMs (CLMs) have various arterial enhancement presentation compared with hepatocellular carcinoma on CEUS [12, 13]. We therefore hypothesized that the diverse enhancement appearance might reflect tumor heterogeneity and have impact on clinical outcomes. To test this hypothesis, a prospective observational study was performed to correlate CEUS features and tumor characteristics in the conversion setting for initially unresectable liver-limited mCRC. We then tested the CEUS features with clinical outcomes. Both the CEUS features and tumor characteristics were evaluated with these outcomes.
Methods
This prospective study was approved by the institutional ethics review board (No. B2015-335R) and informed consent was obtained from every patient.
Patient eligibility
Previously untreated patients with histologically proven CRC and upfront unresectable synchronous liver-confined metastases were eligible. LMs resectability was determined using 3 criteria: ability to obtain a negative margin; preservation of 2 contiguous hepatic segments and≥30% liver remnant; and preservation of adequate vascular inflow and outflow as well as biliary drainage. Unresectability was defined as not meeting any of these criteria. Other inclusion criteria were age≥18 years; resectable primary tumor; ≥1 measurable tumor; Eastern Cooperative Oncology Group performance status of 0–1; life expectancy≥3 months; and adequate hematological, hepatic, and renal function. Patients with other cancers within 5 years were excluded. Patient recruitment was conducted by a local multidiscipline team (MDT), which included colorectal and liver surgeons, oncologists, radiologists, and physicians in related fields. Baseline evaluations consisted of colonoscopy, RAS and BRAF genotyping of biopsy specimens, abdominopelvic and thoracic contrast-enhanced CT, upper abdominal contrast-enhanced MRI, pelvic MRI (especially for rectal cancer), PET/CT, and standard clinical laboratory work-up.
CEUS
CEUS exams were performed on an iU22 (Philips, Bothell, WA, USA) scanner equipped with a C5-1 convex transducer (frequency range, 1–5 MHz) by one of 4 radiologists experienced in CEUS (≥3 years of experience). Conventional ultrasound was performed first and an index lesion in each patient was chosen for CEUS by the examiner, according to 3 criteria: maximum or center slice of the lesion in the scan plane; adjacent parenchyma in the field of view for comparison; and largest lesion meeting the above 2 criteria should be the first option. After adequate identification and observation of the index lesion with conventional ultrasound, the probe was held still while the scanner was switched to contrast harmonic imaging mode with a mechanical index < 0.1. The imaging settings, such as gain, depth, and focus were optimized. Generally, it was preferable to image in the longitudinal (sagittal or coronal) plane to keep the breathing movement within the scan plane. CEUS was performed after intravenous injection of 2.0 mL SonVue (Bracco, Milan, Italy) followed by 5.0 mL saline. A timer was started to coincide with the contrast agent injection. When the lesion began to exhibit enhancement, the patient was asked to maintain quiet breathing and a 90-second sequence was subsequently recorded at the level of the index lesion.
All images and cines were assessed independently by 3 radiologists (4–10 years of experience in CEUS) and features of the index lesion were abstracted, including size (maximum diameter) and echogenicity (hyper- or hypoechogenicity relative to liver parenchyma) on conventional ultrasound, and enhancement pattern (rim-like, homogeneous, or heterogeneous) and enhancement degree (hyperenhanced or non-hyperenhanced relative to liver parenchyma) on CEUS. The lesion was classified as non-hyperenhanced if it exhibited no hyperenhancement across the arterial phase. Any discrepancies among the radiologists were resolved by consensus review.
Treatment
All patients received mFOLFOX6 plus either cetuximab or bevacizumab by RAS genotype once every 2 weeks. The treatment was continued until tumor response indicated suitability for hepatectomy, disease progression, unacceptable toxicity, or a total of 12 treatment cycles. Once completely recovered from hepatectomy, patients resumed the same treatment up to 12 cycles. Perioperative and subsequent treatments were managed by the MDT.
Tumor characteristics
Clinicopathologic data were collected from baseline evaluation, histopathological assessment of the primary cancer, and operation notes.
Efficacy evaluation and follow-up
The primary endpoint was conversion resection rate (R0 and overall resection), assessed by the MDT every 2–4 treatment cycles up to 12 cycles. Local ablation was only allowed for lesions with an unfavorable location (a suboptimal surgical approach), and two-stage resection to achieve tumor clearance was also permitted. Postoperative tumor assessment was performed via MRI within 4 weeks.
Secondary outcomes included objective response rate (ORR), overall survival (OS), and progression-free survival (PFS). Tumor response was assessed according to RECIST version 1.1 [14]. The total number of complete (CR) and partial response (PR) was reported as the ORR. PFS was measured from the onset of conversion therapy to the date of progressive disease (PD), recurrence, or death. Patients without the abovementioned events were censored at the last tumor assessment date. OS was calculated from the date of patient recruitment to death from any cause or the date of last follow-up.
Statistics
Patient baseline characteristics and disease factors were summarized using descriptive statistics. Categorical variables were compared using χ2 or Fisher’s exact tests. Interobserver agreement of CEUS features was analyzed by determining the intraclass correlation coefficient (ICC). Conversion resection rate and ORR were analyzed using χ2 tests and univariate and multivariate logistic regression analyses. OS and PFS were assessed using Kaplan-Meier analyses with log-rank tests and univariate and multivariate Cox regression analyses. Analyses was performed by SPSS 19.0 (IBM, Armonk, NY, USA). Two-sided P < 0.05 was considered statistically significant.
Results
Baseline patient characteristics
From March 2015 to November 2020, 106 consecutive patients (mean age, 58 years±10.3, 79 men) were enrolled. Of these, 2 patients were considered early dropouts. Patient 1, who received 3 cycles of treatment, refused further therapy. The other patient, who received 10 cycles of treatment, died of severe pneumonia. Thus, the evaluable population consisted of 104 patients (Fig. 1). The cutoff date for survival data was July 2022, with a median potential follow-up time for the entire cohort of 37 months (range, 5.0–86.0 months).

Flowchart of participant inclusion and dropout.
Among the patients analyzed, 25 (24.0%) had rim-like enhancement in the arterial phase and the remaining 79 (76.0%) had non-rim-like enhancement, including 30 (28.8%) manifesting homogeneous enhancement, and the other 49 (47.1%) manifesting heterogeneous enhancement. Regarding enhancement degree, 91 (87.5%) exhibited hyperenhancement in the arterial phase, and 13 (12.5%) exhibited non-hyperenhancement. All cases showed hypoenhancement in the portal-delay phase.
There were 89 patients (85.6%) with consistency among 3 radiologists and 15 (14.4%) with inconsistency in enhancement pattern, while in enhancement degree there were 99 (95.2%) with consistency and 5 (4.8%) with inconsistency. The interobserver agreements for enhancement pattern and degree were good (ICC = 0.903 and 0.848, respectively).
Association between CEUS features and tumor characteristics
All analyzed patients were treated surgically for primary cancer. Of these, 46 (44.2%) underwent colorectectomy before chemotherapy, and the remaining 58 (55.8%) received surgery after treatment.
Two index tumor (size and echogenicity), 4 primary (site, differentiation, perineural invasion, and RAS genotype) and 1 serum characteristic (CA19-9 level) were significantly associated with CEUS enhancement pattern (P = <0.001–0.016; Table 1). Various tumor characteristics were evaluated together with enhancement degree, and no significant correlation was found between the imaging feature and tumor characteristics apart from patient age.
Correlation between clinicopathological characteristics and CEUS features
Correlation between clinicopathological characteristics and CEUS features
Data presented as No. (%). *Tumors located from cecal to two thirds of proximal transverse colon were classified as right-sided and the remaining one third of distal transverse colon to rectum as left-sided. A patient had two primary tumors sited in both left and right-sided locations and was classified as having LMs of indeterminate origin. Thus, the patient was excluded from analysis. CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19-9; LMs, liver metastases.
After resectability assessment by the MDT, 22 patients (21.2%) were determined to be eligible for R0 resection. Among these, a residual occult tumor adjacent to a portal vein branch was identified by MRI in one patient. Thereafter, a salvage local ablation was performed. So, the remaining 21 patients (20.2%) achieved actual R0 resection. Besides, tumor shrinkage indicated suitability for hepatectomy with adjunctive local ablation in 28 patients (26.9%). In addition to one-stage surgery, 3 patients (2.9%) underwent associating liver partition and portal vein ligation for staged hepatectomy (ALPPS), including one patient who received local ablation in stage I procedure. Ultimately, 53 patients (51.0%) underwent overall resection.
The CEUS enhancement pattern was significantly associated with R0 resection rate from the MDT (P = 0.029; Table 2). The overall resection rate tended to be higher in the heterogeneous enhancement group compared with the rim or homogeneous group, although the difference was not statistically significant (P = 0.059; Table 2). Further logistic regression analyses identified heterogeneous enhancement as an independent predictor of both R0 and overall resection (P = 0.028 and 0.024, respectively). Details of the univariate and multivariate analyses are shown in Table 3.
Correlation between clinical outcomes and CEUS features
Correlation between clinical outcomes and CEUS features
Data presented as No. (%) unless otherwise indicated. MDT, multidisciplinary team; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; ORR, objective response rate; PFS, progression-free survival; CI, confidence interval; OS, overall survival.
Univariate and multivariate analyses of clinicopathological factors associated with
MDT, multidisciplinary team; OR, odds ratio; CI, confidence interval; LMs, liver metastases; NA, not available.
Regarding the RECIST response, CR and PR were observed in one (1.0%) and 63 (60.6%) patients, whereas stable disease and PD was presented in the remaining 31 (29.8%) and 9 (8.7%) patients, respectively. Thus, ORR of the entire cohort was 61.5%.
The ORR was significantly related to the enhancement pattern (P = 0.002; Table 2; Fig. 2–4). The ORR of rim-like enhancement group was 32.0%, whereas that of heterogeneous and homogeneous groups were 71.4% and 70.0%, respectively. Further logistic regression analyses identified rim-like enhancement as an independent predictor of the worse ORR (P = 0.009). Other independent predictors were primary nodal stage, RAS genotype, and mucinous histology (P = 0.001–0.030). Details of the univariate and multivariate analyses are shown in Table 4.

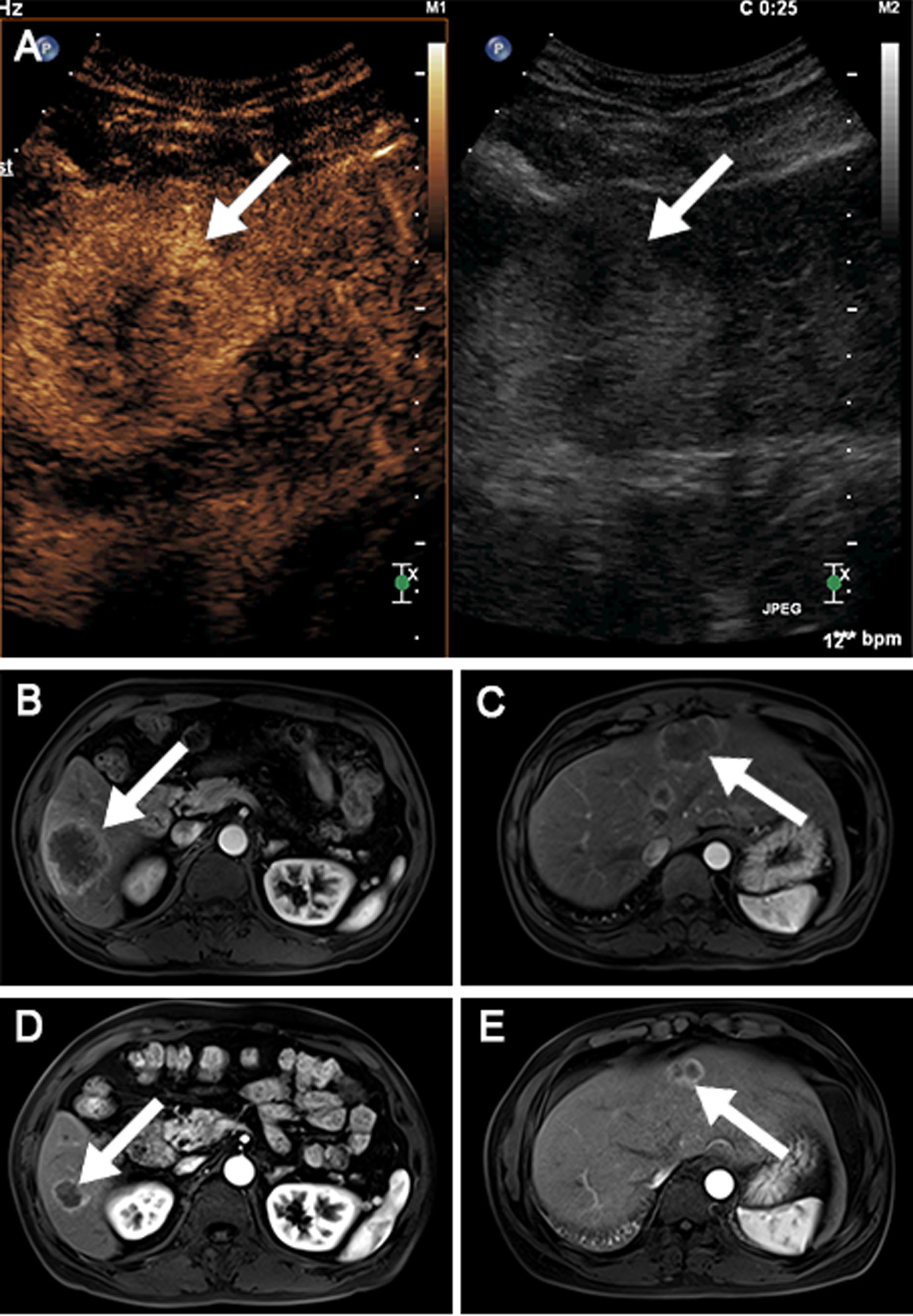
A 53-year-old female patient with well-differentiated RAS wild-type sigmoid colon cancer. A. The hyperechoic index lesion showed homogeneous hyperenhancement in the arterial phase. B, C. Multiple metastatic lesions were present in the liver at baseline. D, E. Partial response was radiologically documented after 4 cycles of mFOLFOX6 plus cetuximab treatment.
A 50-year-old male patient with well-differentiated RAS wild-type rectal cancer. A. The hyperechoic index lesion showed heterogeneous hyperenhancement in the arterial phase. B, C. Multiple metastatic lesions were present in the liver at baseline. D, E. Partial response was radiologically documented after 8 cycles of mFOLFOX6 plus cetuximab treatment.

A 33-year-old male patient with poorly differentiated RAS mutated colon cancer in the hepatic flexure. A. The hypoechoic index lesion showed rim-like hyperenhancement in the arterial phase. B, C. Multiple metastatic lesions were present in the liver at diagnosis. D, E. Disease progression was confirmed with substantial tumor enlargement after 4 cycles of mFOLFOX6 plus bevacizumab treatment.
Univariate and multivariate analyses of clinicopathological factors associated with objective response rate
OR, odds ratio; CI, confidence interval; NA, not available.
After a median follow-up of 37 months, 59 patients (56.7%) died and 91 (87.5%) experienced disease progression. For the entire cohort, the median PFS and OS were 12 months (95% confidence interval [CI]: 10.4–13.6) and 37 months (95% CI: 27.0–47.0), respectively. For the 53 patients underwent overall resection, the median PFS was 20 months (95% CI: 16.5–23.5) while the median OS was not yet reached.
OS differed significantly among 3 groups by enhancement pattern (P = 0.002; Table 2; Fig. 5A). The median OS of rim-like, heterogeneous, and homogeneous group were 24 months (95% CI: 17.9–30.1), 41 months (95% CI: 25.8–56.2) and 72 months (95% CI: 27.8–116.2), respectively. Regarding enhancement degree, the median OS were 38 months (95% CI: 21.6–54.4) in the hyperenhanced group compared with 26 months (95% CI: 11.0–41.0) in the non-hyperenhanced group (P = 0.045; Table 2; Fig. 5B). Univariate and multivariate regression analyses further confirmed a decreased OS in rim-like enhancement group (P = 0.026). Other independent factors were primary differentiation, perineural invasion (PNI), and CA19-9 level (P = 0.018–0.033). Details of the univariate and multivariate analyses are shown in Table 5.
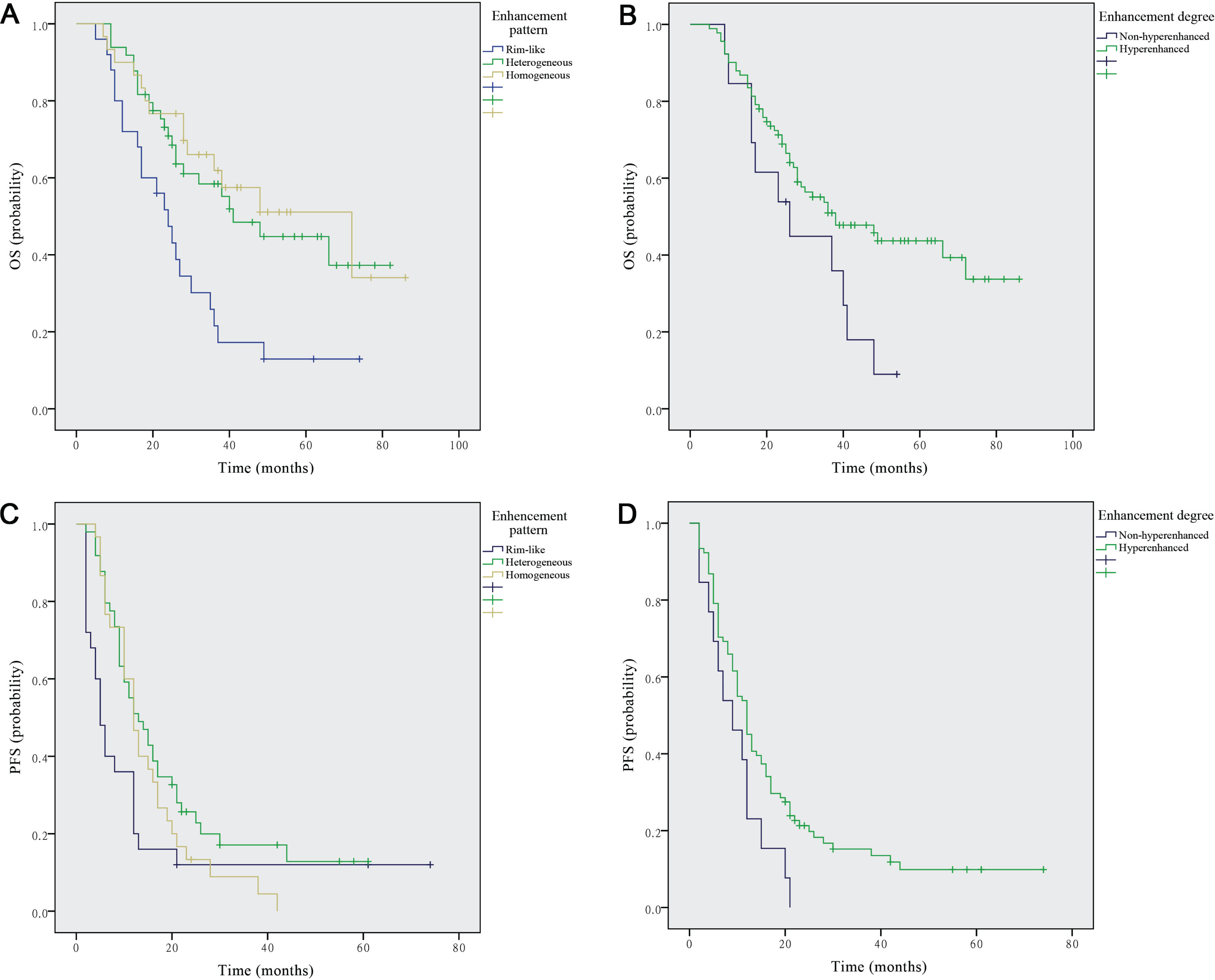
Survival analyses in patients according to CEUS features. A, B. Kaplan-Meier analyses of overall survival in patients according to enhancement pattern (P = 0.002) and enhancement degree (P = 0.045). C, D. Kaplan-Meier analyses of progression-free survival in patients according to enhancement pattern (P = 0.049) and enhancement degree (P = 0.043).
Univariate and multivariate analyses of clinicopathological factors associated with overall and progression-free survival
OS, overall survival; PFS, progression-free survival: HR, hazard ratio; CI, confidence interval; NA, not available; CA19-9, carbohydrate antigen 19-9.
Additionally, we evaluated the association between PFS and CEUS features. Regarding enhancement pattern, the median PFS of rim-like, heterogeneous, and homogeneous group was 5 months (95% CI: 3.0–7.0), 13 months (95% CI: 8.4–17.6) and 12 months (95% CI: 9.3–14.7), respectively (P = 0.049; Table 2; Fig. 5 C). Regarding enhancement degree, the median PFS was 12 months (95% CI: 10.0–14.0) in the hyperenhanced group compared with 9 months (95% CI: 3.1–14.9) in the non-hyperenhanced group (P = 0.043; Table 2; Fig. 5D). Multivariate analyses further demonstrated that RAS genotype, primary differentiation, and number of LMs were independent factors for PFS (P = 0.006–0.010). However, no CEUS feature rescored in the multivariate model. Details of the univariate and multivariate analyses are shown in Table 5.
The current results suggest that CEUS enhancement pattern of LMs is associated with tumor characteristics of the patient level, as well as the lesion level. Moreover, enhancement pattern and degree were correlated with clinical outcomes following conversion therapy, and enhancement pattern was identified as independent predictor of most endpoints.
At the lesion level, CEUS enhancement pattern was significantly correlated with tumor size, in line with a prior study [12]. Notably, the sizes of LMs exhibiting homogeneous and rim-like enhancement were considerably close, suggesting that enhancement pattern is determined only in part by tumor size. In addition, hypoechogenic LMs were more often manifested as rim-like or non-hyperenhanced compared with hyperechogenic lesions. One possible explanation might be that tumor vascularization not only correlates well with enhancement pattern or degree on CEUS, but also indirectly influences lesion echogenicity on non-enhanced ultrasound via ischemic necrosis within the lesion. At the patient level, higher CA19-9 levels and well to moderately differentiated primary tumors were more frequent in the heterogeneous or rim-like enhancement groups, while lower CA19-9 levels and poorly differentiated or undifferentiated tumors were more frequent in the homogeneous group. Interestingly, previous studies reported CA19-9 and tumor differentiation were also associated with apparent diffusion coefficient of rectal cancer on MRI [15, 16]. Moreover, LMs from RAS mutated or right-sided CRCs were more likely to exhibit rim-like enhancement, while those from RAS wild-type or left-sided tumors were more likely to exhibit homogeneous or heterogeneous enhancement. Similarly, a retrospective study showed that standardized uptake values of LMs on PET/CT were positively associated with KRAS mutation [17]. Of RAS genotype and primary site, the clinical significance has been widely recognized and incorporated into clinical practice guidelines for mCRC [11]. Besides, PNI was more prevalent in rim-like enhancement group. Till date, the mechanisms responsible for the correlations between enhancement pattern and tumor characteristics remain unclear. Nevertheless, our observations provided at least further knowledge on tumor characteristics associated with imaging features and in the future, basic science researches are warranted to clarify these correlations.
Previous publications have defined the correlations between tumor imaging features and other characteristics; however, little work looked at surgical conversion, which, if feasible, remains the only chance of cure for inoperable CLMs. For R0 resection, the conversion rate from MDT in our series was 21.2%, which was slightly lower than that of similar therapeutic regimens; conversion rate in the range of 22.3% –25.7% were reported in those studies [5, 18]. For overall resection, the conversion rate was 51.0%, which was comparable to the 49% in a previous report [18]. Despite local ablation and ALPPS were applied, only about half of the patients achieved successful conversion in our study. Accurate identification of these patients is thereby important, as they might benefit from the strategy. In our cohort, heterogeneous enhancement, number of LMs < 8, and unilobar LMs were each positively associated with R0 resection. Recently, a retrospective study also reported that number of LMs≤8 and unilobar LMs independently predicted successful conversion [19]. Furthermore, heterogeneous enhancement withstood the multivariate analyses for both R0 and overall resection. We know that for potentially resectable disease, systemic therapy can downsize LMs and facilitate secondary resection. Although heterogeneous enhancement was initially associated with larger tumor size in the current study, this group achieved the highest ORR and conversion rate. One possible explanation is that tumor size was the main reason for unresectability in this group. Staged hepatectomy triggering rapid liver remnant hypertrophy (ALPPS) also enables successful conversion for insufficient liver remnant [20]. During metastasectomy, intraoperative CEUS was also reported to locate further LMs which had not been identified in preoperative CEUS and/or MRI and surgical therapy was adapted accordingly [21]. Conversion therapy in clinical practice is thus complex, and further investigation of the reasons for unresectability, tumor response to chemotherapy, and operation ways may ultimately help to better anticipate the conversion outcome.
The probability of surgical conversion increases with ORR [22], and ORR following treatment is thus a significant endpoint for inoperable CLMs. Rim-like enhancement independently predicted a worse ORR in our cohort. Additionally, although enhancement pattern was correlated with tumor size and echogenicity, tumor size was not significant in the multivariate analyses and echogenicity showed null association with ORR. It therefore appears prudent to consider that the influence of enhancement pattern on ORR should not be attributable to tumor size or echogenicity. In the past decade, there is an increased move towards response prediction of CLMs from different imaging modalities as well, as advanced image postprocessing techniques are emerging. Reportedly, the wash-in and wash-out rates from CEUS and arterial enhancement fraction from CT were positively associated with ORR following chemotherapy [23, 24]. By contrast, the apparent diffusion coefficient from MRI and standardized uptake values from PET/CT were negatively associated with ORR [25, 26]. For treatment response monitoring, previous studies also reported that CEUS with perfusing software such as VueBox could be used for efficacy surveillance in antiangiogenic or local therapy [27, 28]. As becomes clear from the present study and prior publications, increasing evidence has shown that imaging features of LMs reflect tumor response to systemic therapy, despite the cause of which remains obscure. Unlike previous approaches however, CEUS enhancement pattern is a qualitative imaging feature, which could be easily obtained in a simpler and quicker way. And the imaging feature was reproducible, as shown by the good interobserver agreement among radiologists with varied experience. Furthermore, CEUS with targeted contrast agents such as BR55 was reported to enable reliable detection of CLMs > 0.8 mm and excellent visualization of tumor vascularity in a mouse model [29]. Its availability and advantages further suggest that CEUS enhancement pattern may be a promising tool for response prediction in CLMs.
Clinically, the ultimate therapeutic goal for this lethal disease is to achieve prolonged survival. The current multivariate analyses revealed a decreased OS in the presence of rim-like enhancement. Similarly, a prior study of intrahepatic cholangiocarcinoma also identified rim-like enhancement as an independent risk factor for shorter OS [30]. As seen in the multivariate model, other independent factors were primary differentiation, PNI and CA19-9 level, all of which are established prognostic factors for mCRC [31–33]. Moreover, the hazard ratio of enhancement pattern was comparable to that of other factors. Our findings suggest that patients with LMs exhibiting rim-like enhancement should be considered as a high-risk subcategory, which may help to better predict long-term survival in the specialized setting of conversion. Rim-like enhancement was also associated with shorter PFS, while the imaging feature did not withstand the multivariate analyses. As defined in the methods, PFS was measured from the onset of systemic therapy to the date of PD, relapse, or death. Of these, PD was mainly for the patients with failed conversion, whereas relapse was mainly for those with successful conversion. Therein lies the difference. In our results, 2/3 of the independent factors for PFS also scored in the multivariate model of conversion surgery, such as RAS genotype and number of LMs. And previous study demonstrated that conversion surgery conferred markedly superior PFS for patients with inoperable CLMs (median, 14.3 vs 8.3 months) [5]. Thus, the impact of conversion surgery may be underestimated in current study and in the future, treatment factors should be incorporated into analyses. Besides, hypoenhancement was associated with poorer OS and PFS in our cohort, in accord with a previous study of intrahepatic cholangiocarcinoma [34]. However, enhancement degree did not score in the regression analyses, which might be owing to the low frequency of the imaging feature.
This study had limitations. First, the index lesion selected for imaging interpretation is questionable, as we do not know whether the lesion is fully representative of CLMs. However, the results reported here tend to show that the selected lesion assessed by CEUS reflected tumor characteristics of the patient level rather than the lesion level alone. Second, LMs resectability in this study was inevitably influenced by local experience and the sample was small, therefore studies including multiple institutions and larger series are needed to verify our results. Third, it should also be noted that 55.8% of patients underwent colorectectomy after chemotherapy, and histopathological assessment of the primary cancer may be thereby no longer representative of the baseline characteristics. Finally, because of tumor heterogeneity and a common treatment strategy, we focused exclusively on tumor factors and did not include treatment factors.
Conclusion
Our study demonstrates that the enhancement pattern of LMs on CEUS was directly correlated with tumor characteristics and clinical outcomes following conversion therapy. Patients with heterogeneous enhanced LMs had a superior conversion rate, whereas those with rim-like enhanced LMs had worse survival. These findings suggest that the imaging feature might be of prognosis significance in patients with initially unresectable liver-limited mCRC.
Footnotes
Acknowledgments
We gratefully acknowledge the commitment of all participants involved in the study enabling this research to be conducted.