
Abstract
BACKGROUND AND OBJECTIVE:
Ultrasound-guided interventions (such as biopsies) of unclear lesions are indicated if microcirculatory changes indicate possible malignant lesions. These place high demands on the ultrasound device used. In order to potentially reduce the often associated high technical effort, the wireless ultrasound device Vscan AirTM was examined as a possible ultrasound device for the intervention biopsy.
METHODS:
As part of an advanced training course on Computertomographie- and ultrasound-guided biopsy and ablation procedures, participants were asked about the image quality of the handheld device used by means of questionnaires. Various lesions were evaluated at a depth of 1.0 to 5.0 cm in an in vitro liver model. The image quality was evaluated independently before, during and after the intervention. The rating scale contained values from 0 (no assessment possible) to 5 (maximum high image quality). A high-end device was used as a reference.
RESULTS:
A total of 11 participants took part in the study (n = 4 male [36.4%], n = 7 female [63.6%]). A total of five tumor like lesions at different depths (1 cm, 2 cm, 3 cm, 4 cm, >4 cm) were assessed separately. In all cases, an adequate biopsy of the target lesion (1 cm in length, core filling 5 mm) was successful. From a depth of 3 cm, the image quality of the mobile device increasingly decreased, but the image quality of the high-end system was still not impaired. Compared to the high-end device, there was a highly significant difference in image quality from a depth of 3 cm (p < 0.01). Assessment by inexperienced examiners using a handheld device was adequately possible.
CONCLUSIONS:
Mobile interventional ultrasound represents a potential alternative for the biopsy of unclear tumorous lesions with microcirculatory disorders with limited depth localization.
Introduction
The use of ultrasound diagnostics has become increasingly important in almost all areas of medicine in recent years. In addition to the development of constantly more modern and powerful ultrasound devices and ultrasound techniques [1, 2], the use of ultrasound in interventional procedures such as biopsies is also becoming increasingly important [3, 4]. These are used in particular for superficial and intrahepatic lesions and have a decisive advantage over CT-guided biopsies due to the lack of radiation exposure.
In addition to these advantages, however, the practical implementation of such interventions is also associated with some limitations. In addition to the limited mobility of the high-end devices used in everyday clinical practice due to their size and the cable connections to the ultrasound probes, the hygienic cleaning of these devices after completion of the intervention requires a great deal of time and effort. This in turn reduces the number of possible interventions to be carried out per day.
With the technology of mobile handheld ultrasound devices such as Vscan AirTE and TE Air, there are new ways of counteracting these problems [5]. In addition to its already proven high level of user-friendliness, its wireless connection to a separate screen – which can be flexibly selected and freely positioned in the room according to the respective requirements – is an important aspect. Initial studies on the applicability of this still relatively new technology already exist and provide indications of its fundamentally adequate image quality [6, 7].
With regard to the evaluation of intervention models in vitro for microcirculation, however, the specifications are very complex. It would mean that tissue structures would have to be almost matched to an in vivo model using complex measures. This is partly carried out for tissue transplants [8]. In a common in vitro model, vascular structures are recognizable in the B-scan, but hemodynamics and microcirculation cannot be evaluated. However, in the course of repeated punctures/biopsies, a change in vascular structures in the puncture canal can be recognized on the basis of the subsequent evaluation using, among other things, macroscopy. Experience already exists with real-time in vivo models of microcirculation through to CEUS perfusion with the question of changes in the recurrent application of X-ray contrast media [9, 10]. However, the applicability of mobile handheld ultrasound devices in in vitro tumor models (e.g. for biopsies) is still largely unexplored.
In the present study, the feasibility of ultrasound-guided biopsies with the Vscan AirTM device was therefore analyzed for the first time using an in-vitro liver model.
Material and methods
Ethics vote
After consultation with the Ethics Committee of the University of Regensburg, there were no ethical concerns regarding this study.
The survey of course participants took place as part of a quality assurance program for an interactive radiological intervention course. It was carried out on a voluntary basis. The decision regarding participation had no influence on the course progression. The questionnaires were completed anonymously. Appropriately trained staff were available to answer questions.
Questionnaires
A panel of experts [physicians (specialist status or in training to become a specialist) and MTRs (medical technologists for radiology)] developed a questionnaire with a total of 8 questions to assess the image quality of in vitro examinations using Vscan AirTM based on the experience of the panel members and the existing literature. This was checked for comprehensibility, meaningfulness and feasibility by means of pre-testing and then – if necessary – modified accordingly before final use.
The final questionnaire was completed anonymously by the participants without any possibility of identifying the person completing it. Prior to this, instructions were given regarding the evaluation of the individual parameters. A separate room was made available for completing the questionnaire. The completed questionnaires were then collected in a non-transparent container provided for thispurpose.
Assessment scale
A rating system from 0 to 5 was used independently to evaluate the image quality of the examined lesions: 0 = no evaluation possible, 1 = no diagnostic evaluation possible, 2 = major limitations of diagnostic evaluation, 3 = proportionate limitations of diagnostic evaluation but sufficient for a reliable assessment, 4 = only mild limitations of diagnostic evaluation, 5 = excellent image quality without limitations. The lesions were assessed independently before, during and after the intervention. The assessment criterion here was the delimitability of the lesion or the biopsy needle from the surrounding tissue.
Documentation of the results was done in a proprietary Excel spreadsheet. The applicable data protection rules were complied at all times.
Ultrasound devices used
Handheld system
The Vscan AirTM device from GE was used in this study. It is a wireless ultrasound device that enables direct transmission of the image in real time to a corresponding end device. The corresponding compatible app was previously installed on it. The Vscan AirTM has a linear (3–12 MHz) and a convex probe (2–5 MHz) and the option of using CCDS (color coded Doppler sonography) [6].
High end device
The Resona 9 ultrasound device from Mindray was used. It is a high-end device which, in addition to the classic examination tools (B-Scan, CCDS), also features modern techniques such as elastography and CEUS (contrast enhanced ultrasound). The linear probe L 15-3WU (3–15 MHz, center frequency 10 MHz) was used.
Biopsy needle systems used
The following biopsy systems were used (Fig. 1): Company BIP, Device Koaxialkanüle HistoCore®, Article-Nr.: C14130 Company Pflugbeil, Device Coaxial SABD Biopsy Device, Article-Nr.: CS-1415-15-T
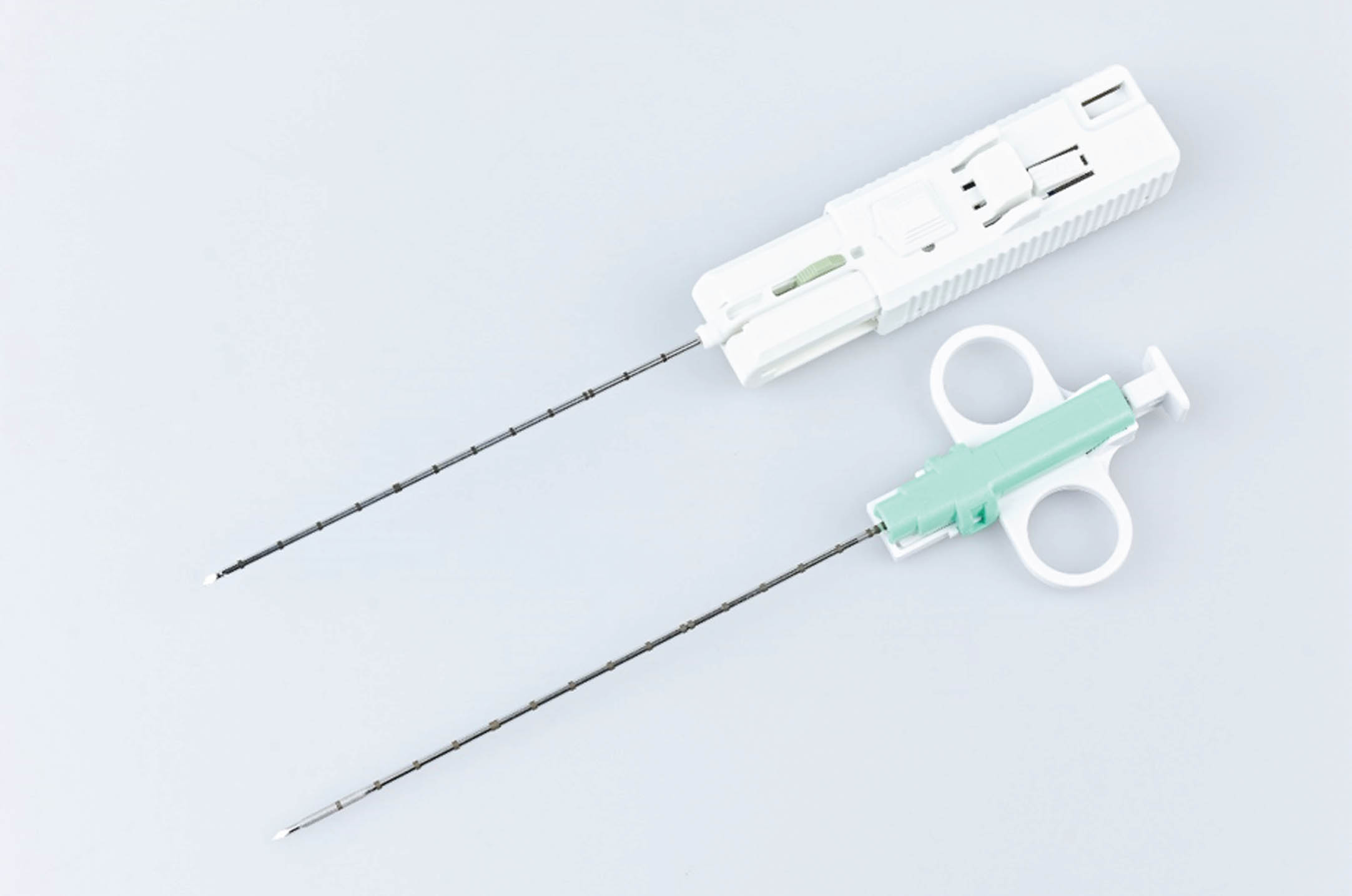
Illustration of the two biopsy needle systems used (image created by the authors).
The participants in the course were made up of physician and non-physician healthcare professionals. All participants were familiar with the basics of using ultrasound technology.
In vitro model used
An in vitro liver model was provided for the study. Beef livers were used, which were provided by a local meat cutting company (Family Kurth, Regensburg, Germany). After appropriate preparation (including the provision of protective materials such as gloves, covers or disinfection facilities), these were cut from the back at different depths and then filled with an olive stuffed with paprika (commercially available sizes up to 1 cm in length and a paprika filling up to 5 mm in diameter; corresponds to a simulation of a mass with border area and center), which represents the lesion to be displayed in the ultrasound (Figs. 2 and 3). The placement of the olives to be biopsied in the liver model – both superficially and in depth – was carried out independently of the biopsies performed and without the interventionalists knowing the exact localization. Finally, a complete biopsy was checked using the biopsy punches obtained and at the end of the test series by removing the biopsied olive parts from the biopsy bed.
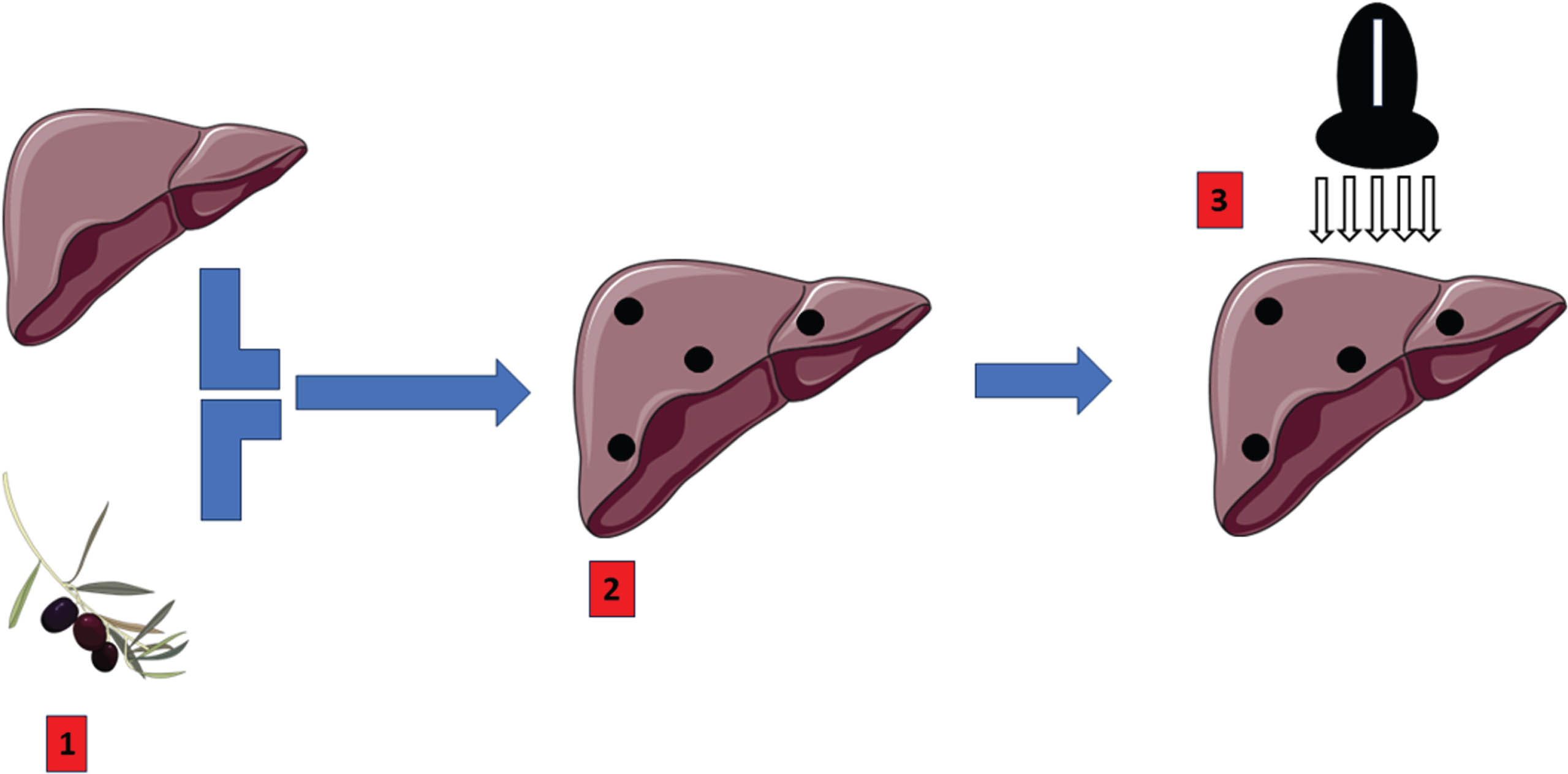
Schematic representation of the in vitro liver model used: 1) Preparation of the liver model by providing a liver and filled olives as intrahepatic lesions 2) “Spiking” the liver by incising and implementing the olives (black dots) at different depths in the liver model 3) Ultrasound and localization of the spiked liver and subsequent biopsy of the olives [11].
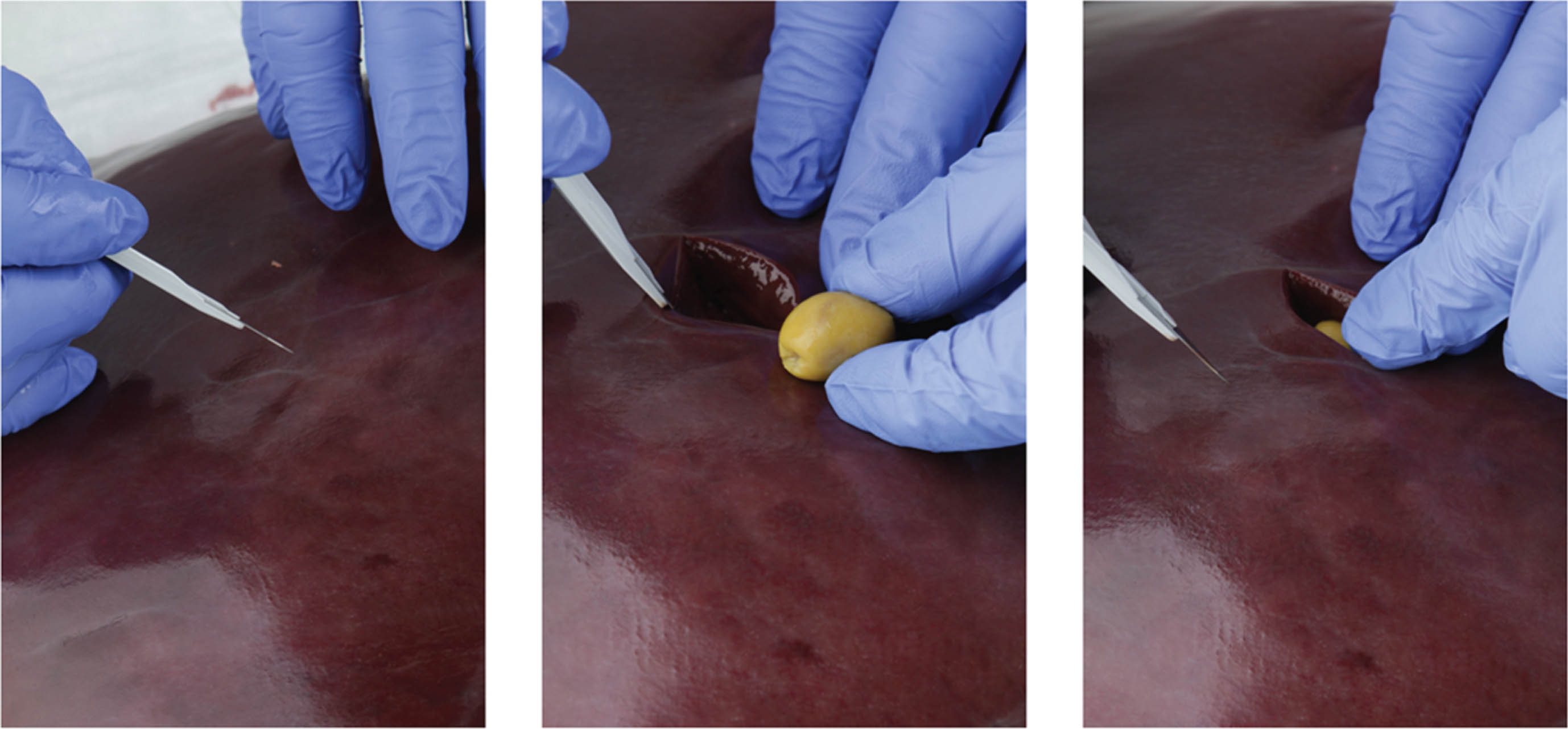
Illustration of the “spiking” of the liver model with the olives as target lesions (sequence from left to right) (image created by the authors).
The significance level for the hypothesis tests was set at p < 0.05. We presented categorical variables as number (percentage [%]) and continuous variables as mean (standard deviation [SD]) or median (interquartile range [Q1–Q3]). The normal distribution was examined using the Shapiro-Wilk test. Differences between the groups of experienced vs. non-experienced investigators were analyzed using the Mann-Whitney U test for non-normally distributed continuous variables. Differences between the Vscan AirTM and Resona 9 groups were analyzed using the paired Mann-Whitney U test.
The statistical analyses were performed using the statistical software R (v4.2.0; R Core Team 2022). Other R packages that were used for data cleansing, analysis and visualization are: tidyverse [12], dplyr [13], ggplot2 [14] and cowplot [15].
Results
A total of n = 11 participants (n = 4 male, 36.7%; n = 7 female, 63.6%; n = 11 age > 18 years) took part in the survey as part of the course program (corresponds to a response rate of 100%). The epidemiological data are listed in Table 1.
Cohort characteristics [All figures are given as number (%)]
Cohort characteristics [All figures are given as number (%)]
A total of five lesions of different depths (1 cm, 2 cm, 3 cm, 4 cm, 5 cm) were assessed separately by each participant using the scale described above. The measurement results were not normally distributed. From a depth of 3 cm, the scale values regarding the assessment of the target lesions with the Vscan AirTM fell continuously (Tables 2, 3 and Fig. 4) and the delimitability of the target lesions decreased (Figs. 5 and 6). There was no significant difference in the visual delineation of target lesions at different tissue depths between experienced and non-experienced examiners using Vscan AirTM (Table 4).
Quality of visual delineation of the individual lesions during the intervention with Vscan AirTM. The numbers are given as mean value (MW) (SD = standard deviation)
Quality of visual delineation of the individual lesions during the intervention with Vscan AirTM. The numbers are given as median (MD) (Q1–Q3)

Illustration of the delimitability of the lesions depending on their tissue depth before, during and after the intervention with the Vscan AirTM.
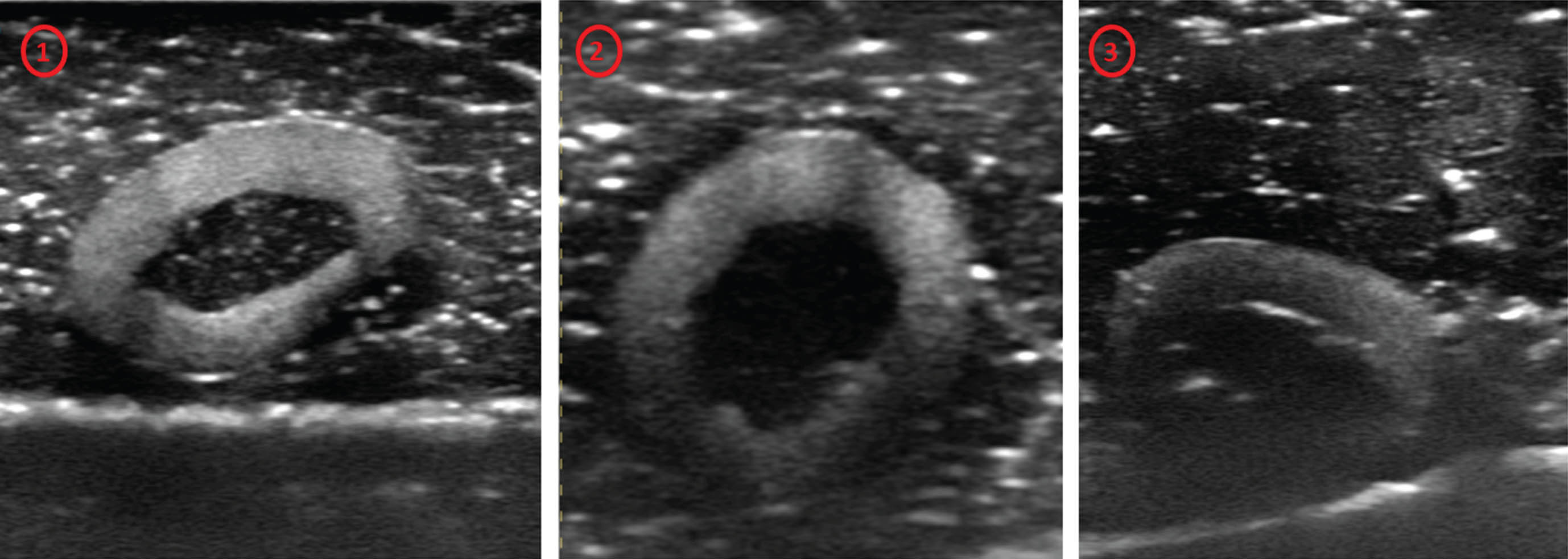
Visualization of the target lesion (olive with filling) with Vscan AirTM: 1) Image quality 5 without relevant limitations. 2) Image quality 3-4, blurring is already visible in the lower part. 3) Image quality 2, clear blurring of the target lesion.
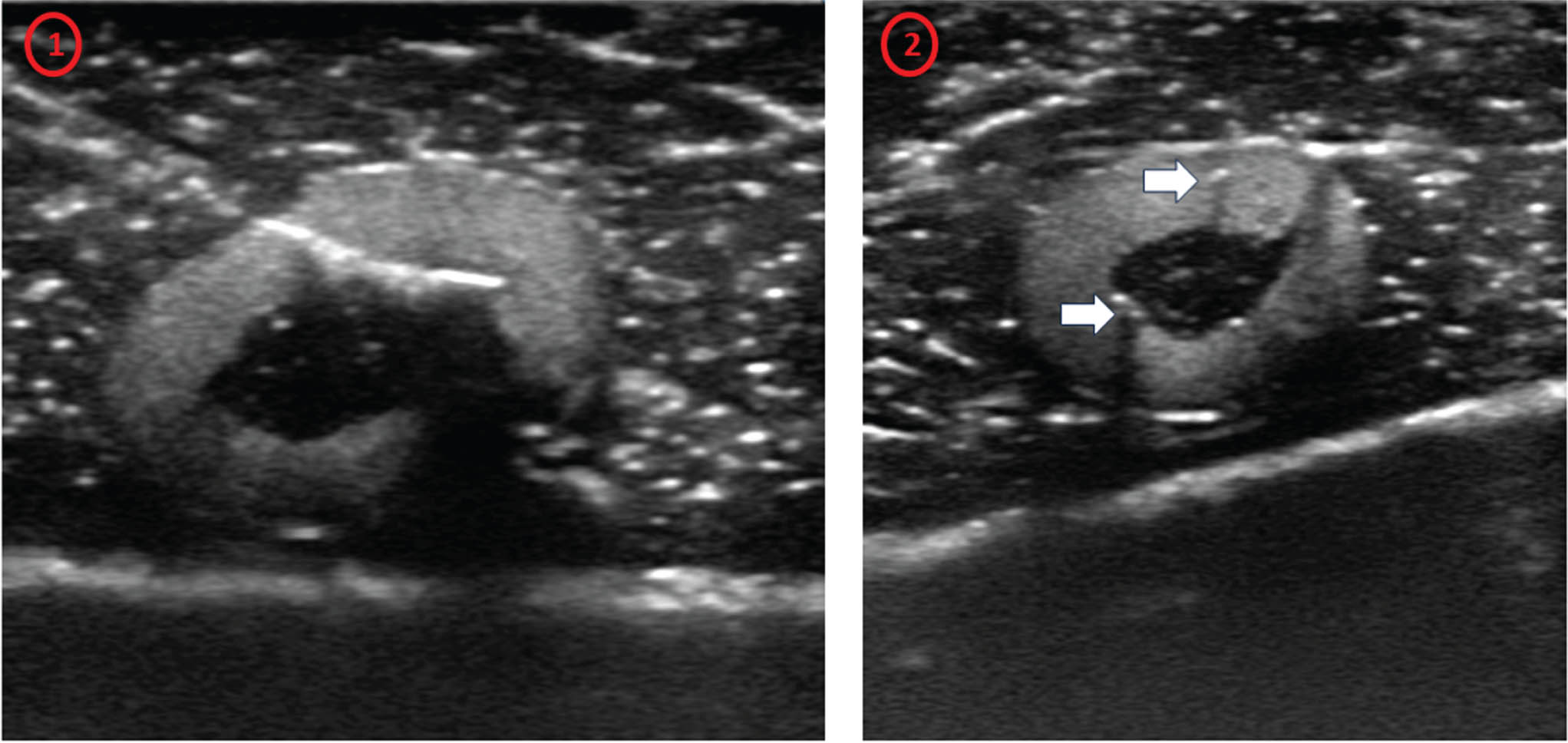
1) Illustration of the biopsy of the target lesion. 2) Target lesion after biopsies; the biopsy marks can be visualized as echo-rich contours in the target lesion (white arrows). The visual delineation corresponds to a 5.
Comparison of the visual delineation of lesions of different tissue depths during the entire intervention process between experienced and non-experienced examiners using Vscan AirTM. The numbers are given as median (Q1–Q3)
In addition to the V-scan, a comparison scan with a high-end device (Mindray, Resona 9) was performed by the participants for all lesions. All participants assessed all lesions with this high-end device in terms of visual evaluation with a 5. In summary, the Resona 9 always proved to be significantly superior to the Vscan AirTM. From a depth of 3 cm, there was even a highly significant result in this respect (Table 5). The assessment of the lesions with the Vscan AirTM is consistently rated with a 4 to 5 up to a depth of 3 cm and only from a depth of 3 cm is there a continuous decrease in the rating scale.
Comparison of the visual delineation of lesions of different tissue depths during the entire intervention process between Vscan AirTM and Resona 9. The numbers are given as median (Q1–Q3)
The initial results of the present pilot study on a wireless mobile handheld ultrasound system appear promising with regard to a training model for ultrasound examiners in training who are interested in interventions. In the in vitro liver model, even those with little experience were able to adequately delineate the target lesions visually and perform punctures under ultrasound guidance with good success. This is supported by the already proven user-friendliness of the Vscan AirTM [16, 17]. However, the success of biopsies depended on the depth of the lesion. In the case of deeper lesions, the biopsy was also clearly dependent on the examiner’s experience, which once again emphasizes the influence of sonographic experience and must be taken into account in addition to other aspects [18].
With the linear part of the mobile probe, a targeted puncture was achieved in all cases with image quality rated as good. The biopsies are still marginal in all cases, although the image quality is sometimes limited at greater depths.
It is more difficult to perform an exact biopsy with the mobile handheld ultrasound system in the lateral puncture direction, a so-called ex plane puncture. If the target lesion could be visualized in the plane of the transducer (in plane), a puncture/biopsy could always be performed accurately up to a depth of 3 cm. In addition to the marginal position, the proximity to septal connective tissue structures in the depth also had a limiting effect on image quality. Here, the targeted puncture with sufficient safety distance in the edge area was not successful in all cases in all planes. This correlates with the experience from other studies on puncture biopsy models [19].
A future step after a puncture/biopsy would be the use of ultrasound-guided ablation techniques such as microwave ablation (MWA). With MWA, the puncture, placement of the probe and monitoring until hyperechogenic structural changes towards the edge of the target lesion are reached can be continuously imaged during the ablation procedure [20, 21]. Compared to a high-end system, however, the precise placement of the probe with the mobile handheld ultrasound – as shown in the present study – is increasingly difficult with deeper lesions. It should be noted that the size of the target lesions in everyday clinical practice may also differ from the lesion size in the present study and that smaller lesions in deeper areas in particular may be difficult to localize.
For a large number of tumors, dynamic contrast sonography has become indispensable for ultrasound-guided biopsies in daily routine. Malignant lesions are often only recognized by a late wash-out [22–24]. In addition, ultrasound-guided CEUS interventions have now also become a decisive diagnostic tool intraoperatively and for further tumor treatments – such as before systemic therapy (e.g. immunotherapy) or for follow-up [1, 26]. However, the additional assessment of the dynamic microcirculation is not possible in a standard in vitro model and requires the development/modification and accompanying evaluation of these models. Now that the CCDS can be used with hanheld ultrasound devices, they can also be used in such models to investigate the flow conditions in the vessels, thus significantly expanding their range of applications.
The network connection for image transmission requires a stable network that guarantees sufficiently fast image transmission in the sense of real-time transmission. The direct connection to a PACS (Picture Archiving and Communication System) system must always take special safety regulations into account, but these have not yet been conclusively clarified.
The in vitro intervention model presented here could also be suitable for future training courses on mobile handheld systems and as an evaluation basis for further studies. An expansion of the group of participants to include students and physican assistants is also quite conceivable, as the use of handheld systems in ultrasound training is adequately possible [27].
However, limitations relate above all to the puncture/biopsy conditions in vitro compared to those in vivo, including any ablation that may have to be performed, with all the risks that this entails. For example, vascular structures with the risk of active bleeding or injuries to bile ducts with the risk of biliomas cannot be adequately simulated in vitro. Also, ultrasound monitoring in vitro in MWA does not include dynamic recording of necrosis formation as in elastography monitoring [28] or monitoring of contrast agent sonography with perfusion analysis [20]. Further evaluation of in vitro models is therefore necessary [29].
Nevertheless, mobile handheld ultrasound and in vitro intervention models can be used as a modern way of establishing future training and research models for the expansion of clinical ultrasound. The development of this technology therefore remains to be seen.
Limitations
A small heterogeneous group was surveyed. Generalizing statements cannot yet be made on the basis of the present study. Only two biopsy needle systems were used. There was no comparison with other models on the market. In addition, this is an in vitro study on a model, which is why no conclusive statements can be made here regarding possible complications or influences when used in vivo. Further studies are essential to answer these questions.
Conflict of interest
FK states consulting activities for Elsevier, Astellas, GSK, MSD, Novartis, Pierre Fabre, Sanofi, AbbVie, Janssen and Servier. UK, EMJ, SK, UVK, WH, CS, CB and ID declare no existing conflicts of interest.
Author contributions
UK: Writing the manuscript, developing the methodology and design
SK: Carrying out the statistical analysis
FK: Supervision
UVK: Review of the manuscript, supervision
WH: Supervision
CS: Supervision
CB: Review of the manuscript, development of the methodology and design
ID: Review of the manuscript, supervision
EMJ: Review of the manuscript, development of the method and design, supervision