
Abstract
OBJECTIVE:
This study aims to evaluate the diagnostic efficacy of a novel system called contrasted enhanced ultrasound thyroid imaging reporting and data system (CEUS TI-RADS) for benign and malignant thyroid nodules. We also seek to assess inter-observer agreement.
METHODS:
The study recruited 433 patients who underwent thyroid ultrasound (US) and CEUS between January 2019 and June 2023 at Affiliated Hospital of Guangdong Medical University. A retrospective analysis of 467 thyroid nodules confirmed by fine-needle aspiration (FNA) and/or surgery was performed. Further, a CEUS TI-RADS classification was assigned to each thyroid nodule based on the CEUS TI-RADS scoring criteria for US and CEUS features of the nodule. The nodules were grouped based on their sizes, i.e., size≤1 cm for Group A, 1 cm < size≤4 cm for Group B, and size > 4 cm for Group C. Multivariate logistic regression was used to analyze independent risk factors for malignant thyroid nodules. Pathological assessment was the reference standard for establishing sensitivity (SEN), specificity (SPE), accuracy (ACC), positive predictive value (PPV), and negative predictive value (NPV) of CEUS TI-RADS for diagnosing malignant thyroid nodules. Receiver operating characteristic curve (ROC) analysis was performed to compare the diagnostic efficacy of the scoring system in predicting malignancy in three groups of nodules. The intragroup correlation coefficient (ICC) was adopted to assess the inter-observer agreement of the CEUS TI-RADS score.
RESULTS:
Out of the 467 thyroid nodules, 262 were malignant and 205 were benign. Logistic regression analysis revealed that the independent risk factors for malignant thyroid nodules included punctate echogenic foci (P < 0.001), taller than wide (P = 0.015), extrathyroidal invasion (P = 0.020), irregular margins/lobulated (P = 0.036), hypoechoic (P = 0.038) on US and hypo-enhancement (P < 0.001) on CEUS. The ROC for CEUS TI-RADS diagnosis of malignant thyroid nodules was 0.898 (95% CI:0.867–0.924, P < 0.05) for all nodules, 0.795 (95% CI: 0.721–0.857, P < 0.05) for group A, 0.949 (95% CI: 0.916–0.971, P < 0.05) for group B, and 0.801 (95% CI: 0.644–0.910, P < 0.05) for group C with optimal cut-off values of CEUS TI-RADS 5 points (all nodules), CEUS TI-RADS 6 points (group A), CEUS TI-RADS 5 points (group B), CEUS TI- RADS 5 points (group C), respectively. Among these groups of nodules, group B had the highest ROC, with SEN, SPE, ACC, PPV, and NPV for diagnosing malignant nodules being 95.9%, 88.1%, 92.8%, 92.6%, and 93.2%, respectively. The ICC of the CEUS TI-RADS classification between highly senior and lowly senior physicians was 0.862 (P < 0.001).
CONCLUSION:
In summary, CEUS TI-RADS demonstrated significant efficacy in distinguishing thyroid nodules. Nonetheless, there were variations in its capacity to detect malignant nodules across diverse sizes, demonstrating optimal performance in 1 cm to 4 cm nodules and providing important insights for clinical diagnoses.
Introduction
Thyroid nodules are distinct lesions inside the thyroid gland that differ radiologically from surrounding thyroid parenchyma. Their etiology ranges from common inflammatory responses and hyperplasia to transformative neoplastic shifts. In recent decades, nodule detection has significantly increased, driven by the development and widespread of high-resolution ultrasound (US) technology. Thyroid nodules are prevalent, targeting an estimated 60% of adults [1]. Although only approximately 5% of nodules have been confirmed to be malignant [2], the possibility of cancer is a major concern and timely screening of thyroid nodules is increasingly important to clinicians and patients. Accurate detection of benign and malignant thyroid nodules is a critical element of preoperative US, which can effectively reduce the risk of puncture.
Several US risk stratification systems for thyroid nodules, including thyroid imaging reporting and data system (TI-RADS) have been introduced by many international organizations, among them, Chile, Korea, the European Thyroid Association, the American College of Radiology (ACR), and Chinese Medical Association (CMA) [3–7]. Nonetheless, these systems are based on a two-dimensional US assessment of thyroid nodules, which lack information on blood flow microcirculation making it difficult to precisely assess the nodules. Unlike the conventional US, the contrasted enhanced ultrasound (CEUS) can provide real-time insights into the vascular perfusion and hemodynamics of thyroid nodules, allowing dynamic assessment of microvascularization patterns [8], which is considered a valuable novel approach for identifying benign and malignant nodules [9, 10]. Jung et al. [11] integrated several ultrasound techniques to assess thyroid nodules and determined that multimodal ultrasound is effective in early detection of malignant nodules. They proposed that CEUS and elastography are suitable for targeted follow-up of TI-RADS III nodules. However, in the case of small nodules (≤1 cm), quantitative analysis with CEUS can offer additional and more objective reference values for the differential diagnosis of these smaller nodules [12]. In addition, CEUS has less clinical utility in predicting cervical lymph node metastasis of thyroid malignant nodules. Concerning cervical lymph node metastases, Liu et al. [13] observed that a larger thyroid tumor diameter, proximity to the peritoneum, and increased neovascularization are associated with an elevated risk of cervical lymph node metastasis. These factors collectively create pathways for the invasion and metastasis of cervical lymph nodes. Meanwhile, numerous researchers have reported that the CEUS features of metastatic lymph nodes in the neck often present centripetal enhancement, asynchronous enhancement, high enhancement, inhomogeneous enhancement, and ring enhancement. Quantitative CEUS parameter analyses, especially the area under the curve (AUC), descend time to one-half (DT/2) parameters, may be more sensitive and accurate in predicting metastatic lymph node invasion and metastasis [14]. Through univariate and multivariate logistic regression analyses, Ruan et al. [15] discovered that nodule composition, echogenicity, shape, margins, echogenic foci, and extra-thyroidal extension in US, as well as the direction of enhancement, peak intensity, and circumferential enhancement on CEUS were important predictors of thyroid carcinoma in 2022. Nevertheless, previous studies found that the size of thyroid nodules influences vascular development and visualization, as well as biological behavior and prognosis of thyroid nodules [16–18], resulting in different clinical decisions. Herein, we investigated the diagnostic value of CEUS TI-RADS in nodules of different sizes by taking the maximum diameter of nodules as 1 cm and 4 cm as the boundary for more valuable reference information for clinical decision-making.
This study sought to confirm the diagnostic efficacy of CEUS TI-RADS in thyroid nodules and further assess the diagnostic performance of CEUS TI-RADS for thyroid nodules of various sizes. Moreover, the use of CEUS TI-RADS between sonographers of different seniority was necessary to be assessed by the inter-observer concordance of CEUS TI-RADS scores.
Materials and methods
Ethics statement
This retrospective study was approved by the institutional review board of the Affiliated Hospital of Guangdong Medical University (PJKT2024-028). Each patient signed the informed consent papers containing a CEUS, fine-needle aspiration (FNA), and surgery for these tests or procedures.
Study population
The inclusion criteria included: (a) patients who underwent US and CEUS at Affiliated Hospital of Guangdong Medical University; (b) patients with a final postoperative pathological result or FNA result of Bethesda II, Bethesda V and Bethesda VI based on The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) [19]; (c) patients with no history of previous treatment, including thyroid surgery, chemotherapy, radiotherapy or I131 treatment. The exclusion criteria included: (a) patients whose nodules are classified as Bethesda I, III, or IV according to TBSRTC; (b) patients without final pathologic results. A total of 446 patients fulfilled the inclusion criteria between January 2019 and June 2023 (Fig. 1).
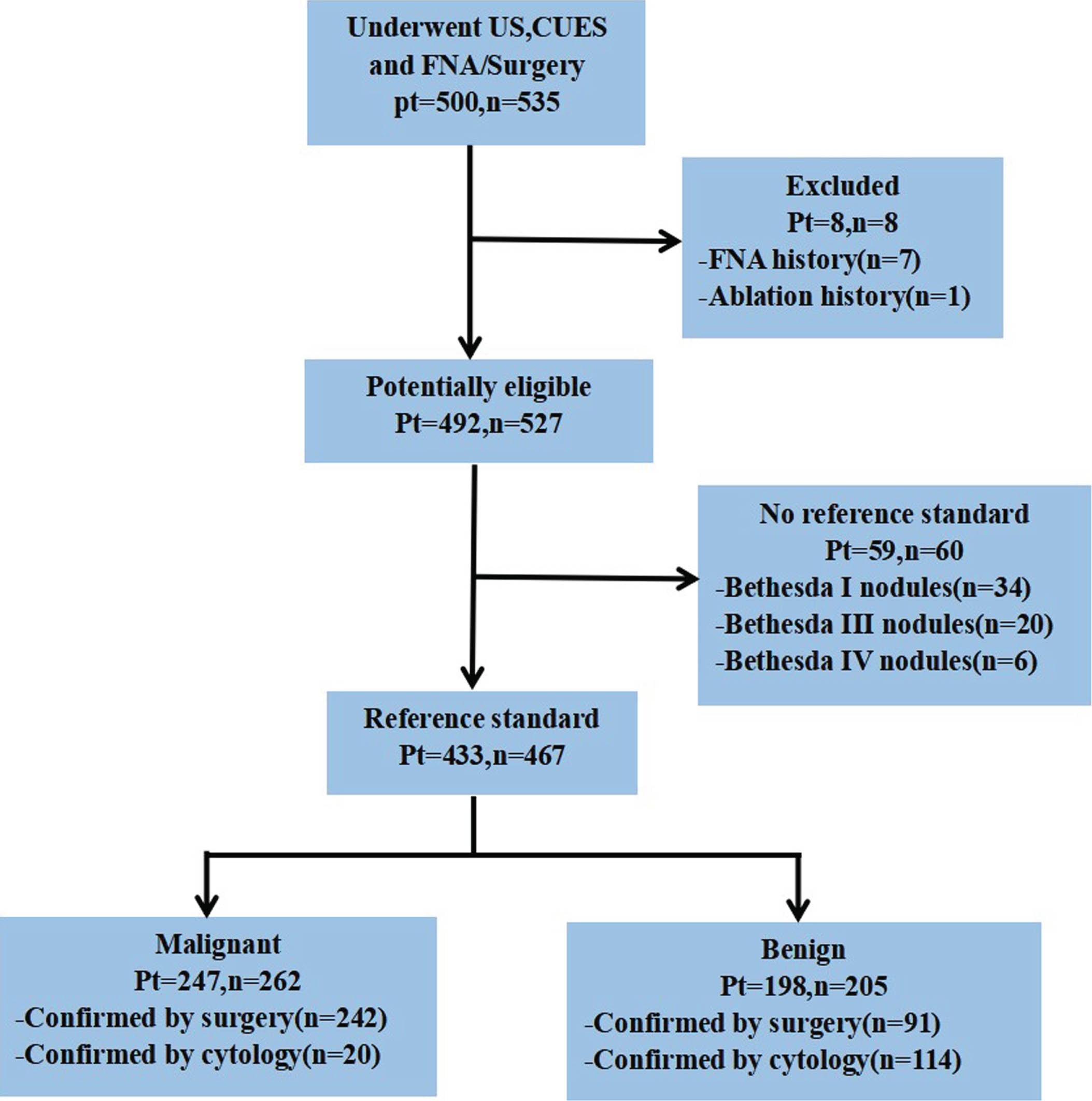
Study flowchart. US: ultrasound, CEUS: Contrast-enhanced US, FNA: Fine-needle Aspiration, n: Number of Thyroid Nodules, pt: Number of Patients. Note. Out of 433 patients 400 patients had a single nodule, 32 patients had two thyroid nodules, out of which 12 patients had one benign nodule and one malignant nodule respectively, and one patient had three nodules.
A high-frequency linear probe (Siemens Acuson Sequoia and Canon Aplio 500) was used for every US inspection. SonoVue TM (Bracco Imaging S.p.A., Milan, Italy), a sulfur-hexafluoride-filled microbubble contrast agent protected by a flexible phospholipid shell was the contrast medium. To create intravenous access, a 20-G needle was placed into the patient median cubital vein. The patient was instructed not to swallow after the contrast agent and 5 ml of saline were combined and agitated to homogeneity. Subsequently, 2.4 ml of the suspension was rapidly injected into the median cubital vein whereas the probe and body posture were kept constant. After injection, the timer on the ultrasound machine was set to start. The photographs were stored on the hard disk of the ultrasound device, which was constantly monitoring the dynamic perfusion process of the lesion in real-time.
To calculate the inter-observer concordance of CEUS TI-RADS scores, 150 thyroid nodule images were randomly selected for individual analysis of US and CEUS features. These features included size, echogenicity, sh ape, margin, echogenic foci, and extra-thyroidal invasion in US, as well as enhancement direction, peak intensity, ring enhancement, and composition on CEUS. Two sonographers performed the analysis. The junior sonographer had experience of less than 5 years in thyroid ultrasonography, whereas the senior sonographer had more than 5 years of experience. Importantly, both sonographers were blinded to the pathologic findings; nodules were scored and categorized following the CEUS TI-RADS classification criteria. Subsequently, interobserver variability in CEUS TI-RADS scores was retrospectively evaluated. Figure 2 illustrates the CEUS TI-RADS categories criteria.

Chart of CEUS thyroid imaging reporting and data system (CEUS TI-RADS), with correspondent malignant probabilities and indications for FNA.
Statistical analyses were performed on the software SPSS 27.0 (IBM, Armonk, NY, USA) and MedCalc 22.0 (Applied Math, Mariakerke, Belgium). Normally distributed measurements were presented as mean±standard deviation. Comparisons of categorical variables were performed using the X2 test, and logistic regression was employed to identify independent risk factors predictive of malignant nodules for both US and CEUS characteristics. Receiver operating characteristic (ROC) analysis was used to establish the cut-off values, compute the area under the curve (AUC), and establish 95% confidence intervals (CI). The sensitivity (SEN), specificity (SPE), accuracy (ACC), positive predictive value (PPV), and negative predictive value (NPV) were measured to assess the diagnostic efficiency of the CEUS TI-RADS system. The significance level was set at p < 0.05. Inter-observer agreement for CEUS TI-RADS scores was evaluated through the intragroup correlation coefficient (ICC). The agreement was classified as poor (ICC≤0.50), moderate (0.50 < ICC≤0.75), good (0.75 < ICC≤0.90), and very good (ICC > 0.90).
Results
Study population, US, and CEUS features of thyroid nodules
In total, 500 patients with 535 nodules underwent US, CEUS, and FNA/surgery between January 2019 and June 2023. A total of 8 nodules were excluded because of FNA history (n = 7) or ablation (n = 1). Moreover, 60 nodules, including 34 Bethesda I nodules, 20 Bethesda III nodules, and 6 Bethesda IV nodules were excluded for the lack of reference standard. Finally, 467 nodules from 433 patients were included, among which 33 patients had two nodules and one patient had three nodules. The mean age of all malignant nodules was (45±13) years and the mean age of benign nodules was (48±13) years. Out of the 467 nodules, 262 were malignant and 205 were benign. A total of 242 malignant nodules were diagnosed with the pathologic result, including 234 papillary thyroid carcinomas (PTC), 6 follicular thyroid carcinomas (FTC), and 2 medullary thyroid carcinomas (MTC). A total of 91 benign nodules were surgically confirmed, including 62 nodular goiters, 12 follicular thyroid adenomas (FTA), 7 Hashimoto thyroiditis, 3 granulomatous thyroiditis, 3 Hürthle cell tumors, 1 ectopic thymus, and 3 noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP). The cytologic assessment confirmed 20 malignant and 114 benign nodules, among which 3 were Bethesda V, 17 were Bethesda VI, and 114 were Bethesda II. Table 1 shows US and CEUS characteristics of all nodules.
Clinical features of the study population and basic characters of thyroid nodules
Clinical features of the study population and basic characters of thyroid nodules
As shown by logistic regression analysis, punctate echogenic foci (P < 0.001), taller than wide (P = 0.015), extrathyroidal invasion (P = 0.020), irregular margins/lobulated (P = 0.036), hypoechoic (P = 0.038) on US and hypo-enhancement (P < 0.001) on CEUS were the independent risk factors for malignant thyroid nodules (Table 2). The nodules were grouped based on their sizes, i.e., nodule size≤1 cm was group A, 1 cm < size≤4 cm was group B, and size > 4 cm was group C. The diagnostic efficacy of the CEUS TI-RADS classification in differentiating benign and malignant thyroid nodules was examined using ROC analysis (Fig. 3). The AUC of CEUS TI-RADS for all nodules was 0.898 (95% CI:0.867–0.928, P < 0.05), whereas nodules of group B obtained excellent performance with AUC, SPN, SPE, ACC, PPV and NPV of 0.949 (95% CI: 0.916–0.971, P < 0.05), 95.9%, 88.1%, 92.8%, 92.6% and 93.2%, respectively. Table 3 presents AUC, SPN, SPE, ACC, PPV, and NPV for Group A and Group C.
Factors associated with malignancy in thyroid nodules
Factors associated with malignancy in thyroid nodules

ROC analyses for the diagnostic performance of the CEUS TI-RADS for predicting the malignancy of thyroid nodules in different groups.
Comparison of the diagnostic performances of CEUS TI-RADS in different size nodules
In group A, echogenicity, shape, and calcification on the US, as well as the direction of enhancement (Figs. 4, 5), peak intensity (Fig. 6), and composition (Fig. 7) on CEUS were statistically different between benign and malignant nodules (P < 0.05). On the other hand, margin (P = 0.050) (Fig. 7), extra-thyroidal invasion (P = 0.306) in the US, and ring enhancement (P = 0.878) on CEUS were not statistically different between benign and malignant nodules. In group C, margin, calcification, and extra-thyroidal invasion on US, as well as peak intensity, ring enhancement, and composition on CEUS were statistically different between benign and malignant nodules (P < 0.05), whereas echogenicity (P = 0.171), shape (P = 1.000) on US, enhancement direction (P = 0.845) and composition (P = 1.000) on CEUS were not statistically different. In group B, all US and CEUS characteristics were statistically different (P < 0.05) (Table 4).
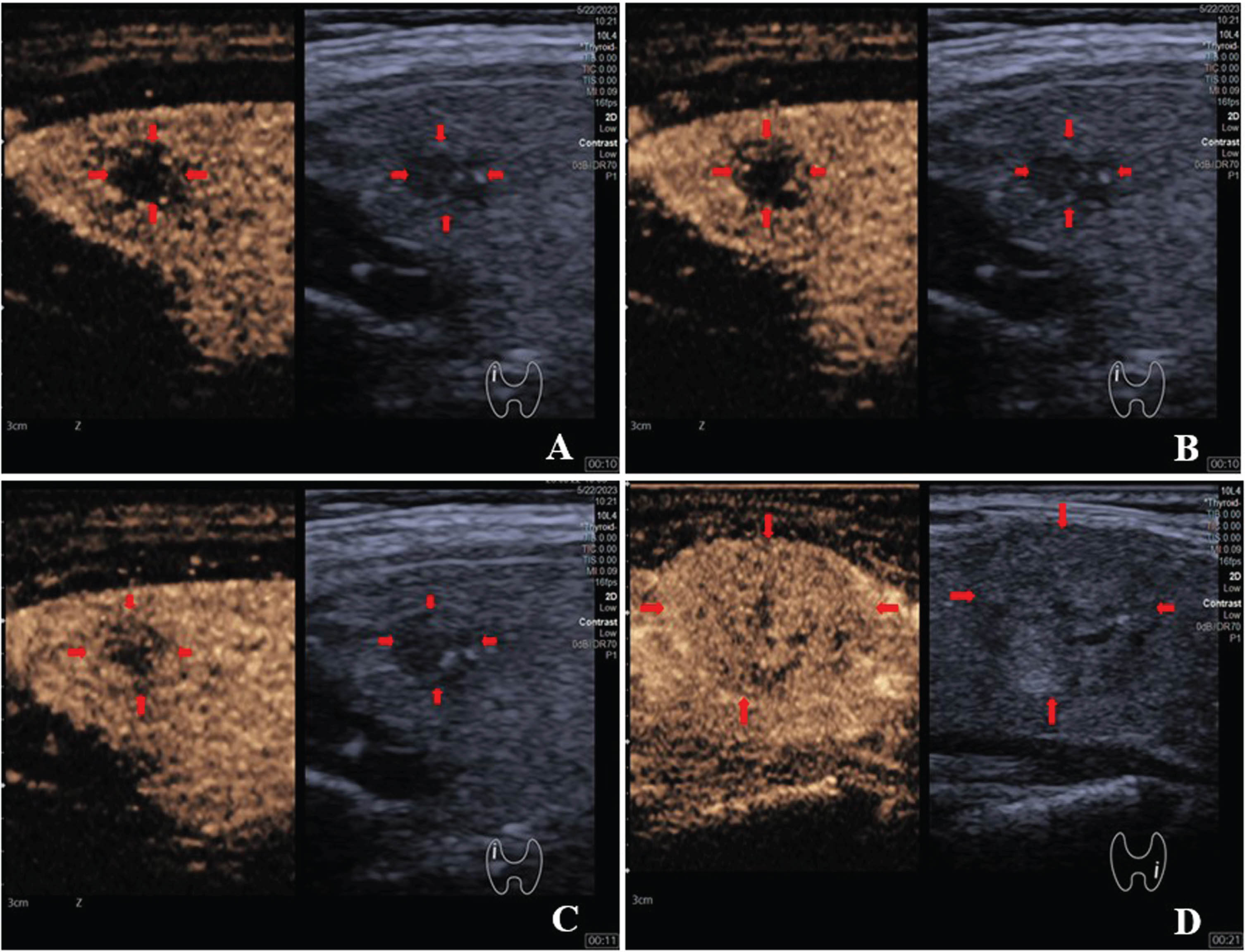
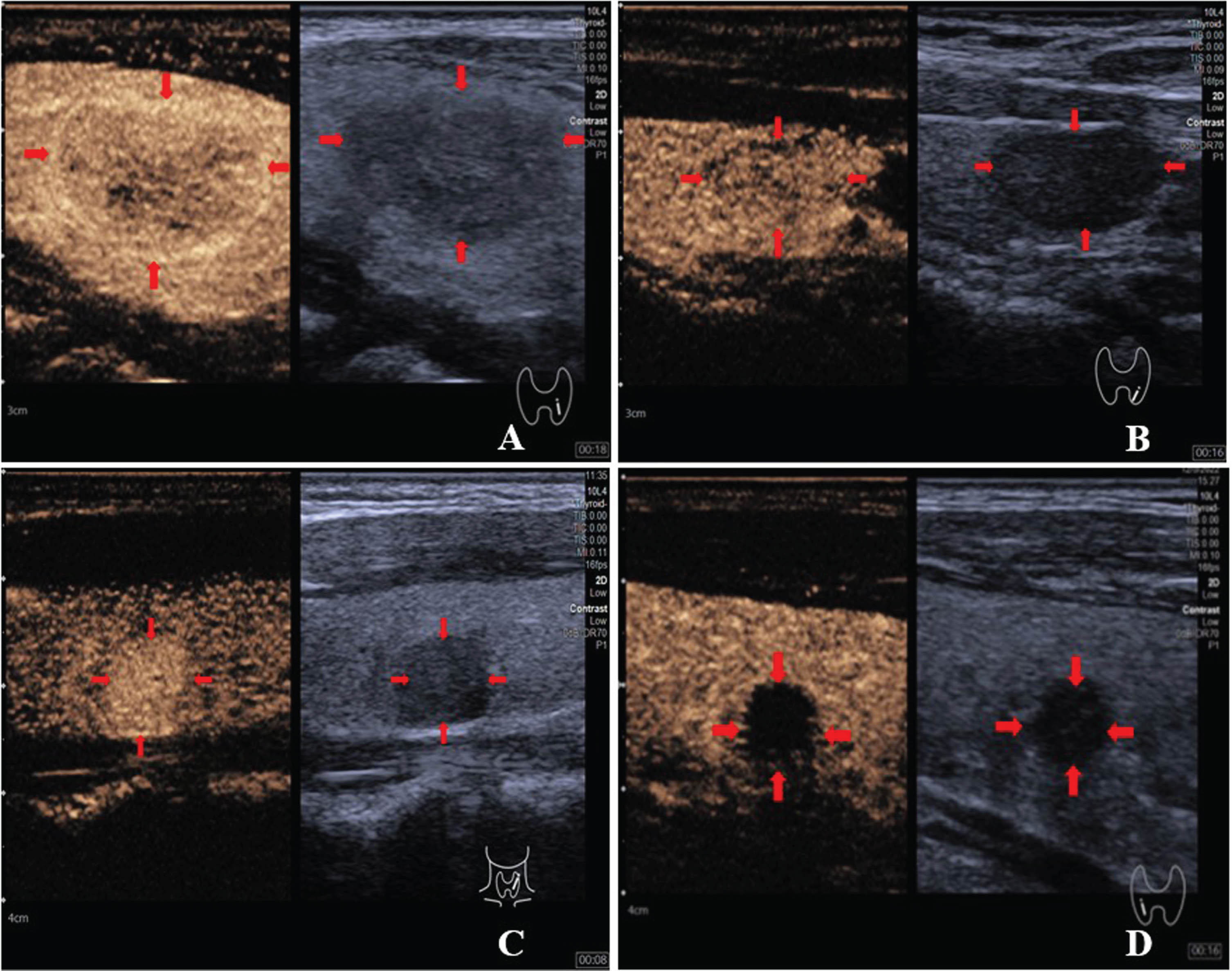
Images (A-C) showed centripetal enhancement of the same papillary thyroid carcinoma (PTC) nodule (red arrows) in the right lobe of thyroid gland of a 69-year-old woman; the image (D) was a case of a benign nodule (red arrows) in the left lobe of thyroid gland of a 41-year-old woman showing feature of scattered enhancement on CEUS. The minutes and seconds after the contrast media injection were indicated by numbers in the bottom right corner of each panel.
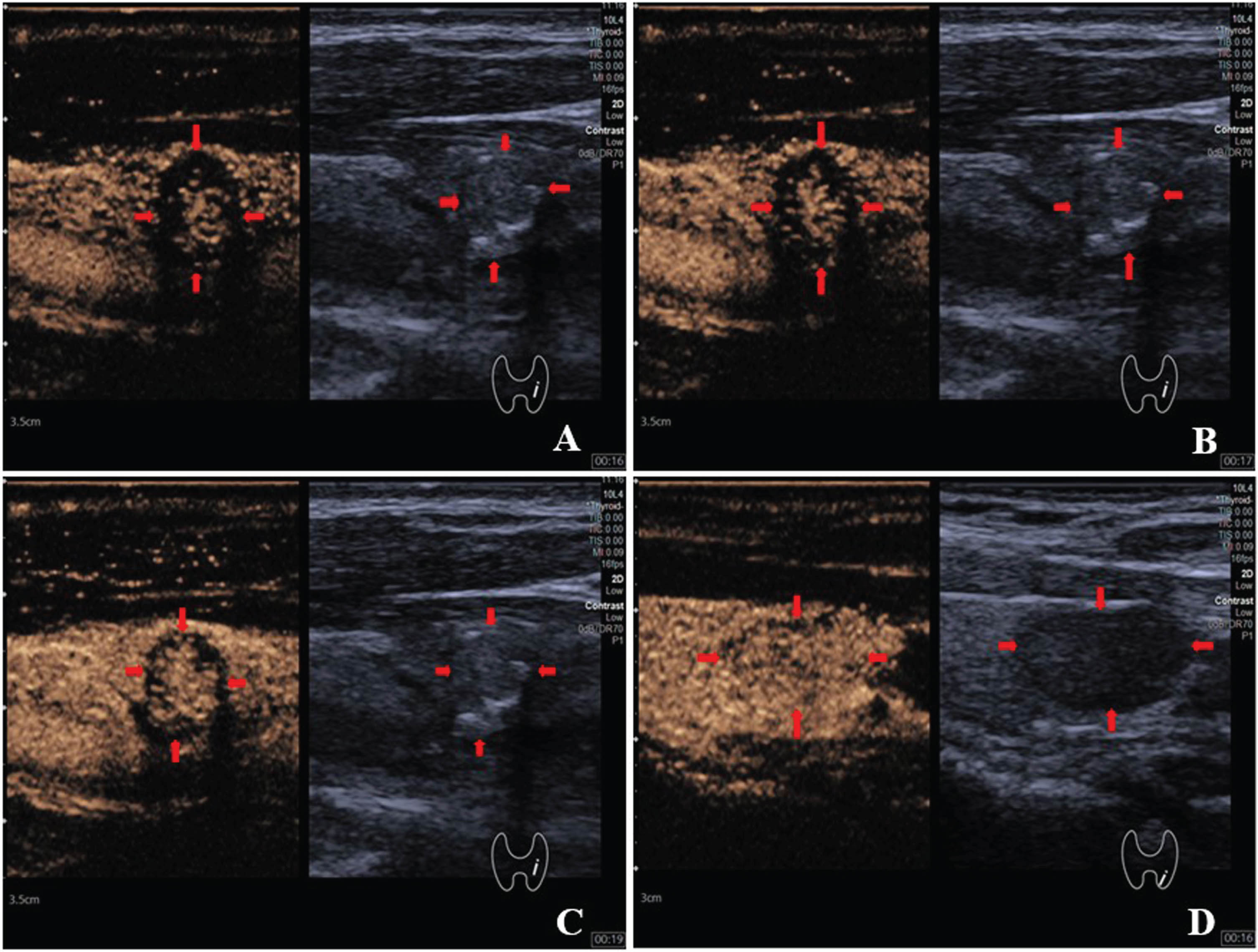
Images (A-C) showed centrifugal enhancement of the same papillary thyroid carcinoma (PTC) nodule (red arrows) in the left lobe of thyroid gland of a 69-year-old man; image (D) was a case of a benign nodule (red arrows) in the left lobe of thyroid gland of a 65-year-old woman showing feature of scattered enhancement on CEUS. The minutes and seconds after the contrast media injection were indicated by numbers in the bottom right corner of each panel.
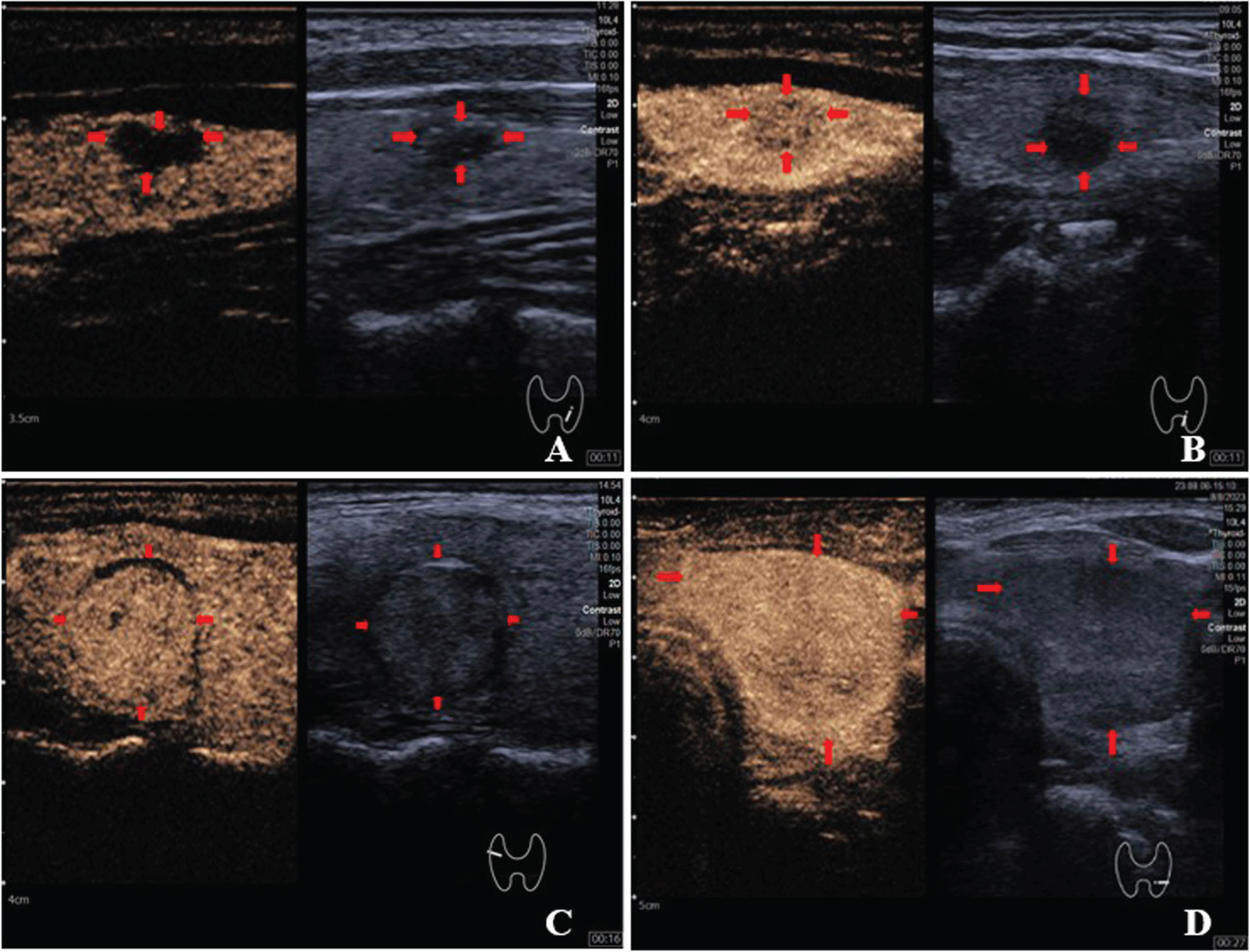
Images (A-D) shouwed feature of peak enhancement of thyroid nodules (red arrows). (A) nonenhancement; (B) hypoenhancement; (C) isoenhancement; (D) hyperenhancement. The minutes and seconds after the contrast media injection were indicated by numbers in the bottom right corner of each panel.
Images (A-D) showed features of ring enhancement and composition of thyroid nodules (red arrows). (A) ring enhancement; (B) absent ring enhancement; (C) solid; (D) nonsolid. The minutes and seconds since the contrast media injection are indicated by numbers in the bottom right corner of each panel.
US and CEUS features of benign and malignant nodules of different sizes
The ICC was used to analyze the concordance between the scores of senior and junior sonographers for 150 thyroid nodules. Consequently, the ICC between senior and junior sonographers for the CEUS TI-RADS score was 0.862 (P < 0.001).
Discussion
At this stage, ultrasound has become the preferred screening method for thyroid diseases due to its advantages of non-invasiveness, low cost, no radiation, simplicity and reproducibility. In recent years, ultrasound technology in this field has made great progress, such as CEUS and ultrasound elastography, etc. These new technologies play an important and irreplaceable role in the differential diagnosis of thyroid nodules.
Zhang et al. [20] combined traditional US, shear wave elastography and BRAF V600E to evaluate nodules with benign FNA results, and then compared them with the final pathological results, and found that the combined three methods diagnostic efficacy was higher than alone, and the difference was statistically significant (P < 0.05), suggesting that further clinical decision-making should be considered for any nodule with two or more signs of suspected US malignancy and a hard ultrasound elasticity display. Whereas Ruan et al. [15] pioneered the development of CEUS TI-RADS by combining conventional US with CEUS, and they used the CEUS TI-RADS in the differential diagnosis of benign and malignant thyroid nodules with good results in internal cross-validation and external validation. Their ROCs were 0.93 (95% CI: 0.92–0.95) for internal validation, 0.89 (95% CI: 0.84–0.92) for the first external validation set, and 0.90 (95% CI: 0.85–0.94) for the second external validation set. However, none of these validation sets were investigated in groups based on nodule size. This study categorized the nodules into groups based on size to further investigate the diagnostic efficacy of CEUS TI-RADS. The World Health Organization (WHO) defines papillary thyroid microcarcinoma (PTMC) as a PTC with a maximum diameter of 1 cm [21]. Although several major guidelines, including the ACR, recommend surveillance of sub-centimeter nodules, many patients with suspicious sub-centimeter nodules are subjected to FNA in our country due to patient anxiety, physician preference, family history, and other factors [22]. When the maximum diameter of the nodule exceeds 4 cm, the risk of capsular and vascular invasion, which converts follicular adenoma into follicular carcinoma increases and more likely compresses the trachea, causing aesthetic problems [1]. Therefore, the nodules were classified based on their sizes, with size≤1 cm being Group A, 1 cm < size≤4 cm being Group B, and size > 4 cm being Group C.
Our results revealed that the highest AUC of 0.949 (95% CI: 0.916–0.971, P < 0.05) was obtained for nodules in group B, whereas the AUCs for nodules in groups A and group C were 0.795(95% CI: 0.721–0.857, P < 0.05) and 0.801 (95% CI: 0.644–0.910, P < 0.05), respectively. This was consistent with the findings of Li et al. [23], who used CEUS to diagnose nodules smaller than 1 cm and found no significant benefit of CEUS in TMC diagnosis. The poor diagnostic efficacy of CEUS TI-RADS for sub-centimeter nodules might be attributed to (1) FNA experiencing problems with insufficient specimens and false negative results, with most studies showing false-negative rates of less than 5%, and others reporting higher rates (ranging from 7.5% to 21%) [24]; (2) The volume effect could arise in CEUS because of small nodule, in which benign nodules including the mummified nodules are readily misdiagnosed as malignant nodules. Therefore, we suggested that for sub-centimeter nodules, the contrast agent dose be appropriately reduced based on machine conditions and the sonographer’s experience to significantly minimize the volume effect. Nevertheless, when the nodule was too large for the limited probe exploration range, it was difficult to precisely diagnose the nodule, whereas CEUS could provide effective guidance for puncture to improve the positive puncture rate of the nodule [25].
For small nodules (group A), malignant nodules were mostly PTC whereas benign nodules were largely nodular goiter. Both benign and malignant nodules were largely hypoechoic, with little evident extra-thyroidal invasion and most did not have ring enhancement features on CEUS. However, not all benign nodules in large nodules (group C) were predominantly iso/hypoechoic, and there were quite a few with hypoechoic features. Due to the large size, most of the nodules were wider than tall on conventional US, and nearly all appeared solid on CEUS. Due to the high number of vasculatures, branches, and arteriovenous fistulae inside the larger nodules, the inside of the nodule would be simultaneously perfused with the blood-rich thyroid tissue. Therefore, it yields unsatisfactory results in the differential diagnosis of benign and malignant large and small nodules using US and CEUS.
We found that CEUS TI-RADS had a significant benefit in the differential diagnosis of thyroid mummification and PTC. Mummified thyroid nodules (MTNs) [26] are cystic solid nodules that change after treatment such as resorption or nodal ablation, and the nodules show signs of malignancy including hypoechoic/very hypoechoic and taller than wide in atrophic collapse, which can be classified as TI-RADS 5 in the ACR TI-RADS classification. Furthermore, we discovered that CEUS could improve the classification between PTC and MTNs, as the former exhibited centripetal anisotropic hypoenhancement due to its relatively poor vascularization. MTNs, on the other hand, mostly exhibited the absence of enhancement on CEUS, which might help reduce the unnecessary FNA and surgical resections of such nodules. This is consistent with the findings of Chen et al. [27].
Although CEUS could play a crucial role in differentiating MTNs from PTC, this scoring system failed to categorize FTC and inflammatory nodules. In this investigation, there were 6 cases of FTC, among which only 2 cases were classified as category 5 and 4 as categories 3-4A; circumferential hyperenhancement was observed in the 6 FTC. Therefore, distinguishing FTC from adenoma or nodular goiter with adenomatous hyperplasia was difficult because the US manifestations of FTC did not show apparent malignant signs including extrathyroidal invasion and microcalcifications. Since tumor invasion of the margin or blood vessels was the only pathological diagnostic criterion for FTC [28], CEUS TI-RADS could not differentiate between FTC and FTA with any degree of precision. Therefore, there is a need for additional studies on CEUS sensitivity and specificity for FTC diagnosis.
Meanwhile, 5 nodules with Hashimoto’s thyroiditis pathology and 2 nodules with granulomatous thyroiditis pathology were misdiagnosed as malignant. The misdiagnoses were attributed to the concomitant microcalcification of the nodules, aspect ratio > 1, and low enhancement of the malignant signs. Hashimoto’s thyroiditis with fibrosclerotic nodules and granulomatous thyroiditis is characterized by fibrosis as the primary pathological change and poor blood supply, making them prone to overlap on US and CEUS, hence complicating their differentiation from malignant nodules [29]. Zhang et al. [29] revealed that CEUS combined with time-intensity curve (TIC) parameters could provide effective quantitative information on microvascular perfusion for differential diagnosis of inflammatory thyroid nodules and PTC, which warrants further validation.
Unlike the findings of Ruan [15], our study performed logistic regression analysis on the ultrasound characteristics of 467 nodules. As a result, we found that hyperenhancement and the presence or absence of circumferential enhancement were not statistically significant in differentiating between benign and malignant nodules, corroborating with the findings of many previous studies [9, 30]. We believe that the inconsistent conclusions might still be attributed to the tumor size and growth stage. Tumor growth is categorized into two stages, i.e., from the slow growth stage without blood vessels (pre-vascular stage) to the rapid growth stage with blood vessels (vascular stage). In relatively small tumors with no or few blood vessels, the enhancement observed by CEUS was majorly hypoenhancement. Upon rapid tumor growth, various neovascularizations are formed under various angiogenic factors, causing nodule hyperenhancement shown by CEUS [31]. Notably, the presence of a halo is often considered a benign feature [32]. However, some thin halos shown on conventional US might be unclear and difficult to detect, whereas the surrounding rings could be observed on CEUS. More peripheral halo rings could be observed on CEUS than on conventional US. Because its formation factors remain unclear, scholars [33, 34] analyzed the ring enhancement of the nodule; they suggested that irregular ring hyperenhancement is a sign of malignancy, and the non-enhancement ring could focus on the regularity and irregularity, and should combine with the enhancement features inside the nodules. Therefore, we thought that categorizing ring enhancement before allocating points would be more rigorous.
In the present study, a senior and a junior medical practitioner independently assessed 150 thyroid nodules, using the CEUS TI-RADS classification system for scoring purposes. The ICC was 0.86, indicating a high degree of consistency in their assessments. This outcome confirmed the use of this approach as a valuable diagnostic tool for junior medical practitioners.
This work has several compelling limitations. First, it is a single-center retrospective study, and the reading scores of the physicians are based on static charts, which do not mimic real clinical practice; thus, the findings might not be generalizable to other institutions. Secondly, some of our pathology outcomes were based on FNA, which potentially caused FNA false positives and false negatives. Thirdly, most of the malignant nodules were PTC; therefore, the diagnostic value of this scoring system for other malignant pathologic types needs further research.
Conclusion
In conclusion, the novel CEUS TI-RADS scoring system has high efficacy in the differential diagnosis of benign and malignant thyroid nodules, potentially reducing FNA or unnecessary surgical intervention for benign nodules, particularly MTNs. Nonetheless, its diagnostic efficacy is influenced by the nodule size, implying that more prospective multicenter studies are required to further validate and provide valuable information for clinical diagnosis.