
Abstract
BACKGROUND:
Rapid evolution of ultrasound technology has allowed widespread use of handheld ultrasound devices (HHUDs) for many possible applications. Along with the adult population, the use of HHUDs for Point of Care Ultrasound (POCUS) in pediatric medicine has been increasing over the last few years. However, pediatric-specific literature is still scarce on mobile vascular ultrasound.
OBJECTIVE:
To evaluate diagnostic capabilities of Vscan Air™ in comparison with high-end ultrasound for the assessment of the internal jugular vein in children and adolescents.
METHODS:
42 Internal Jugular Veins (IJVs) of 21 pediatric patients were scanned by an experienced examiner using a WLAN-supported handheld ultrasound device (Vscan Air™) and high-end cart-based ultrasound (LOGIQ E9) as reference. B-Mode and Color-coded Doppler (CCDS) were performed and compared. Image quality was assessed using a score of 0 to 5 and statistically analyzed. Results were interpreted independently by two readers in consensus.
RESULTS:
21 patients (2–17 years; mean 11,00±4,5 years; female n = 11, male n = 10) were examined. The rating score never dropped below 3 for both devices. The median score evaluation of B-Mode and CCDS for the high-end device was 5.00, of Vscan Air™ 5.00 for B-Mode and 4.00 for CCDS. A significant difference was shown between the two devices in the evaluation of CCDS.
CONCLUSIONS:
Vscan Air™ ultrasound device allows sufficient assessability of the IJV in pediatric patients, opening up new possibilities for fast and mobile POCUS of cervical veins and potential guidance of central venous catheter placement.
Introduction
Rapid evolution of ultrasound technology has allowed widespread use of handheld ultrasound devices (HHUDs) for many possible applications, lately boosted by the COVID-19 pandemic [1–8]. They are location-independent, simple-to-use, ubiquitously applicable devices and much easier to disinfect than cart-based scanners. Costs are in general low compared to high-end devices. The portable and lightweight nature of HHUDs makes it an ideal modality for use in austere environments, disaster situations, and resource-limited settings without access to high-end imaging [9]. Along with the adult population, the use of HHUDs for Point of Care Ultrasound (POCUS) in pediatric medicine has been increasing over the last few years [3, 10–12]. In general, children are well suited for ultrasound examinations due to their body habitus. The lack of necessity of patient transport and sedation and the lack of radiation exposure are major advantages compared to other diagnostic tools used in pediatric imaging [13].
Ultrasound is considered the primary diagnostic method of choice in the peri-procedural assessment of the jugular veins [14]. Modern cart-based scanners allow a detailed and complete morphological and functional evaluation of the vein. However, considering the issues of hygiene, mobility and prompt accessibility especially in critically ill patients or out-of-hospital settings, a connection of the linear probe to the ultrasound unit via wire can limit the availability of sonographic examinations. Recently, increasingly powerful handheld devices have been developed [15]. At our institution, we use a pocket-size wireless scanner, Vscan Air™ [16]. This device combines the linear and convex probes, providing high resolution in a wireless transducer and enables image transmission via wireless LAN.
Literature is still scarce on specific pediatric vascular ultrasound using mobile devices. Our aim was to assess the IJVs of children and adolescents (under 18 years of age) compared to high-end ultrasound in a routine clinical setting.
Methods
This single-center, retrospective feasibility study evaluates whether handheld ultrasound with Vscan Air™ is comparable to standard cart-based ultrasound in assessing IJVs of pediatric patients and in estimating potential use of the HHUD for possible sonographic guidance of internal jugular catheter placement.
Consent for the retrospective analysis of images obtained by Vscan Air™ had been approved by the local ethics committee (Nr. 23-3347-104). All examinations performed using high-end ultrasound were part of standard patient care and served as reference.
Patients
A total of 21 patients (age range 2–17 years; mean 11,00±4,5 years; female n = 11, male n = 10) were included. All patients were referred to the pediatric radiology division at our hospital between January 2023 and May 2023 and underwent routine sonographic examinations of the head and neck region. Patients with known pre-existing anomalies of cervical veins or cervical venous malformations or with cervical tumors causing venous compression had been excluded.
Ultrasound examinations
All patients were examined by a board-certified pediatric radiologist with more than 15 years of experience in sonography. Non-contrast, conventional, cart-based high-end ultrasound was performed, immediately followed by an examination using handheld ultrasound (HHU), thus providing the same examination conditions where possible. Both the high-end device and mobile device were developed by the same manufacturer, so a comparability between the two devices could be assumed. Spectral Doppler with quantitative measurements was not available at the time of the investigation in VScan Air™ and therefore could not be compared.
Reference examinations
A linear multifrequency transducer was used (6–9 MHz, LOGIQ E9, GE Healthcare, USA). Solely non-contrast ultrasound was carried out. Images of IJVs in two planes on each side were stored digitally in our Picture Archiving and Communication System (PACS).
All patients were examined in supine position. Warm transmission gel was used for patient comfort. First, right IJV location and course were assessed from the skull base, at the jugular foramen, down to the upper thorax, at the level of venous confluence with the subclavian vein to form the brachiocephalic vein. The perivascular structures were examined for adjacent cervical tumors, such as compressing lymph nodes, vascular malformations, abcesses or thyroid nodules. IJV morphology was depicted by B-Mode in the transverse and longitudinal plane. Shape, wall thickness, echogenicity of lumen, respiratory variability and visibility of valves were observed. Compressibility of the vein was noted using intermittent compression sonography. Color-coded Doppler sonography (CCDS) was used next to verify antegrade venous flow; Color Doppler function was adapted to low flow using optimized gain and adjusted low pulse repetition frequency. Afterwards, the same procedure was used to assess the left IJV. In addition, the examination was extended using a convex probe in search of possibly causing intrathoracic pathologies.
Examinations with Vscan Air™
The linear probe (3–12 MHz) of the HHUD (Vscan Air™, GE Healthcare, USA) was used. The wireless scanner was WLAN-connected to a touchscreen tablet PC. A mobile iOS device was used on which the corresponding function app had been installed. The battery of the HHUD could be charged quickly on site using inductive charging. Battery capacity lasted for 50 minutes‘ scan time, sufficient for examining more than one patient. The obtained images were saved anonymously and password-protected on the used mobile device, in compliance with applicable data protection regulations. Then the same procedure was performed as described above using the HHUD. Settings for flow and depth were suitably adjusted.
Rating score image quality
Image quality was assessed using a score of 0 to 5: 0 = no evaluation possible (e.g., in case of patient movement/crying), 1 = no diagnostic evaluation possible, 2 = major limitations of diagnostic evaluation (no reliable assessment), 3 = proportionate limitations of diagnostic evaluation but sufficient for a reliable assessment (e.g. due to post-interventional edema), 4 = only mild limitations of diagnostic evaluation, 5 = excellent image quality without limitations.
Documentation of the results was performed in a proprietary Excel spreadsheet, also in compliance with the applicable data protection regulations.
Evaluation procedure
Data were evaluated and read in consensus off-line by two readers (one experienced with > 3000 examinations/year, > 30 years of experience in sonography, DEGUM III; the other with > 500 examinations/year, > 15 years of experience in sonography, certified pediatric radiologist) blinded to the examination date. Results of both techniques were compared.
Statistical analysis
The program IBS SPSS Statistics version 29.0.0.0 (241) was used for statistical analysis. The Gaussian distribution of the collected data was tested by Shapiro-Wilk test, and regarding the small number of cases additionally by histograms and Q-Q plot testing. In the absence of a normal distribution, a hypothesis test of the paired samples was carried out by a Wilcoxon test otherwise by a paired t-test. The Significance level was set to an α-value of 0.05.
Results
One 17-year-old male patient had been excluded because of a cervical lymphoma bulk compressing the IJV. The remaining 21 patients with 42 IJVs were included. 16 patients presented with acute or prior hemato-oncological diseases, 11 with status post stem-cell transplant (SCT). Non-hemato-oncological diagnoses included mild reactive lymphadenopathy, Zuelzer-Wilson disease, pleomorphic adenoma of the parotid gland, ataxia teleangiectasia and facial venous malformation (Table 1). Prior to this study, two patients had been diagnosed with thromboses of the left brachiocephalic vein following Hickman line placement (one patient in 2018 and the other in 2022); central lines had been removed and follow up care had shown no residual flow obstruction after anticoagulant therapy in both children. At the time of examination, no patient had a catheter inserted via the internal or external jugular, subclavian or brachiocephalic vein and none presented with thromboses of the IJVs. No patient showed anatomical variants of the cervical veins. In one patient presenting with a metastasized testicular malignant germ cell tumor, a thyroid nodule was incidentally detected by ultrasound (Fig. 1). Surgical specimen histology following thyroid lobectomy revealed a thyroid adenoma. Patients who showed only small, non-compressing cervical lymph nodes were included (Fig. 2).
Demographic data of the studied cohort
Demographic data of the studied cohort
f = female, m = male. SCT = stem cell transplantation, LAP = lymphadenopathy, MDS = myelodysplastic syndrome, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia.
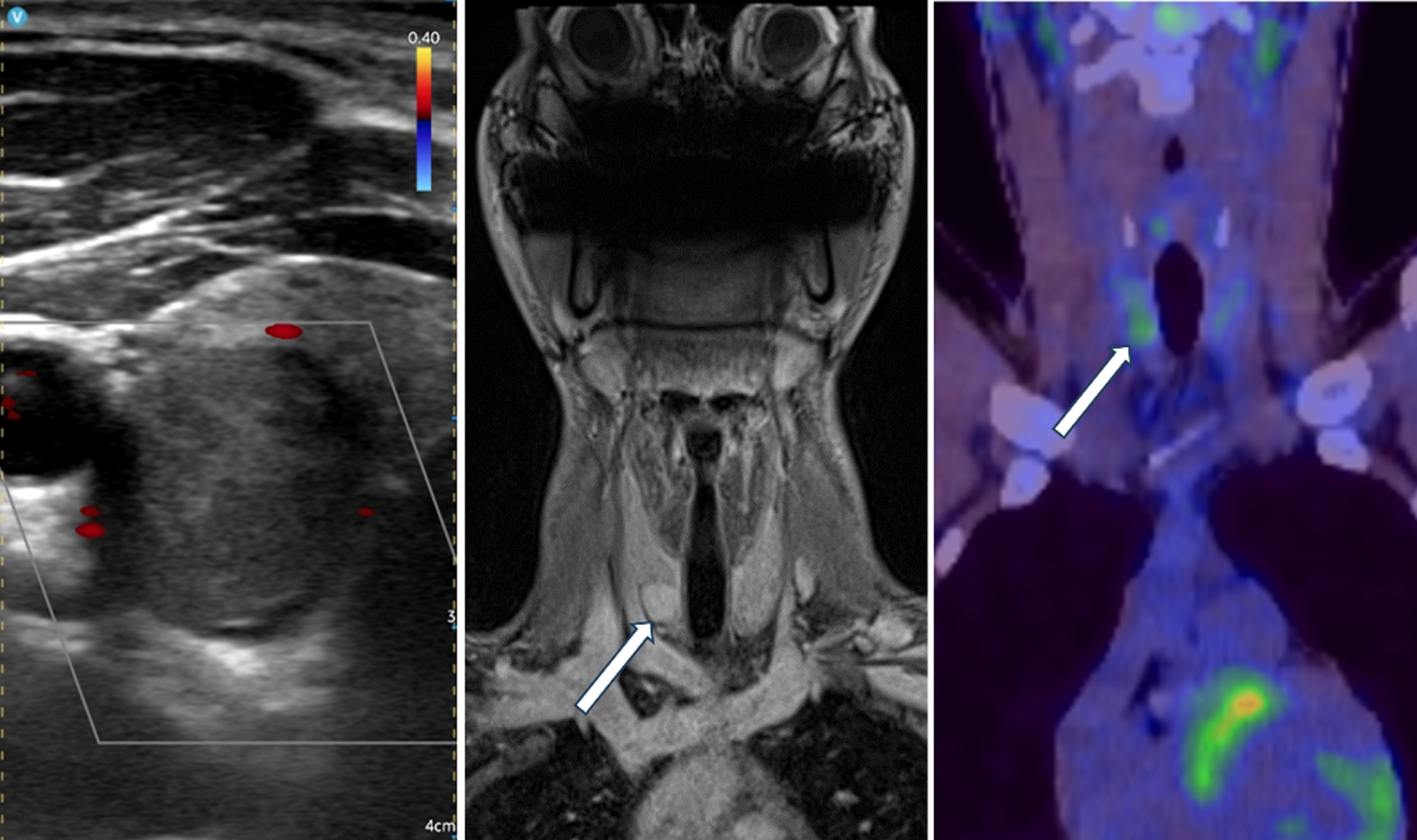
16-year-old male with an incidentally detected thyroid nodule (arrow) of the right lobe depicted by Vscan Air™ (left), contrast enhancing in MRI (middle) and PET-positive (right).
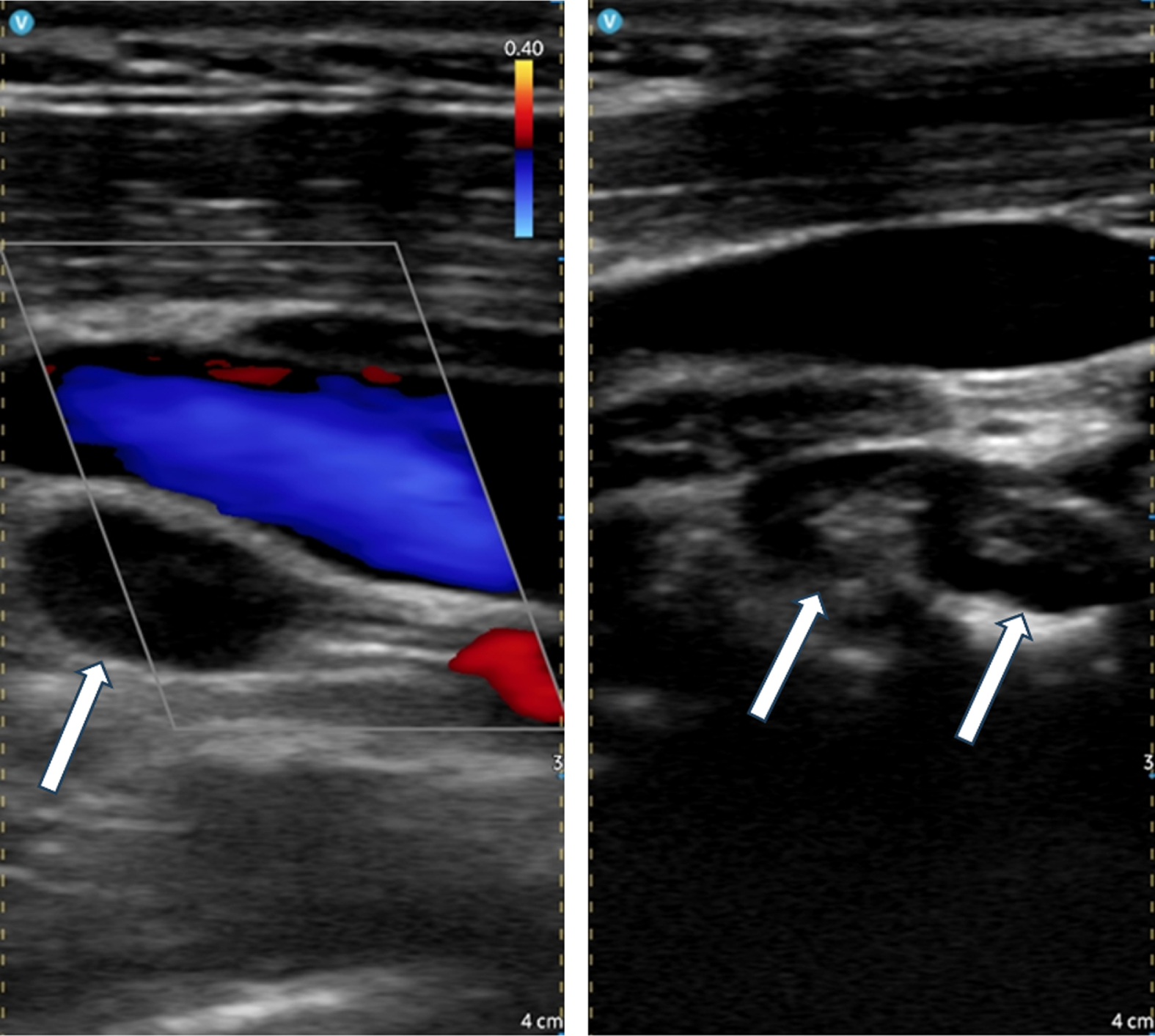
PET-positive (not shown), hypoechogenic lymph node (arrow) adjacent to the IJV in a 17-year-old girl with Hodgkin‘s disease (left) and small infection-associated lymph nodes with preserved hila (arrows) in a 3-year-old girl post SCT for ALL (right), pictured by Vscan Air™.
Using B-Mode, we found no difference between the HHUD compared to conventional high-end ultrasound (median 5.0 points with both devices). Vscan Air™ showed excellent image quality in IJV assessment (Fig. 3). Even in the older patients, no limitations due to depth blur or inhomogeneity occurred. Using CCDS, the HHUD showed slightly reduced image quality compared to high-end ultrasound (Table 2). Image quality achieved by Vscan Air™ was never less than 3 points (Fig. 4). With both devices, main limiting factor in IJV assessment was patient movement and crying, especially in Color-flow imaging.
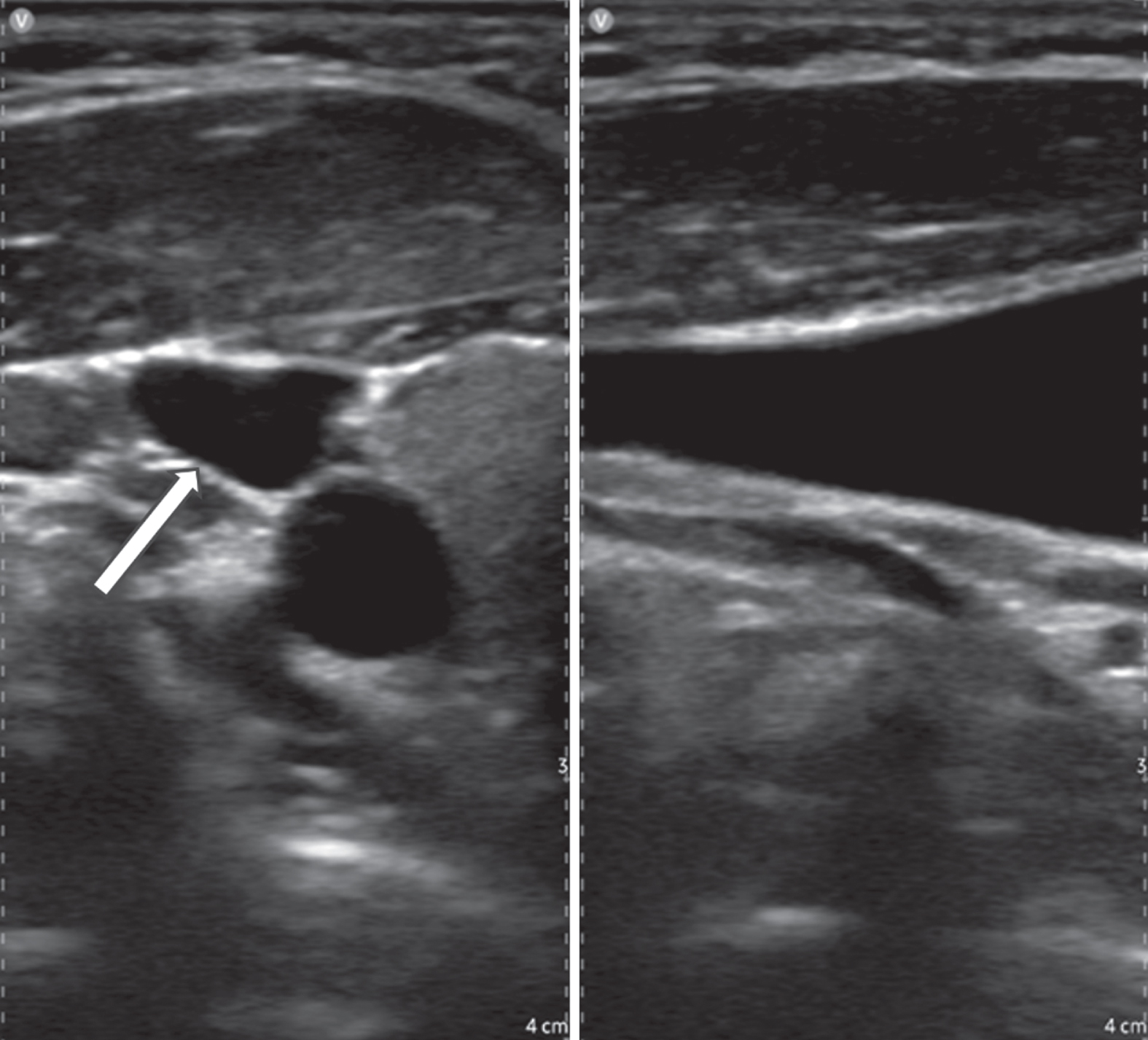
Image quality 5. Right IJV (arrow) in the axial plane (left) and longitudinal plane (right) in a 12-year-old boy with β-thalassemia.
Comparison of the evaluation score of the Vscan Air™ device and high-end device
CCDS = Color-coded Doppler sonography.
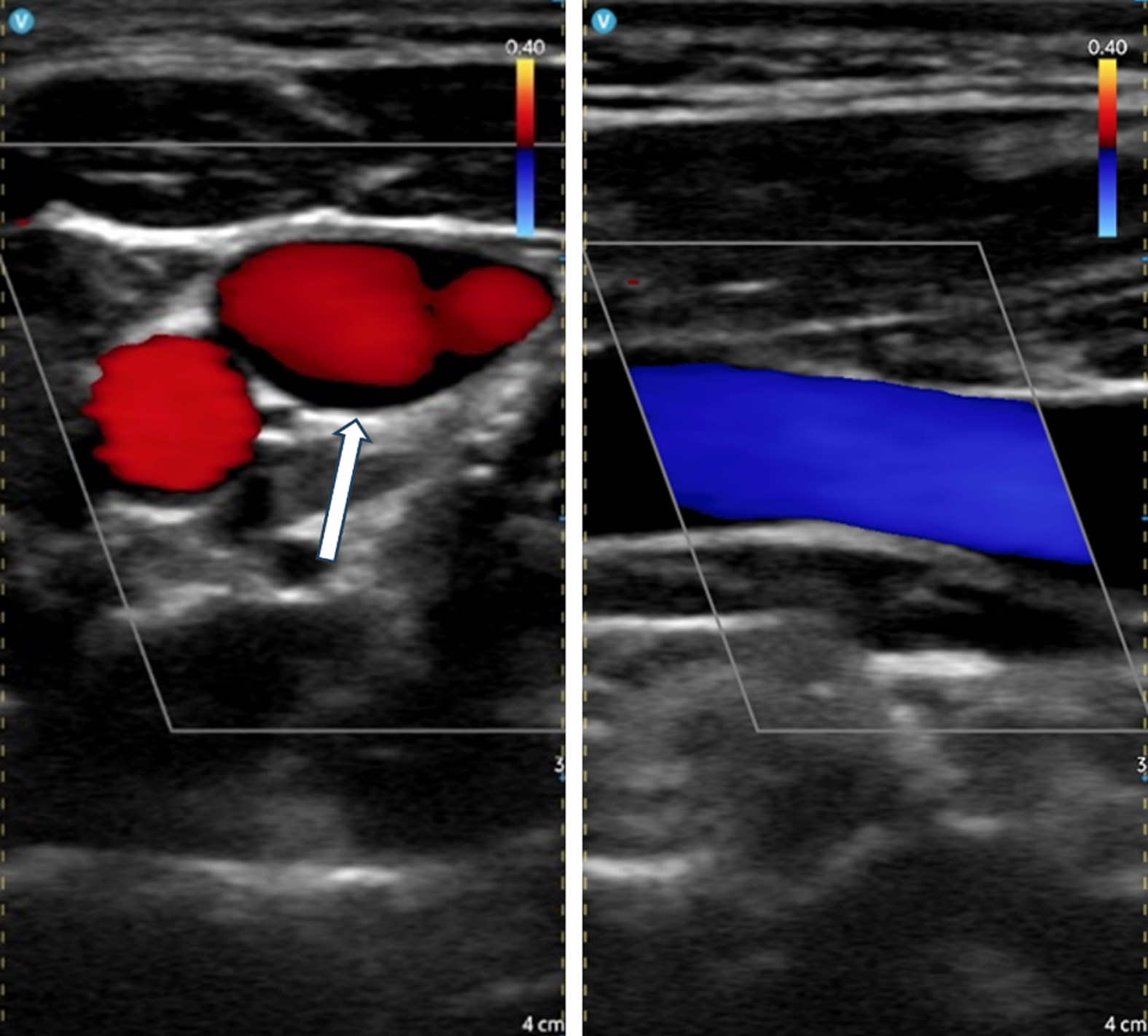
7-year-old boy with Rosai-Dorfman disease. Left IJV in the axial (left, arrow) and longitudinal plane (right) depicted with Vscan Air™ using CCDS. No relevant limitations present.
Central venous access provides a safe and effective form of vascular access in emergency and critical situations. The IJV as the major venous return from the brain, upper face and neck [17] is commonly used for central venous access in severely sick children and adolescents. International consensus recommendations advocate for the use of POCUS in pediatric vascular procedures, supported by pediatric-specific literature [18–20]. Ultrasound guidance significantly reduces the risk of cannulation failure and rate of arterial punctures in central venous catheterization in comparison with the anatomical landmark technique [21, 22]. Especially when dealing with critically ill children, ultrasound devices used for vascular catheterization need to be quickly accessible, simple to use and preferably easy to disinfect. Modern HHUDs can meet these requirements even in out-of-hospital-settings due to rapidly advancing ultrasound-related technology, particularly due to improved frequency ranges and screen resolution. Capacities of installed batteries suffice for adequate examination times. In addition, reliable image storage and safe data transfer have been made possible by modern IT-solutions, allowing security and privacy of patient data and thus the use of HHUDs in clinical routine. However, given the fact that current diagnostic capabilities of HHUDs are still limited, the obtained image quality needs to be reliably sufficient when compared to high-end ultrasound.
Limited probe options can be an important restriction on the use of HHUDs in pediatric imaging. A great advantage of Vscan Air™, the used device for our study, is its dual probe. The integrated multifrequency linear probe allows high-resolution imaging, which is an essential requirement for pediatric sonographic imaging.
To the best of our knowledge, this is the first study to evaluate the diagnostic usefulness of handheld wireless ultrasound for POCUS of the internal jugular vein in children and adolescents. Even though Vscan Air™ currently offers only a very limited range of pediatric-specific presets, our data indicate that the device allows assessment of IJVs in children and adolescents with sufficient diagnostic quality. Using B-Mode, the image quality achieved by Vscan Air™ proved to be the same as with high-end ultrasound, allowing detailed depiction of vessel anatomy and movement. Using CCDS, the obtained image quality showed to be moderately reduced, but still sufficient when compared to high-end ultrasound. The exclusion of IJV thrombosis could be made confidently in every patient, consistent with prior experience with Vscan Air™ [23]. Limitations of the image quality achieved by both devices were mainly patient-related, primarily due to movement and crying. Particularly the latter can impede Color-Flow imaging of cervical veins to a great deal. Overall, we found our patients not to be intimidated by the pocket-sized HHUD and being quite familiar with the connected smartphone, which was helpful in providing a relaxed examination atmosphere and reducing patient movement. The intuitive and unrestricted usability of Vscan Air™ in conjunction with high-resolution vascular images could provide possible ultrasound-guided placement of central venous catheters via the jugular vein. On the other hand, it could be difficult to place the screen while scanning respectively puncturing.
This monocentric study is limited by the small number of patients. The youngest patient of the cohort was two years old; no under 1-year-olds, who show particularly short necks compared to older children, were included. Our results may not be generalizable to all pediatric patients.
Conclusion
Our first experience with Vscan Air™ for the assessment of internal jugular veins opens up new possibilities for ultrasound-guided central line placement and the evaluation of venous thrombosis in pediatric patients. Further studies need to be conducted, especially focusing on the peri-procedural use of handheld ultrasound.
Conflict of interest
The authors have no potential conflicts of interest to declare.