
Abstract
BACKGROUND:
Prophylactic mesh implantation following open surgical repair of abdominal aortic aneurysm is a debatable subject.
OBJECTIVE:
To assess the efficacy of a self-gripping polyester mesh used in on-lay technique to prevent incisional hernia after open abdominal aortic aneurysm repair.
METHODS:
We retrospectively reviewed the records of 495 patients who underwent aortic surgery between May 2017 and May 2021. Patients included in the study underwent open surgical repair for infrarenal abdominal aortic aneurysm (AAA) with closure of the abdominal wall with either small bite suture technique or prophylactic mesh reinforcement. Primary endpoint of the study was the occurrence of incisional hernia during a two-year follow-up period. Secondary endpoints were mesh-related complications.
RESULTS:
Mesh implantation with the on-lay technique was successful in all cases. No patient in the mesh group developed an incisional hernia during the 24-month follow-up period. Two patients in the non-mesh group developed a symptomatic incisional hernia during the follow-up period at 6 months. Three cases of post-operative access site complications were observed in the mesh group.
CONCLUSIONS:
Application of a self-gripping polyester mesh using the on-lay technique demonstrates acceptable early-durability after open surgical repair of abdominal aortic aneurysms. However, it appears to be associated with a number of post-operative access site complications.
Introduction
Incisional hernias after midline laparotomy have a variable prevalence of 3% to 20% [1, 2]. Approximately half of the incisional hernias occur in the first year after surgery [3]. Patients undergoing open surgical AAA repair appear to be at increased risk for incisional hernia development, possibly due to a number of systemic disorders affecting collagen and elastin synthesis and degradation [4]. The incidence of incisional hernia formation after open surgical AAA repair can be as high as 40% at follow-up [3, 6].
Abdominal wall hernias have a negative impact on patients‘ quality of life. Furthermore, they can also lead to complications such as bowel obstruction and strangulation. Several abdominal wall closure techniques have been reported to reduce the risk of this adverse event, such as various fascia suturing techniques, transverse rather than midline incisions and prophylactic abdominal wall reinforcement with mesh [7, 8]. The latter is the most widely used method, using either synthetic or biological material to close the fascia [9, 10]. The mesh can be applied using either an on-lay, in-lay or sub-lay technique, with current data being inconclusive regarding the optimal location [11–13].
The use of prophylactic mesh reinforcement during abdominal closure following open surgical AAA repair has been widely reported in the last years and has demonstrated numerous benefits to patients, including a reduced risk of incisional hernias and improved quality of life [2, 9]. However, it is also associated with risks and potential complications, such as mesh infection, seroma formation, mesh migration and mesh-related pain [6, 11]. This can lead to longer hospital stays and additional complications.
The available data on material selection for mesh reinforcement after open AAA repair are limited and mostly concern the use of synthetic polypropylene meshes. In this context, the aim of this study is to evaluate the efficacy of a self-gripping polyester mesh in abdominal wall closure after open AAA repair using the on-lay technique and to compare it with suture closure.
Materials and methods
Patient population
We retrospectively reviewed the records of all patients who underwent aortic surgery between May 2017 and May 2021. Patients included in the study underwent open surgical repair for infrarenal AAA with primary closure of the abdominal wall using either small bite suture technique or prophylactic mesh reinforcement with a two-year follow-up.
Parameters analysed included patient medical history, demographics and perioperative data. Perioperative outcomes and follow up data were collected and analyzed. The primary endpoint of the study was the occurrence of an incisional hernia at two years. Secondary endpoints were major and minor access site complications during the postoperative period. Major events were defined as complications requiring surgical management, whereas minor events were managed conservatively. The ethics committee of our institution approved the study (Registration number 21-2458-104).
Procedure
All operations were performed by two surgeons experienced in open aortic surgery (KP, KO). Surgical access to the abdominal cavity was obtained via a long midline incision from the subxiphoid to the suprapubic region. Aneurysmal repair was performed using a Dacron prosthesis (Maquet Cardiovascular, Wayne, NJ, USA). After closure of the aneurysmal sac and the posterior peritoneum, patients underwent fascial and abdominal closure using a continuous suture technique with a wound length ratio of 4 : 1. In patients with mesh reinforcement, additional preparation was performed on the left and right after fascial closure, to create a space between the anterior rectus sheath and the subcutaneous tissue. A self-gripping polyester mesh (ProGrip TM, Medtronic, Dublin, Ireland) was then applied on the fascia using the on-lay technique to reinforce the abdominal wall (Fig. 1). The mesh was fixed on the fascia surface with two stitches on the cranial and caudal end of the mesh using a long-term absorbable suture No 2/0 (MonoPlus, B. Braun Surgical, S.A., Rubi, Barcelona, Spain). Application of the mesh required approximately 15–20 minutes. A suction drain was placed in the subcutaneous tissue in all patients.
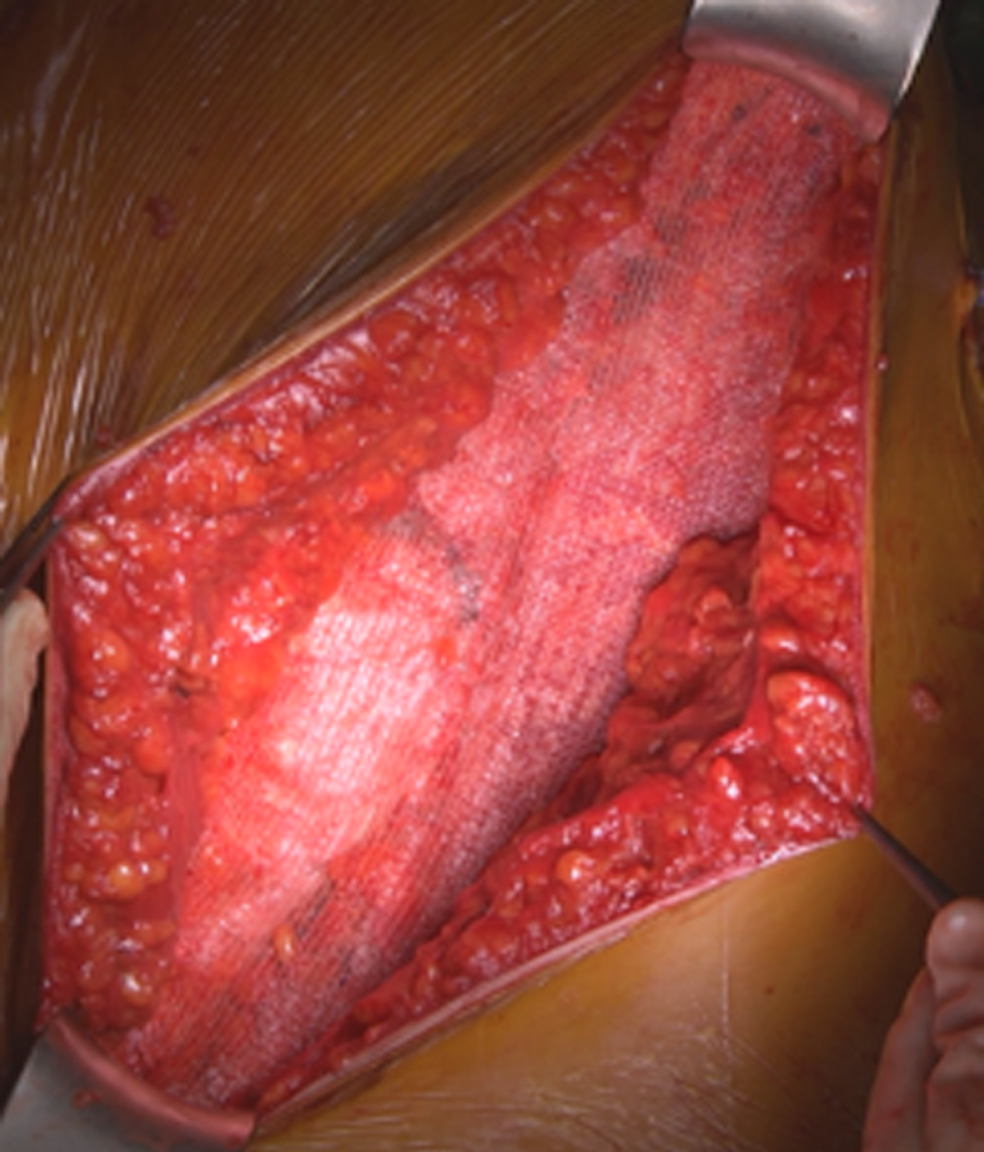
Application of the ProGriptrademark polyester mesh in on-lay technique during abdominal closure following abdominal aortic aneurysm repair.
Prior to discharge all patients underwent either ultrasound, computed tomography angiography (CTA) or magnetic resonance imaging (MRI) examination for control of the aneurysm and detection of possible incisional hernias. Patients were followed up either on an outpatient basis or by their general practitioner after 24 months.
Data analysis
Analysis of collected data was performed using SPSS for windows (Version 27; SPSS INC, Chicago, IL, USA). Variables were presented as mean±standard deviation (SD) in the case of normal distribution and as median plus range in the case of skewed data. Differences in age, sex and BMI used for aneurysmal repair between mesh and control groups were tested for statistical significance using the Mann-Whitney U test (two-tailed) for continuous variables and Fisher’s exact test (two-tailed) for categorical variables. Statistically analyzed data were considered significant when p < .05.
Results
A total of 495 patients who undergoing aortic surgery at our center were identified during the study period (Fig. 2). Endovascular aortic repair was performed in 448 cases. In 15 patients late open conversion was performed after explantation of an infected endoprosthesis. 7 patients underwent open surgical repair of thoracoabdominal aortic aneurysm (TAAA) and 5 patients of aortoiliac occlusive disease (AIOD) respectively. A total of 10 patients (9 male, 1 female, mean age 66.7±8.7 years) underwent open surgical repair of infrarenal AAA with prophylactic mesh reinforcement during abdominal closure. 10 patients (8 male, 2 females, mean age 71.4±9.1 years) were identified during the study period who underwent suture abdominal closure after open surgical AAA. Two patients in the mesh group had a previous history of median laparotomy. No patient was suffering from connective tissue disorders such as Ehlers-Danlos or Marfan syndrome. Patient demographics and comorbidities for both groups are summarised in Table 1.
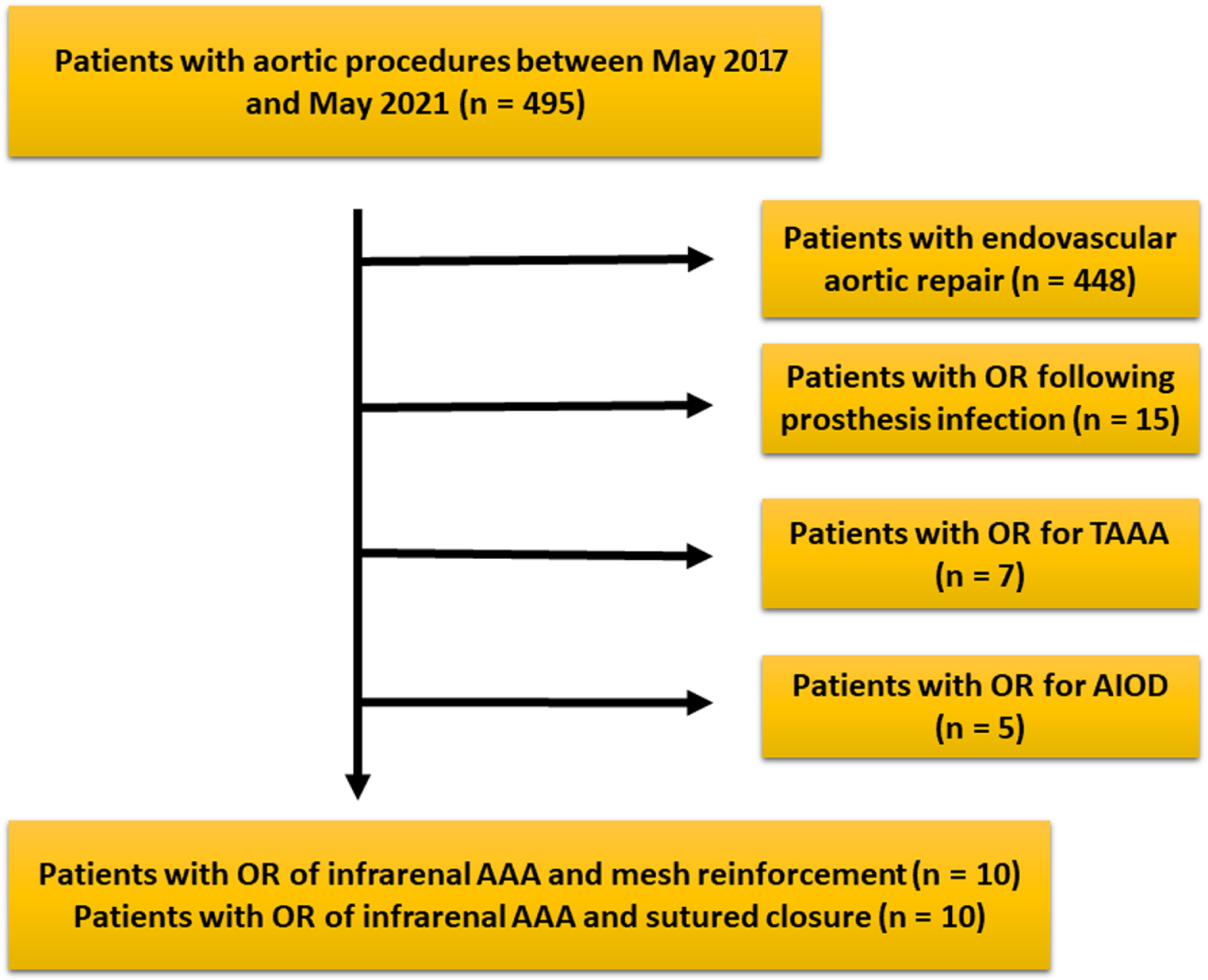
Figure showing patient selection and exclusion process. n = number, OR = open repair, TAAA = thoracoabdominal aortic aneurysm, AIOD = aortoiliac occlusive disease, AAA = abdominal aortic aneurysm.
Patients’ demographics. SD = standard deviation; BMI = body-mass-index; CAD = coronary artery disease; Hypertension = blood pressure > 130/80 mmHg; COPD = chronic obstructive pulmonary disease; Diabetes = HbA1 C >7%; Hypercholesterolemia = total cholesterol levels > 200 mg/dL; CKD = chronic kidney disease
Intensive care unit (ICU) and hospital length of stay were 3.9±1.4 and 14.5±6.8 days for the mesh group and 4.2±2.4 and 16±5.5 days for the non-mesh group respectively, with no statistical difference between the two (p = .91 for ICU and p = .35 for hospital length of stay). Three access site complications were observed postoperatively in the mesh group. One patient developed a subcutaneous seroma which was managed conservatively. One patient underwent local wound management due to a periumbilical dehiscence of the median laparotomy. The last patient had a prolonged hospital stay (30 days) due to wound infection requiring surgical revision. None of the patients required mesh explantation. There were no access site complications in the control group. Other post-operative complications included paralytic ileus (n = 2), renal failure (n = 1) and pulmonary embolization (n = 1) in the mesh group. In the control group, post-operative complications included renal failure (n = 3), cardiac insufficiency (n = 1) and paralytic ileus (n = 1).
Follow up was completed in all patients. One patient in the mesh group died of stroke at month 8. No patient in the mesh group developed an incisional hernia during the 24-month follow-up period. In the non-mesh group, two patients developed an incisional hernia during the follow-up period (p = .13). Both presented with bowel protrusion at month 6. In one case the hernia was managed surgically with mesh reinforcement. Operative revision for the second patient was delayed due to the COVID-19 pandemic. There were no further access site related complications in either group during follow-up. Post-operative and follow-up data are summarised in Table 2.
Postoperative complications and follow up data
The incidence of incisional hernia following open AAA repair ranges from 10 –47%, with up to 55% of incisional hernias occurring in the first 12 months after abdominal surgery [3, 6]. A number of reasons for this increased incidence have been identified, including obesity, chronic pulmonary obstructive disease (COPD) and connective tissue disorders [4, 14].
Mesh reinforcement to prevent incisional hernia has been widely reported in abdominal surgery. Mesh is placed using either an on-lay, a sub-lay or an in-lay technique. Most reports show significantly better results, with little or no difference in recurrence and infection rates between the different materials used [15–17]. In cases of abdominal closure following open AAA repair, current guidelines support the use of mesh reinforcement for abdominal closure [18, 19].
Various synthetic materials such as polypropylene, polyester, or expanded polytetrafluoroethylene can be used to close the abdominal defect [20]. There are limited reports on the use of biological materials, demonstrating certain advantages such as reduced risk of infection, adhesion formation and postoperative pain [10, 21]. Composite materials can be used to maximise the advantages of two synthetic materials, while minimising their disadvantages [20].
Polypropylene is a commonly used material during hernia repair, because of its low cost and good tissue integration. However, it is often associated with adhesion formation due to its inflammatory response, resulting in contraction of the mesh and the surrounding tissue [20]. There have also been reports of chronic wound pain and increased seroma formation in the on-lay position [15]. Polypropylene-based meshes have been used extensively in abdominal surgery for the prevention and the repair of various types of hernia, with most reports showing superior results to suture closure [15, 16]. In cases of open AAA repair, the use of polypropylene-based meshes during abdominal wall closure has been reported, but with limited data.
A meta-analysis from Indrakusuma et al, including four randomised control trials (RCTs), showed that mesh reinforcement during abdominal closure after open AAA repair significantly reduced the risk of incisional hernia compared with standard suture closure (RR 0.27, 95% CI 0.11–0.66) [22]. In three RCTs a polypropylene mesh was used for reinforcement of the abdominal wall. In one RCT a biological mesh from processed bovine pericardium was used for abdominal closure. There was no study using a polyester mesh, and it was unclear in the interpretation of the results whether the type of material used for abdominal wall reinforcement was important [22]. Another recent report by Honig et al investigated the incidence of incisional hernia after open AAA repair using a polypropylene mesh. The data showed no difference between mesh reinforcement and primary abdominal closure [23].
Polyester-based meshes show superior tissue incorporation and reduced adhesion formation compared to polypropylene when used in the onlay technique [24]. In some early reports polyester mesh was associated with higher infection and hernia recurrence rates. However, subsequent data has not supported these claims [24, 25]. In a report from 2019, Gillion et al evaluated the 2-year results following application of a composite polyester monofilament mesh with a collagen barrier for primary and recurrent hernias [26]. Their results were excellent, with limited complications, supporting the long-term efficacy of the composite polyester mesh [26]. In a meta-analysis by Totten et al, polyester mesh application after ventral hernia repair showed slightly better results in comparison to polypropylene in terms of infection rates (3.5%, 95% CI 2.5-4.9 vs 5%, 95% CI 3.9-6.3) [27].
In our study, abdominal closure was improved using a self-gripping polyester mesh with polylactic acid grips using the on-lay technique (ProGrip TM, Medtronic, Dublin, Ireland). The mesh is indicated for the prevention of incisional hernia [28]. It is made of a low-weight monofilament knitted fabric that incorporates absorbable polylactic acid micro hooks, providing enhanced tissue gripping. To the best of our knowledge, this is the first comparison of a polyester-based mesh being used for abdominal closure with small bite sutured closure following open AAA repair. During the 24-month follow up period, no cases of incisional hernia and no mesh related complications were reported. However, when compared to the non-mesh group who underwent sutured abdominal wall closure, there was a higher rate of access site related wound healing complications.
Limitations include the retrospective, single-centre, observational character of our study, the limited follow-up period and the small number of patients.
Conclusions
Application of the ProGriptrademark mesh during abdominal closure after open abdominal aortic aneurysm repair is simple using the on-lay technique and appears to be safe, with good early durability. However, it seems to be associated with a number of post-operative complications. Although an explantation of the mesh is rarely required, infection of the median laparotomy wound can pose a serious threat after open surgical AAA repair, leading to serious adverse events. As the number number of open AAA procedures has decreased over the last decade, multi-centre trials are needed to generate robust patient data and further evaluate the effectiveness of mesh reinforcement during abdominal closure after open aortic surgery. Cost effectiveness studies are also needed as mesh application is not reimbursed in some countries.
Informed consent
Written informed consent was obtained from all subjects involved in this study.
Funding
This study received no external funding.
Conflict of interest
Kyriakos Oikonomou has received educational grants from W.L. Gore & Associates, Bentley and is a consultant for Medtronic.
Author contributions
GS, JPD and TB wrote the manuscript, analyzed the data, reviewed the literature and supervised the manuscript preparation process. KO, WS, KP, CZ, and TB analyzed the data, reviewed, and edited the manuscript. KP and TB supervised the manuscript preparation process.