
Abstract
BACKGROUND:
No studies have been retrieved comparing perfluorobutane with sulfur hexafluoride for microwave ablation (MWA) in small hepatocellular carcinoma(sHCC).
OBJECTIVE:
To retrospective investigate the value of perfluorobutane ultrasonography contrast agent in ultrasonography (US)-guided MWA of sHCC.
METHODS:
We conducted a retrospective clinical controlled study about US-guided percutaneous MWA in patients with sHCC, and in patients undergoing intra-operative treatment with perfluorobutane or sulfur hexafluoride. In both groups, a contrast agent was injected to clear the tumor and then a needle was inserted. A 5-point needle prick difficulty score was developed to compare needle prick difficulty in the two groups of cases.
RESULTS:
A total of 67 patients were included: 25 patients in group perfluorobutane, aged 41–82 (60.64±9.46), tumor size 1.1–2.8 (1.78±0.45) cm. 42 patients in group sulfur hexafluoride, aged 38–78 (62.26±9.27), with tumor size of 1.1–3.0 (1.89±0.49) cm. There was no significant difference in age or tumor size in both groups (P > 0.05). Puncture difficulty score (5-point): 2.0–2.7 (2.28±0.29) in group perfluorobutane, and 2.0–4.7 (2.95±0.85) in group sulfur hexafluoride, and the difference between the two groups was statistically significant (P < 0.05). Enhanced imaging results within 3 months after surgery: complete ablation rate was 100% (25/25) in the group perfluorobutane, 95.2% (40/42 in the group sulfur hexafluoride), with no significant difference between the two groups (P > 0.05).
CONCLUSION:
Perfluorobutane kupffer phase can make the operator accurately deploy the ablation needle and reduce the difficulty of operation.
Keywords
Introduction
Microwave ablation (MWA) treatment is considered as a potential first-line treatment for many liver cancer patients, which has the advantages of minimally invasive safety and multiple repetition, especially for Small Hepatocellular Carcinoma (sHCC, ⩽3 cm) comparable to surgical resection [1, 2]. Ultrasonography (US) has many advantages such as real-time monitoring and flexible operation, and is often used for image guidance during MWA [3]. However, many sHCC is often not clear enough on US, especially the deep nodules, or near the diaphragm, which brings many difficulties to the accurate deployment of MWA needle.
Contrast-Enhanced Ultrasonography (CEUS) is a technique that uses the microbubbles of contrast agent to enhance the subsequent scattering echo, reflect and observe the blood perfusion of the diseased tissue, and then improve the resolution, sensitivity and specificity of US diagnosis [4]. At present, sulfur hexafluoride (SonoVue; Bracco) is the main Ultrasonography contrast agent used clinically in China. Hexafluoride is of great value in the detection of liver cancer and microvascular invasion [5, 6]. However, its development time is short and the stability of microbubbles is poor [7].
Perfluorobutane (Sonazoid; GE Healthcare) is a new contrast agent, which was approved in China in April, 2019. Previously, perfluorobutane had only been approved in Japan, Korea and Norway, and has not been approved in European and American. Using the characteristics of liver kupffer cells for specific uptake of perfluorobutane contrast medium, the specific kupffer phase 10 min after injection [8, 9]. Because most tumors contained no or only a few kupffer cells, most tumors do not show enhancement in the painful period. The imaging time of kupffer phase is more than 1 hour, so the operator has enough time to perform whole liver scanning, tumor localization and even other small lesions that can not be found by imaging [10, 11]. Perfluorobutane has been used in the differential diagnosis of benign and malignant liver masses and the evaluation of hepatocyte microvascular invasion [12, 13].
However, to date, no studies have been retrieved comparing sulfur hexafluoride with perfluorobutane for MWA in sHCC. Therefore, a retrospective clinical controlled study is warranted and we aim to determine the value of perfluorobutane in MWA of sHCC, and whether kupffer phase imaging is more advantageous than sulfur hexafluoride to improve the precision of MWA needle deployment to obtain efficacy and gather more evidence.
Methods
Trial design
This study was reviewed and approved by the Ethics Committee of our Hospital (No. 40, 2020). This retrospective clinical controlled study of MWA in patients with sHCC was conducted between January 2021 and December 2022. All patients were divided into perfluorobutane and sulfur hexafluoride groups based on different intra-operative use of contrast media. Written informed consent was obtained from all of the patients.
Inclusion criteria: (1) clinical diagnosis of Milan liver cancer or pathological diagnosis of preoperative biopsy; (2) single sHCC, with unclear gray-scale Ultrasonography development, the largest diameter is less than 3 cm; (3) before ablation, CEUS was performed with perfluorobutane or sulfur hexafluoride to improve tumor display. Exclusion criteria: (1) Patients who were not followed up; (2) severe cardiac and pulmonary insufficiency; (3) the coagulation function is seriously impaired.
Instrument and contrast medium
KY-2000 (Kangyou Medical or ECO Microwave System, China), aseptic KY-2450 B-1, single-point ablation power of 60 w, ablation time of 6 minutes. The ultrasonic instrument uses EsaoteMyLab twice (Parkson, Italy), and used CA 541 (1–5 MHz) convex array probe. Contrast agent: perfluorobutane is a white block preparation, and 2 ml sterile water for injection was extracted for reconstruction. When injected through the cubital vein, according to the patient’s weight of 0.015 mL/kg, 5 mL of normal saline was injected. Sulfur hexafluoride is a white powder preparation, which is arranged in 5 mL suspension with normal saline. It is injected by elbow vein lump, with 2 ml each dose, and then injected with 5 ml normal saline.
Procedure
In both groups of cases, general anesthesia was used, and perfluorobutane or sulfur hexafluoride was used to make the tumor clear, and then puncture needle. Single needle ablation was used to inactivate the tumor and the surrounding 1 cm liver parenchyma to achieve the safety boundary. The evaluation effect was performed by CEUS, and the who did not reach the safety boundary should be supplemented.
Puncture difficulty score (5 points): the difficulty score table of needle insertion process (5 points). The scoring standard: two radiologists with more than 10 years’ working experience clearly image the tumor, and then calculate the average score. If the development is very clear, it will be 1 points, 2 points for good, and 3 points for general; In the process of needle puncture and needle deployment, one point will be given for injection of contrast medium once, and two points will be given for injection ≥2 times. The two items were summed up as the final score. Post-contrast tumor development definition score (1–3 points) and contrast agent injection frequency score (1–2 points).
Follow-up
Postoperative follow-up: Enhanced imaging (MRI, CT or US) was performed within 3 months after operation to evaluate the short-term efficacy: there was no abnormal enhancement within the edge of ablation focus until the ablation was completed; Abnormal interior or edge of incomplete ablation.
Statistical analysis
Statistical analysis was performed by SPSS 19.0 software, normally distributed measurement data were expressed (mean±standard deviation), and t test was used for comparison between groups. Count data were expressed as number of cases and percentage, and comparison between groups were performed using χ 2 test. A P < 0.05 was considered as a statistically significant difference.
Results
Demographics and baseline characteristics
A total of 81 patients met the inclusion criteria, as well as 14 patients who did not follow-up regularly or were lost to follow-up following surgery. Finally, 67 patients were included, including 41 naive patients and 26 relapsed patients (12 had a history of surgical resection and 14 with ablation). Among them, 25 participants were treated with perfluorobutane, and 42 participants were treated with sulfur hexafluoride (Fig. 1). There were 54 males and 13 females, aged 38–82 (61.66±9.30), and tumor size 1.1–3.0 (1.85±0.47) cm. Perfluorobutane group 25 patients, aged 41–82 (60.64±9.46), tumor size 1.1–2.8 (1.78±0.45) cm; 42 patients in sulfur hexafluoride group, aged 38–78 (62.26±9.27), tumor size 1.1–3.0 (1.89±0.49) cm. There were no significant differences in age or tumor size in the two groups (P > 0.05, Table 1).
Flow chart of the study selection process.
General data, Puncture difficulty score (5-point) and efficacy comparisons between the perfluorobutane and sulfur hexafluoride groups
In 25 patients in the perfluorobutane group, the needle was administered in the kupffer phase, with a contrast injection of 1. Of the 42 patients in the sulfur hexafluoride group, 36 were performed in the arterial phase and another 6 in the portal and delayed phase, with a minimum of one and a maximum of four. Score of needle difficulty: 2.0–2.7 (2.28±0.29) in group perfluorobutane, and 2.0–4.7 (2.95±0.85) in group sulfur hexafluoride, and the difference between the two groups was statistically significant (P < 0.05), Fig. 2 and Table 1.
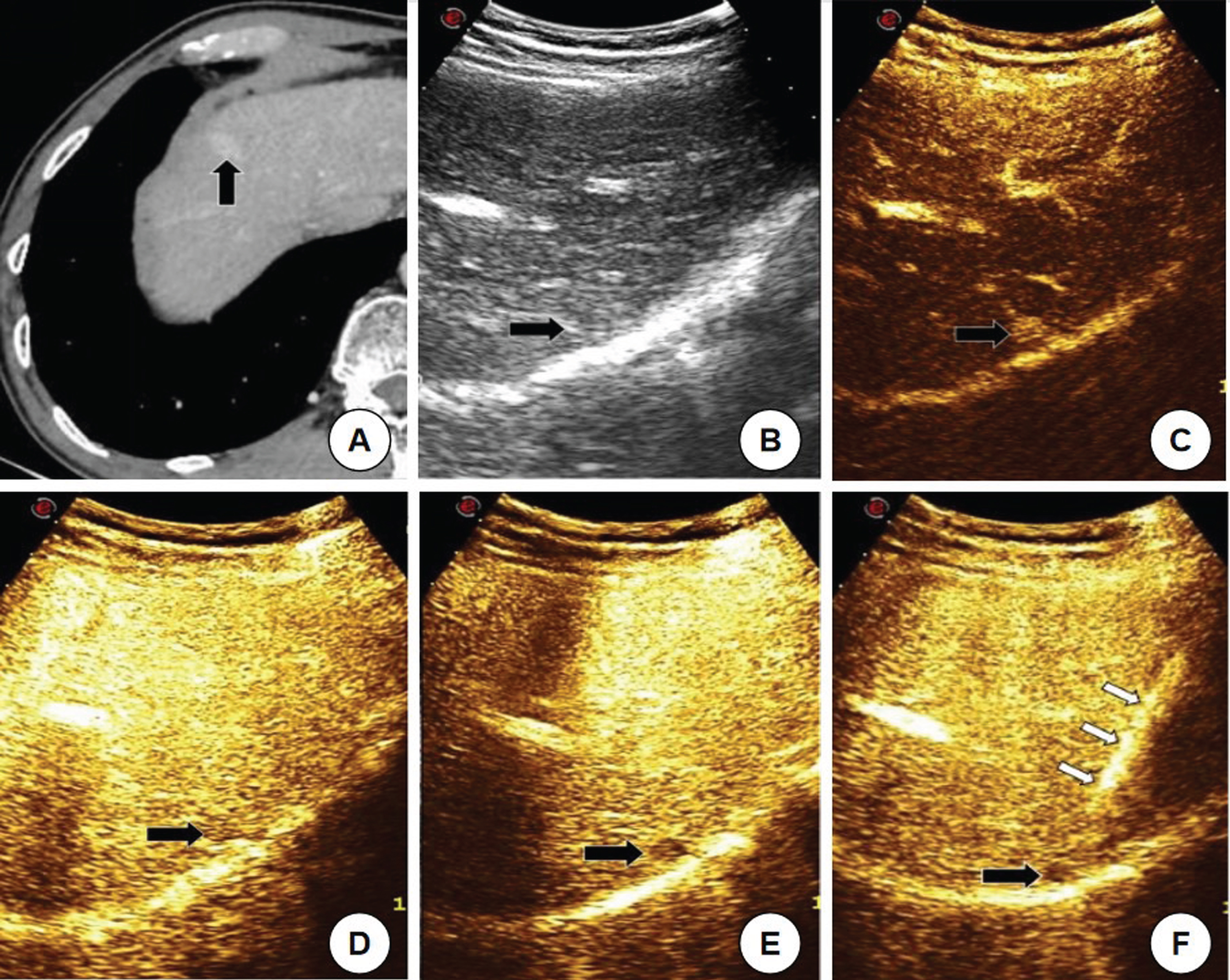
The Small hepatocellular carcinoma patients underwent microwave ablation under perfluorobutane guidance in kupffer phase. A 65-year-old male, 2 years after liver cancer surgery, has cancer of the right liver. (A) Enhanced CT found new carcinoma of the right liver (black arrow), size 1.1×0.8 cm; (B) Gray scale ultrasonography is difficult to distinguish from the surrounding liver parenchyma due to the small tumor, isoecho, and deep location; (C) In perfluorobutane contrast, the arterial stage tumor showed high enhancement and obvious contrast with the surrounding liver parenchyma, but the duration was only 6 s; (D) The tumor in the delayed stage showed a slightly lower enhancement, without obvious contrast with the surrounding liver parenchyma; (E) The tumor showed a very low enhancement in kupffer phase, and high enhancement of the peripheral liver parenchyma, in sharp contrast and long duration; (F) Deploy the ablation needle in kupffer phase (white arrow is microwave ablation needle injection).
Enhanced imaging was performed within 3 months after ablation, complete ablation rate was 100% (25/25) in perfluorobutane group and 95.2% (40/42) in sulfur hexafluoride group, and there was no significant difference between the two groups (P > 0.05).
Discussion
MWA can be used as a radical treatment for sHCC, and its precise deployment is the key to its efficacy [14]. In this study, it was shown that the unique kupffer phase of the perfluorobutane contrast agent, with its well-defined tumor development and long duration, gives the operator sufficient time and confidence to perform a continuous procedure, and that an accurate needle can achieve better ablation.
sHCC is easy to be missed on gray-scale US. In particular, 47.8% of liver cancers of 1 cm were not detected on gray scale US [15, 16]. First, 90% of people with primary liver cancer have viral hepatitis and cirrhosis. People with cirrhosis often have multiple regenerative nodules in the liver. If there are sHCC mixed together, it is sometimes difficult to distinguish [17–19]. Second, liver cancer is located deep in or near the diaphragm, and tumor development may be unclear and missed due to sound attenuation and other reasons. The tumor development may be unclear and be missed. In particular, it is particularly difficult to detect. In addition, sHCC located under the capsule and close to the ribs are likely to be missed [20]. At the same time, some tumors are not easily detected when US scans are affected by gas in the lungs or intestines [21, 22].
US is the most commonly used guideline for thermal ablation of liver cancer in clinical practice. This may result in incomplete ablation when the development of liver cancer is unknown. In order to achieve better ablation effect, CEUS is usually used to improve the contrast between tumor and surrounding liver parenchyma, and puncture ablation is performed after the tumor development is clear [7, 23]. Currently, there are mainly two common ultrasonography contrast agents in China, perfluorobutane and sulfur hexafluoride. Sulfur hexafluoride has long been used in clinical practice. Most previous studies of CEUS in thermal ablation of liver cancer have been based on this approach. Both perfluorobutane and sulfur hexafluoride angiography include arterial phase, portal phase and delayed phase, while perfluorobutane has more kupffer phase on this basis [24]. This is the unique contrast phase of the perfluorobutane. A large number of kupffer cells in the liver parenchyma phagocytose perfluorobutane microspheres, and the normal liver parenchyma showed high enhancement, while the lack of kupffer cells, usually showed low or no enhancement, in sharp contrast to the surrounding normal liver parenchyma, and the imaging can last for 1 hour [25].
The puncture needle under sulfur hexafluoride contrasts sharply with the surrounding liver papillae, but only for a few seconds to more than ten seconds. The development time is short, and it is difficult to meet the requirements for accurate puncturing needles, sometimes requiring repeated injections [26]. There are 2 cases in this study, with a maximum number of up to 4 injections. However, the contrast between portal and delayed stage tumors and peripheral hepatic papillae is often not significant enough, and the utilization values are limited. Only 6 of the 42 patients in the sulfur hexafluoride group in this study had a puncture during this time. All 25 needles in perfluorobutane group were performed in phase kupffer. Previous studies have shown that the kupffer hepatocellular carcinoma and hepatic parenchyma are more significant in the arterial phase compared to the arterial phase of perfluorobutane, which is more favorable for puncture guidance. Moreover, the development time of kupffer liver stage is very long, which enables that the operator has enough time for meticulous operation to achieve the purpose of accurate puncture needle [27–29].
In addition, because the two contrast agent microbubble shell composition is different, sulfur hexafluoride microbubbles are more likely to rupture, US imaging requires lower mechanical index (<0.1), and perfluorobutane can be imaging under higher mechanical index (>0.2), higher mechanical index ablation needle can show more clearly, this is conducive to puncture needle, more important is able to improve the safety of puncture [30, 31]. The kupffer period of perfluorobutane is easier to operate and more convenient. All patients in the perfluorobutane group of this study received only one contrast injection before ablation, and the two groups were statistically different (P < 0.05).
Enhanced imaging examination within 3 months after ablation showed that the recent efficacy of the two groups was similar, with no statistical difference (P > 0.05). The evaluation of curative effect after ablation is of paramount importance [32]. Tumor recurrence and scar changes after ablation can be judged by CEUS. The typical change of scar after MWA is lack of contrast enhancement from artery to late stage. In marginal recurrence, irregular nodular angiographic enhancement of the arteries in the marginal area and irrigation of these nodular tumors at the beginning of the portal venous phase usually occur [33, 34]. Previous literature shows that CEUS and enhanced CT have the same value. Of course, enhancing MRI is still the most accurate method at present [35].
Some limitations of this study remain. First, the scoring system is based on the supervisor’s judgment and is related to the operator’s experience. Second, the small sample size of this study, which may be biased, calls for more data accumulation and more in-depth studies.
Conclusion
In summary, the tumor development is clear and prolonged during the kuffer phase of perfluorobutane, giving the operator enough time and confidence to perform continuous manipulation and accurate puncturing of the needle to achieve better ablation.
Author contributions
QQA, YHP and DLL contributed to the data curation, analysis, investigation and writing of the manuscript. FL, ZXK and DLL performed and analysed the ultrasonography examinations and operation of the patients. QQA and XZ also reviewed, edited the writing and validated the whole analysis process. All authors read and approved the final manuscript.
Conflict of interest
All the authors declare that there is no conflict of interest.
Funding
This work was supported by funding from the Zhejiang Province Medical and Health Science and Technology Program Project (2022KY1019 and 2021KY937), and Hangzhou Science and Technology Plan Guidance Project (20201231Y033).