
Abstract
It was investigated whether different types of mental or developmental disorders (MDD) would be rated differently in terms of stereotypic perceptions and behavioral tendencies and whether these effects of stereotypes on behaviors would be mediated via emotional responses in line with the Stereotype Content Model (SCM). Furthermore, an experimental investigation sought to ascertain whether predictions about behavioral intentions of bystanders in a cyberbullying scenario towards a victim with MDD could be derived from the general behavioral tendencies as predicted by the SCM. Two-hundred-forty-eight undergraduate students (62% female) aged 18–35 (M = 22.5) were randomly allocated to one of five conditions (anxiety, depression, schizophrenia, Asperger’s, or control). Stereotypes, emotional, and behavioral responses, as well as bystander intentions were assessed. Results largely confirmed the general application of the SCM to MDD; however, this was not the case for bystander intentions in cyberbullying. Implications for the application of the SCM and methodological considerations are discussed.
Cyberbullying has been defined similar to traditional bullying, which is as an act of aggression that is intentional, repetitive, and towards an individual of lower power (Olweus, 1993), but extended to electronic forms of contact (Smith et al., 2008). In most bullying incidents peer witnesses or bystanders will be present. The behaviors of bystanders are a crucial factor for the psychological impact of the bullying event on the victim (e.g., academic performance, depression, suicidal ideation) as well as for prevention and intervention strategies (Salmivalli, 2010). Approving in a passive manner or actively joining in has both shown to reinforce the bully’s behaviours whilst simultaneously negatively affecting the impact of the bullying event on the victim’s mental health. In contrast, when bystanders support or defend the victim this was shown to be effective in stopping the bullies’ behaviours as well as to lessen the negative effects of the bullying event on the victim’s mental health (Hawkins, Pepler, & Craig, 2001; Pepler, Craig, & O’Connell, 2010; Salmivalli, 2010).
This study specifically focuses on the victimization of individuals with mental health difficulties who have been shown to be disproportionately represented as victims in bullying and cyberbullying events (Livingstone, Görzig, & Ólafsson, 2011). For individuals with mental health difficulties, the relation with cyberbullying victimisation is two-fold, i.e. those who are victimised are likely to suffer from mental health difficulties whilst those who suffer from mental health difficulties are likely to be victimised (Gámez-Guadix, Orue, Smith, & Calvete, 2013).
A plethora of research in the tradition of the Stereotype Content Model (SCM) has shown that the content of a group’s stereotype determines the type of discriminatory behavior towards this group (Cuddy, Fiske, & Glick, 2008) whilst the associations of the stereotypes with these discriminatory behavioral tendencies were shown to be mediated via prejudicial emotional responses (Cuddy, Fiske, & Glick, 2007). These range from negative emotions towards outgroups, such as pity, contempt, or envy, to positive emotions usually reserved for ingroups, such as admiration. The behavioral tendencies put forward by the SCM framework can roughly be divided into supporting, aggressing, and ignoring. Similarly, the behaviors of bystanders in bullying scenarios vary between helping, aggressing, or ignoring (Pfetsch, 2016; Van Cleemput, Vandebosch, & Pabian, 2014). Research applying the SCM to social perceptions of those with mental health difficulties or mental and developmental disorders (MDD) has shown that individuals with different types of MDD are perceived differently on the stereotypic dimensions put forward by the model (Fiske, 2012; Sadler, Kaye, & Vaughn, 2015; Sadler, Meagor, & Kaye, 2012). The term mental and developmental disorders (MDD) was employed here to be inclusive of Autism spectrum disorder which has been considered as a mental health problem in terms of stereotypic perceptions (Fiske, 2012), however, clinically it is classified as a developmental disorder and the authors wished to be mindful of this fact in their use of terminology.
In order to guide intervention and prevention strategies, it is important to investigate the underlying mechanism that contribute to different types of bystander behaviours towards individuals with MDD. To fulfill this goal, we employ the theoretical framework of the SCM to explore how different types of bystander behaviors could be explained based on a victim’s group stereotype. Specifically, the current research investigates whether the perceptions of individuals with different MDD that have been associated with different kinds of stereotypes, i.e., depression, anxiety, schizophrenia, or Asperger’s, may predict discriminatory behavioral tendencies towards individuals with a particular MDD and whether this relationship is mediated by prejudicial emotional responses. Following this investigation, it is explored whether the behavioral intentions of bystanders in a cyberbullying scenario towards an individual described in terms of a particular MDD would match the behavioral tendencies as predicted by the SCM framework.
The Stereotype Content Model and the BIAS Map
The Stereotype Content Model (SCM) (Fiske, Cuddy, Glick, & Xu, 2002; Fiske, 2018) proposes that when individuals encounter other people or groups, they assess whether their intentions are helpful or harmful and whether they are capable of enacting them. As a result, two fundamental dimensions have been put forward to systematically explain the stereotypic perceptions of different social groups – warmth (trustworthiness, friendliness) and competence (capability, assertiveness). The combination of these two dimensions create four unique clusters of social groups ranging from low warmth and low competence, low warmth and high competence, high warmth and low competence to high warmth and high competence.
The four different warmth and competence classifications elicit specific types of prejudice in the form of emotional responses which are based on the literature on intergroup emotions (see Cuddy et al., 2008; Fiske et al., 2002): Admiration is elicited by warm and competent groups. This usually applies to members of in-groups, close allies, or members of the culturally default group. Contempt and, for MDD groups also fear (see Sadler, 2015), are triggered by groups considered low in warmth and competence. Typical examples for these groups are drug addicts or the homeless. Pity is associated with groups that are considered warm but incompetent. Examples of these groups are old or disabled people. Envy is directed at groups that are considered low in warmth but high in competence and might be connected to jealousy of rich people, for example.
As an expansion of the SCM, the Behaviors from Intergroup Affect and Stereotypes (BIAS) map has been developed (Cuddy et al., 2007) in order to distinguish discriminatory behavioral outcomes that are connected to the group stereotypes via the related prejudicial emotional responses. Four specific behavioral outcomes are differentiated: active harm (e.g., attacking), passive harm (e.g., ignoring), active facilitation (e.g., helping), and passive facilitation (e.g., cooperating). Warmth is thought to predict active behaviors and competence passive behaviors; whilst high assessments of warmth or competence are linked with facilitative behaviors and low assessments are associated with harmful behaviors (Cuddy et al., 2007, 2008). Consequently, the warmth and competence stereotypes of social groups predict behavioral responses of active or passive harm and facilitation. These associations between stereotypes and behaviors are proposed to be mediated via the emotional responses put forward by the SCM (see Fig. 1 for an illustration); whereby active facilitation (e.g., helping) is linked to high warmth via the emotional responses of pity (low competence) and admiration (high competence); passive facilitation (e.g., cooperating) is linked to high competence via the emotional responses of envy (low warmth) and admiration (high warmth). Further, active harm (e.g., attacking) is linked to low warmth via the emotional responses of envy (high competence) and contempt as well as fear (low competence). Lastly, passive harm (e.g., ignoring) is linked to low competence via the emotional responses of contempt and fear (low warmth) as well as pity (high warmth).
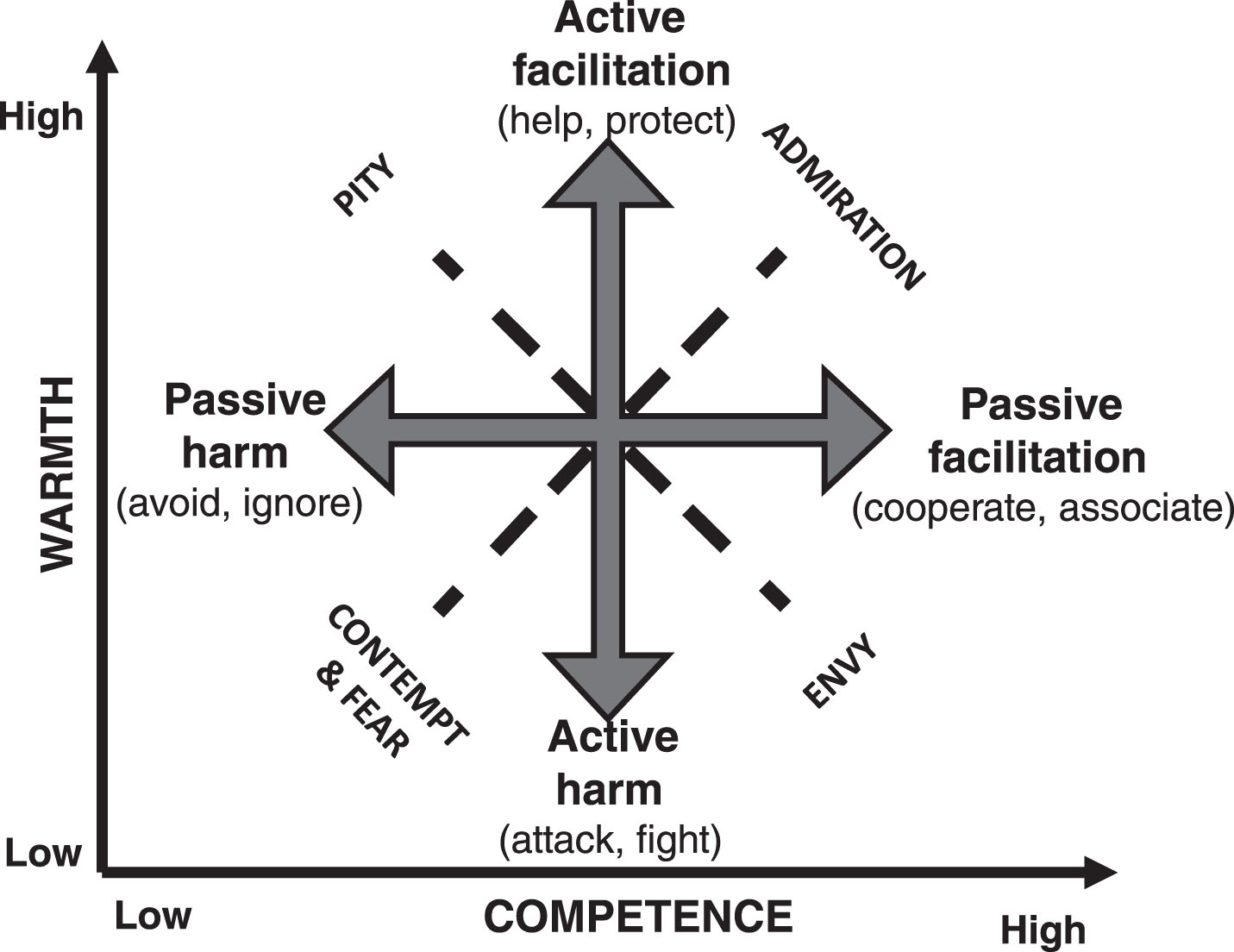
Associations between stereotypes, emotional and behavioural responses when applying the SCM framework towards individuals with MDD (Cuddy et al., 2007; Sadler et al., 2015).
The SCM Framework and People with Mental or Developmental Disorders
In general, people with MDD often experience stigmatization which might have multiple negative outcomes and can differ by type of disorder (e.g., Angermayer, Holzinger, & Matschinger, 2010; Evans-Lacko, Brohan, Mojtabai, & Thornicroft, 2012; Link, Yang, Phelan, & Collins, 2004). The general literature focusing on stigma and stereotypes about individuals with MDD, such as found in the general population or popular culture, has shown that typical representations for each of the three outgroup classifications proposed by the SCM are seen in individuals with depression and anxiety disorders, who are perceived as emotional but not always capable (high warmth, low competence), those with schizophrenia, who are seen as uncontrollable or dangerous as well as often dysfunctional (low warmth, low competence), and those on the autism spectrum, who are often portrayed as lacking social skills but with special talents in other areas (low warmth, high competence) (Jones & Harwood, 2009; Norman, Windell, & Manchanda, 2012; Rohr, 2015; Wood et al., 2014). The current research focuses on these specific MDD in order to cover the range of outgroup stereotypes across the warmth-competence space put forward by the SCM.
The SCM framework has been tested across various countries and contexts (see Fiske, 2018) including MDD (Fiske, 2012; Follmer & Jones, 2017; Sadler et al., 2012, 2015). Further empirical evidence linking those different types of MDD to the SCM framework is inconsistent and will be outlined in the following along with possible implications for the stereotype-behavior link and associated mediational pathways via emotions as proposed by the BIAS map.
Studies employing the SCM framework towards people with mood and anxiety disorders as well as those with depression paint a mixed picture. Those individuals have been perceived as warm and incompetent (Sadler et al., 2015; Amazon Mechanical Turk [MTurk] sample, age: M = 35.62, SD = 13.93) or scoring in the middle of the warmth and competence dimensions (Sadler et al., 2012; MTurk sample, age: M = 35.86, SD = 12.8). Individuals with depression only have been described as cold and average in competence by a student sample (Fiske, 2012) and as cold and incompetent relating to employees (Follmer & Jones, 2017; MTurk sample of US employees). Additionally, for both, individuals with anxiety or depression, stereotypic perceptions of warmth (high) and competence (low) were associated with the behavioral responses of active facilitation or passive harm (i.e., helping or avoidance) and the emotional response of pity; however, the mediational pathways of these stereotype-behavior links via pity in line with the BIAS map have not been assessed (Sadler et al., 2015). The contrasting findings of the stereotypic perceptions (low warmth, low competence) for individuals with depression would, in line with the BIAS map, suggest that they may be associated with emotional responses of contempt and fear and behavioral responses of active or passive harm (i.e., attacking or avoidance); however, those responses have not been assessed (Follmer & Jones, 2017). People with schizophrenia or generic psychopathology have been described as low on both, competence and warmth, across studies (Fiske, 2012; Sadler et al., 2012, 2015) and were shown to evoke both passive and active harm (i.e., ignoring or attacking) via the emotional responses of fear and contempt thereby confirming the predictions made by the BIAS map (Sadler et al., 2015). Stereotypes of autism (this term was participant generated, see Fiske, 2012) spectrum disorder or Asperger’s along with neurocognitive deficits, such as Down Syndrome or Alzheimer’s disease, were considered as relatively warm and incompetent or tending towards mid-warm and mid-competent (Fiske, 2012; Sadler et al., 2015) which in line with the BIAS map would suggest evoking active facilitation or passive harm (i.e., helping or ignoring) via the emotional pathway of pity; again, this has not been assessed as of yet.
In sum, previous research employing the SCM framework to MDD yields findings for stereotypic perceptions in terms of warmth and competence, however, those findings are not always consistent or in line with population based stereotypes and merit further investigation. Behavioral and emotional responses have been assessed for most (but not all) MDD, only one study has assessed the mediational pathways of the stereotype-behavior link via emotional responses; however, those were exclusive to the emotions of contempt and fear and behavioral responses of harm (Sadler et al., 2015); whilst to the best of our knowledge none of those studies has tested the mediational pathways as put forward by the BIAS map (Cuddy et al., 2007).
Bystanders’ Responses to Cyberbullying Link with the BIAS Map
Corresponding to the behavioral tendencies specified in the BIAS map, active and passive behavioral roles have been distinguished when describing the roles of bystanders in bullying events. In relation to the victim of the bullying event, bystander behaviors have been characterised in terms of active or passive facilitation (i.e., defending or supporting the victim) or harmful in an active (i.e., assisting/reinforcing the bully) as well as in a passive manner (i.e., ignoring/doing nothing; Salmivalli, Kärnä, & Poskiparta, 2011; Salmivalli, Lagerspetz, Björkqvist, Österman, & Kaukiainen, 1996). Similar classifications have been adopted by research on cyberbullying which have been proposed to vary between joining in, helping the victim, comforting the victim or doing nothing (Bastiaensen et al., 2014, participants’ age: 13-14 years; Pfetsch, 2016; Van Cleemput et al., 2014, participants’ age: 9–16 years).
We apply the SCM framework to behavioral tendencies of bystanders in cyberbullying events whereby the victim is a member of a discriminated against group such as individuals with MDD (e.g., Angermayer et al., 2010; Evans-Lacko et al., 2012; Link et al., 2004). Consequently, bystander behaviors are thought to correspond to behaviors predicted by the stereotypes held of the discriminated against groups. The behavioral tendencies as specified in the BIAS map (Cuddy et al., 2007) include active facilitation, such as helping, assisting, or defending someone. These types of behaviors directly correspond with bystander roles of defending the victim. Further, active harm refers to aggression, insults, harassments, or hate crimes and can be directly linked with the bystander roles of assisting the bully or joining in. The passive behaviors specified in the BIAS map framework are indirect and covert. These include passive harm which refers to distancing oneself from another in a form of neglecting, excluding, or ignoring and can be linked with the bystander behaviors of ignoring or doing nothing. Further, passive facilitation means tolerated or convenient cooperation or association. Research on bystander behaviors in cyberbullying has also assessed behaviors that show facilitation towards victims in a more passive manner (i.e., comforting or supporting the victim privately; e.g., Bastiaensen et al., 2014). Hence, supporting is used in the current research as a classification of bystander behaviors that correspond to the behavioral category of passive facilitation in the BIAS map.
Aims of the Study
The SCM framework has been successfully applied in prior studies examining the links between different types of stereotypic perceptions, prejudiced emotions and discriminatory behaviors. However, whilst there is some prior research utilizing the SCM framework in relation to MDD, those findings mostly relate to stereotypic perceptions only and are not always consistent. The current study aims to explore the stereotypic perceptions and behavioral tendencies towards individuals with MDD in form of anxiety, depression, schizophrenia, and Asperger’s as compared to a default ingroup. It is then investigated whether a stereotype-behavior link will be mediated by prejudicial emotional responses as put forward by the BIAS map. In addition, it is explored whether the behavioral intentions of bystanders in a cyberbullying event towards individuals with an MDD can be predicted by the group stereotype of the MDD and associated behavioral tendencies as put forward by the BIAS map. Possible predictions for each of the MDD groups in terms of stereotypes and behaviors from previous research outlined above are explored. Mediational pathways for the stereotype-behavior link via emotions are tested in line with procedures outlined by the BIAS map (Cuddy et al., 2007). The specific predictions based on previous empirical evidence for each MDD in terms of the SCM framework as well as associated bystander intentions are outlined in Table 1.
Empirical Evidence for Stereotypic Perceptions of MDD and Associated Predictions for Behavioral Tendencies and Bystander Intentions by the BIAS Map
1Follmer & Jones, 2017; 2Sadler et al., 2012, 2015; 3Fiske, 2012.
Method
Participants and Procedure
Participants were 248 University students (62% female) aged 18–35 years (M = 22.5, SD = 3.64) and from diverse ethnical backgrounds (38% White, 28% Black, 21% Asian, 6% mixed, and 8% other). Thirteen participants with missing responses across response scales were excluded from the analyses. An initial socio-demographic assessment screened out those reporting one of the mental or developmental disorders addressed in this study and those aged over 35 years. The exclusion criteria were in line with ethical guidelines and to ensure the inclusion of young participants in order to ensure similarity in group identification as well as with previous studies in this area.
Participants were approached on the University’s campus and asked to complete a Qualtrics based survey on a portable electronic device. The first part displayed an established cyberbullying scenario on a fake Facebook page (Bastiaensens et al., 2014) which was adapted to describe the victim of cyberbullying in terms of a particular MDD (i.e., anxiety, depression, schizophrenia, or Asperger’s) or as a typical student (control). Each MDD vignette was adapted from the literature (Breheny, 2007; Nevill & White, 2011; PsyWeb, 2015) using case studies and vignettes that were based on the clinical diagnostic criteria of the MDD. These were then rewritten to fit a Facebook page post of the victim, i.e. changed to first person account and reflecting a typical situation in a student’s life on campus which was identical between conditions whilst preserving the traits of the diagnostic criteria associated with each condition. The vignettes were finally reviewed and agreed upon by two of a panel of four independent experts (i.e., mental health professionals; see Fig. 2 for an example and the appendix for the complete wording for each vignette’s Facebook post). The MDD label was not included in the vignettes to adhere to real world conditions as close as possible and acknowledging that the use of a label for vignettes in research on stigma and MDD has not shown to make a difference(Butler & Gillis, 2011).

Cyberbullying scenario for the depression condition.
Participants were randomly allocated to one of the MDD conditions or the control group and asked to read the scenario carefully whilst imagining that they encountered the incident as bystanders whereby the perpetrator and the victim were students from their year group. After viewing the vignette, participants were asked to indicate their bystander intentions and complete a manipulation check measure. Subsequently, an alleged independent second part of the survey was introduced, adopting the research paradigm from the SCM framework (see Cuddy et al., 2007; Sadler et al., 2015). Upon completion, participants were presented with a debrief page and a chocolate bar as an appreciation. Ethical approval was received from the University’sEthics Committee.
Measures
Stereotype content and BIAS map
Participants were asked to complete a series of items assessing stereotypic perceptions, emotional and behavioral responses (Cuddy et al., 2007; Sadler et al., 2015) in line with their allocated experimental condition, i.e. either towards individuals with the particular MDD (i.e., anxiety, depression, schizophrenia or Asperger’s) or as a typical student (control). Likert response scales (1 = not at all; 5 = extremely) assessed all following measures: a) stereotypic perceptions (i.e., warmth: warm, friendly; α= .89; competence: competent, skilled; α= .79), b) emotional responses (i.e., admiration: admiration, inspired by; α= .78; pity: compassion, sympathetic; α= .69; envy: envious, jealous; α= .82; contempt: contempt, disgust; α= .65; and fear: uneasy, fearful; α= .66) c) as well as two facilitative (active, i.e., helping: help, assist; α= .70; passive, i.e., associating: unite with, abide by; α= .62) and two harmful behavioral tendencies (active, i.e. attacking: attack, aggress; α= .76; passive, i.e. avoiding: avoid, distance from; α= .88). In line with the original and frequently replicated research paradigm of the SCM framework the items asked participants to indicate responses from the viewpoint of “society” or “people in general” to prevent a social desirability bias; (see Cuddy et al., 2007; Sadler et al., 2015; for a review of the research paradigm and it’s applications, see Fiske, 2018). The emotional category of fear was an addition to the usual research paradigm. Fear has been established to be a unique emotional response and discrete from anger or contempt in research on MDD stigma, whilst in the BIAS map fear and anger are merged into contempt (see Sadler et al., 2015).
Bystander intentions
Behavioral intention scales aggregated to represent active facilitation (helping, i.e., defending the victim), passive facilitation (associating, i.e., supporting the victim) and active harm (attacking, i.e., assisting the bully) were adopted from Bastiaensen et al. (2014) using items assessing defending the victim (7 items; e.g., “Would you defend [name of victim]?”; α= .79), supporting the victim (12 items, e.g., “Would you comfort [name of victim]?”; α= .87) and assisting the bully (10 items; e.g., “Would you show the picture to others or tell them about it, to make fun of it?”; α= .92). Behavioral intention scales representing passive harm, i.e., demeaning or ignoring, were added (i.e., 4 items; “I would ignore the Facebook post and pretend as if nothing had happened”; “I would try to avoid communicating with [name of victim] via SMS, chat, or e-mail”; “I would try to keep out of [name of victim]’s way at University”, “I would try to avoid communicating with [name of victim] when we are alone, ‘in private’.”; α= .87). Participants were asked to indicate agreement to those items on a scale from 1 (I would definitely not do this) to 7 (I would definitelydo this).
Manipulation check
Participants were asked to indicate for a series of four statements whether they were true or false in relation to the cyberbullying scenario (e.g., “[name of victim] is a happy person.”, “[name of victim] has problems with eating and sleeping.” for the Facebook vignette representing the depressive disorder). Four participants who gave more than two incorrect or less than two correct answers have been excluded from the analyses relating to the cyberbullying scenario only. Given the small number of omissions, procedures for dealing with missing data werenot considered.
Analyses and Results
Stereotype Content
In order to adjust for baseline differences between stereotypes and behaviors across conditions (e.g., participants generally gave higher ratings for active facilitation compared to active harm, across conditions), scales were standardized via z-transformation rendering a grand mean of zero for each scale.
Stereotypes
A 2 stereotype (warmth, competence)×5 condition (anxiety, depression, schizophrenia, Asperger’s, control) ANOVA with repeated measures on the first factor showed a significant main effect for condition, F(4, 230) = 10.27, p < .001, as well as for the interaction term of stereotypes by condition interaction, F(4, 230) = 2.42, p < .05. Planned contrasts showed that all MDD groups received lower ratings from the control group on competence and all but the Asperger’s group received lower ratings from the control group on warmth, t’s(230) = 2.32–5.37, all p’s<.05 (see Fig. 3 and Table 2).
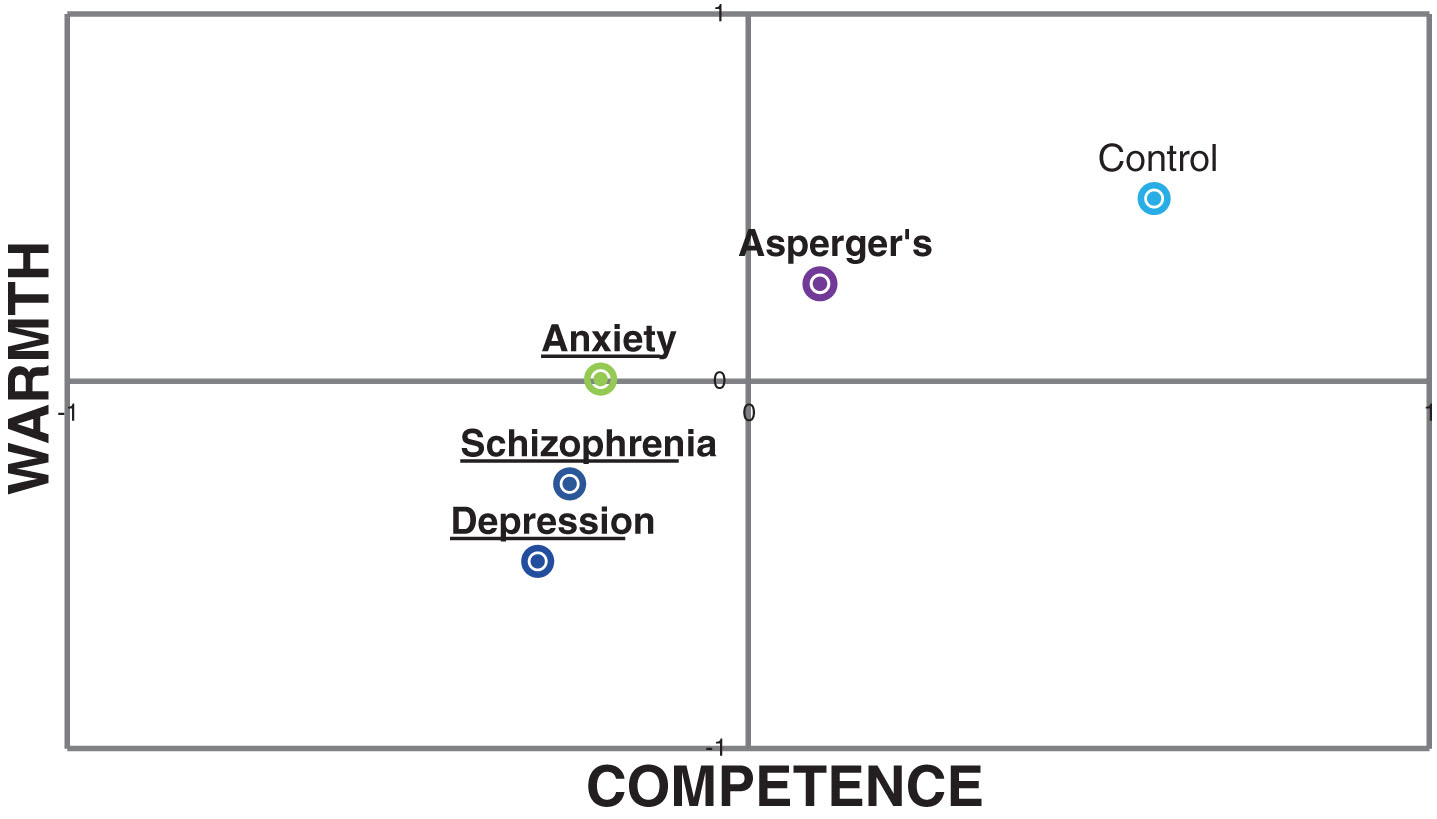
Mean stereotype ratings by condition (z-scores). MDD conditions differ significantly from the control (p < .05) in warmth (underlined) and competence (bold).
Stereotypes and Behavioral Tendencies by MDD Group
Notes. Means sharing a subscript letter differ significantly between groups (all p’s < .05). Means in bold indicate behaviors predicted by the BIAS map for the obtained pattern of stereotypic perceptions.
Behavioral tendencies
For the 4 behaviors (help, associate, attack, avoid)×5 condition (anxiety, depression, schizophrenia, Asperger’s, control) ANOVA with repeated measures on the first factor a significant interaction term emerged for the behavioral tendencies by condition interactions, F(12, 690) = 4.36, p < .001. Planned contrasts revealed that ratings were significantly lower from the control group in helping and associating for the schizophrenia group, and significantly higher from the control group in attacking for the depression and the schizophrenia groups as well as in avoiding for the Asperger’s, depression and the schizophrenia groups, t’s(230) = 1.98–4.46, all p’s < .05 (see Table 2).
Mediational analyses
Subsequent mediational analyses analogues to the BIAS map (Cuddy et al., 2007, p. 640) have been performed using SPSS PROCESS (Hayes, 2012). Results showed that, for facilitative behaviors, competence predicted associating (passive facilitation; β= .19, p < .001) which was mediated by the emotions admiration and envy (total indirect effect = 0.17, 95% CI = 0.098 to 0.258). Further, warmth predicted helping (active facilitation; β= .19, p < .001) which was mediated by the emotions admiration and envy (total indirect effect = 0.13, 95% CI = 0.064 to 0.194). For harmful behaviors, the associations between stereotypes and behavioral tendencies as predicted by the BIAS map, i.e. between competence and avoidance (passive harm) or warmth and attacking (active harm), were not found. However, both types of harmful behaviors were significantly predicted by the emotions fear and contempt (β’s = .19–.54, all p’s<.05)(see Fig. 4 ).

Mediational analyses predicting behavioural tendencies. Coefficients in parentheses represent direct effects. Broken lines indicate non-significant effects; *p < .05; **p < .01; ***p < .001.
Bystander Intentions
A 4 behavioral intentions (defend, support, bully, ignore)×5 condition (anxiety, depression, schizophrenia, Asperger’s, control) ANOVA with repeated measures on the first factor showed a significant bystander intentions by condition interaction, F(12, 678) = 1.8, p < .05. Planned contrasts showed that ratings were significantly lower than for the control group in supporting for the schizophrenic victim and in ignoring for the depressive victim, t’s(226) = 2.11 and 2.3, p’s<.05. No other significant differences emerged (see Table 2). Significant correlations emerged between the bystander and BIAS map behavioral categories for supporting with active and passive facilitation as well as for bullying and ignoring, both with passive facilitation and active harm (see Table 3).
Correlations of Behavioral Tendencies with Bystander Intentions
Note.*p < .05; **p < .01; ***p < .001. Bold correlations were predicted to be significant.
Discussion and Implications
The current study investigated whether individuals with different types of MDD would be rated differently in terms of their stereotypic perceptions and behavioral responses. Further, it was investigated whether the effect of stereotypic perceptions on behavioral responses would be mediated via the emotional responses in line with previous research applying the BIAS map paradigm (Cuddy et al., 2007; Sadler et al., 2015). Moreover, the study set out to experimentally ascertain whether predictions about specific behavioral intentions of bystanders in a cyberbullying scenario towards a victim with an MDD could be derived from the general behavioral tendencies towards individuals with that MDD as would be predicted by the BIAS map.
Findings regarding the link between stereotypes, emotional responses, and behavioral tendencies, employing the BIAS map paradigm were largely but not always in line with predictions made by the model. In line with previous research the anxiety and Asperger’s groups were perceived as low in competence and relatively (compared to other MDD groups) high in warmth (Fiske, 2012; Sadler et al., 2012). In contrast to findings from Sadler et al. (2012) the depression group was not perceived to be high in warmth; however, confirming Follmer and Jones (2017) the depression group was perceived as low in both, warmth and competence. Similarly, and in line with previous findings (Fiske, 2012; Follmer & Jones, 2017; Sadler et al., 2012, 2015) the schizophrenia group was also perceived as low in both, warmth and competence. In terms of behaviors, all groups except for anxiety triggered at least one behavioral tendency in correspondence with their stereotypic perceptions as would be predicted by the BIAS map. The Asperger’s group triggered the expected avoidance behaviors, the depression and schizophrenia groups the expected attack and avoidance behaviors and the control group the facilitative behaviors (i.e., associating, helping) associated with ingroups or close allies (Cuddy et al., 2007, 2008); however, unexpectedly none of the predicted behavioral responses (i.e., helping, avoiding) were statistically significant for the anxiety group.
Both types of facilitative behaviors were associated with the stereotypic perceptions and mediated by the emotional responses as predicted. Active facilitation (helping) was predicted by warmth and mediated via pity and admiration whilst passive facilitation (associating) was predicted by competence and mediated via envy and admiration. For the harmful behaviors (active attacking, passive ignoring) no significant associations with stereotypic perceptions were found and both were solely predicted by the emotions fear and contempt. Interestingly, those are the main predictor emotions as put forward by research on stigma of mental illnesses (Angermeyer et al., 2010; Corrigan et al., 2003) which may suggest that the SCM framework omits specificities concerning some stereotypic subgroups. However, despite the lack of confirmation for the full mediational model, the precedence of emotions over stereotypes in predicting behaviors put forward by the framework (Cuddy et al., 2007) could be confirmed for facilitative as well as for harmful behaviors. By and large these findings confirm predictions made by the SCM framework in terms of stereotypes, emotional responses and behavioral tendencies and extend these towards the specific groups of MDD investigated in this study.
The findings for the bystander intentions did not map onto the expectations derived from the BIAS map and in fact showed little variation across groups altogether. In addition, the correlations between behavioral tendencies from the SCM framework with the behavioral intentions of bystanders did mostly not confirm predictions and showed an inconsistent pattern overall. This may pose important questions in terms of a possible social desirability response bias for the cyberbullying scenario and about the ecological validity of the SCM framework. Several important differences between the BIAS map research paradigm and the cyberbullying scenario that may explain those differential findings must be noted. First, whilst the items for the BIAS map explicitly specify the labels of the target groups, here a particular MDD, this has been operationalized via trait descriptions of the victim in the Facebook vignette in line with DSM-5 criteria of the MDD. Second, the behavioral response scales of the BIAS map items list abstract behaviors (e.g., “Do people tend to help people with [MDD]?”) whereas the bystander intention items specify behaviors in more detail (e.g., “Would you tell someone about the picture, to help [name of victim]?”). Third, the BIAS map items ask participants to answer from the viewpoint of society or people’s behaviors whereas the bystander items ask participants to respond in terms of their own behaviors. In all three cases, the bystander responses may have been associated with a stronger social desirability bias which is perhaps due to the presentation of a more realistic scenario. Therefore, the bystander responses may at the same time yield greater ecological validity than the BIAS map paradigm, that is, social desirability and ecological validity may be confounded in explaining the lack of correspondence between the behavioral responses.
Whilst the Facebook vignettes present realistic scenarios, it is unclear in how far abstract scenarios such as the BIAS map paradigm can be linked to participants’ actual behaviors and emotional responses (Bauman et al., 2014). In particular, participants from diverse and disadvantaged backgrounds, such as in the current sample (University of West London, 2018), may not identify with the society at large as is implied in the response scales used by the SCM framework (Cuddy et al., 2007; Fiske et al., 2002). For this reason, responses about participants own behaviors may differ largely from those made about their believed behaviors of society or people in general, perhaps more so than assumed by previous research employing the SCM framework (Henrich, Heine, & Norenzayan, 2010).
Limitations and Future Research
The present research presents several limitations. As mentioned above, there is a possibility of a social desirability bias, in particular regarding the responses following the bullying scenario which is a common concern in research addressing cyberbullying (Görzig, 2011). Another limitation related to the bullying scenario is the use of a scenario in itself. Using scenarios in research limits the external validity of the studies implications to very specific events outlined in the scenario. Further, given that bullying is a problematic issue for school students or adolescents and mostly researched within this age group, the use of a University student sample in this study, may have had an impact on responses. In particular, given that group identification and dynamics, which can be much more pronounced in adolescence, are an important component within bullying events, especially when they may relate to group norms and stereotypes (e.g., Jones, Bombieri, Livingstone, & Manstead, 2012, participants’ age:10–13 years).
Future research on MDD stigma should investigate the influence of using an MDD label as opposed to a vignette without label but with the MDD trait descriptions. Further, the use of abstract compared to specific behaviors on individuals’ behavioral responses should be explored. In terms of the SCM framework it should be investigated how participant responses may vary if the response scales ask participants to answer from the viewpoint of society or people in general as opposed to specifying their own reactions. It may be of interest whether there is variation in this regard depending on the participant population and their socio-demographic background as well as their identification with societyin general.
Conclusions
The current research has provided additional evidence on MDD stigma against the background of the SCM framework. Stereotypic perceptions as well as the mechanisms which link to behavioral discrimination have been investigated and partially supported the BIAS map approach regarding individuals with MDD. The research further uncovered potential weaknesses of the SCM framework in terms of its ecological validity which demands further investigation. A potential application of the SCM framework linking it with bystander behaviors in a cyberbullying event towards individuals with MDD has been explored. The application of the SCM to this specific and applied scenario could not be supported which may be due to a social desirability response bias, the samples socio-demographic background and a potential lack in ecological validity of the original research paradigm from the SCM framework. Implications for research on bystander behaviors in cyberbullying events drawn from the current research are twofold. Firstly, the difficulty of possible social desirability bias in this research area in general has been reiterated. It may therefore be advisable to combine and or replace research using self-reports with peer or teacher nominations and other types of observational methods, which have been shown to be more reliable (Cornell & Brockenbrough, 2004). Moreover, we can conclude that, although theoretically promising, the SCM framework did not contribute in explaining different types of bystander behaviors based on the victim’s group stereotype as this study set out to do. Due to the possible shortcomings of the theory in terms of ecological validity that may have emerged in this study, theoretical frameworks that have proven to be valid in an applied context should be explored in future research. All of these aspects merit further investigation in future research for which the current study has provided a starting point.
Author Note
We would like to thank our colleagues who served as expert reviewers of the study materials. In alphabetical order they are: Dr. Savin Bapir-Tardy, Dr. Gary Britton, Dr. Michael Broll, and Sally Ferguson. We would also like to express our gratitude to our students who have contributed to the data collection for this project. In alphabetical order they are: Sofia Anjos, Elena Bensoula, Ashlee Campbell, Fion Cheah. Without you this work would have not been possible. This publication was co-written at Masaryk University as part of the project MUNI/A/1204/2018 with the support of the Specific University Research Grant, as provided by the Ministry of Education, Youth and Sports of the Czech Republic in the year 2019.
Footnotes
Appendix
Full text employed for the Facebook vignettes by type of MDD
Anxiety (adapted from PsyWeb, 2015)
I walked around campus today, well pacing back and forth really, I felt extremely restless. I also couldn’t sleep last night. I am really really worried that I might not progress. I can’t stop thinking about this, even at night. During the lecture I suddenly realised that I didn’t even manage to focus on what was being said anymore.
Asperger’s (adapted from Nevil, 2015)
I walked around campus today with my book in-hand as always, I do also like to read it when walking. I didn’t really spend time or talked with other students. I am a good student – but I find it kind of difficult to make friends. People gave me odd looks just because I sat in my chair rocking back and forth which I usually do.
Depression (adapted from Breheny, 2007)
I walked around campus today feeling very down and unhappy. It was very hard to get out of bed, get dressed, go to Uni - or do anything. There is nothing that is fun anymore. I don’t even feel like eating and sleeping is difficult too. I feel completely worthless. Sometimes I think I would be better off dead….
Schizophrenia (adapted from Breheny, 2007)
When I walked around campus today, I felt that others were spying on me and trying to hurt me. I think they could sometimes hear what I am thinking. I could hear voices when no one else was around. And then later, those people on TV were sending messages again, just to me.
Control group
I walked around campus today after the lecture. I met a few other students and chatted with them. I like going to Uni and hanging out with my friends.