
Abstract
Separate lines of research have linked negative parenting practices, victimization, and negative affectivity - separately - with internalizing symptoms in children. However, no previous studies have connected these lines of research to examine internalizing pathology in children. The current study tested complex moderated-mediation models to investigate the respective effects of victimization and negative affectivity on the relationship between parenting practices and internalizing symptoms. Greek-Cypriot children (N = 374) and their parents took part in the study. The children completed the Revised Olweus Bully/Victim Questionnaire, the Negative Affect Scale for Children, and the Parental Bonding Instrument. Their parents completed the Child Behavior Checklist – Parent Report (CBCL). Moderated-mediation models highlighted that negative affectivity moderates the mediating effect of victimization on the relationship between parenting practices and internalizing symptoms. The research findings contribute to the existing literature and advance our understanding of children’s internalizing symptoms development. Implications and future directions are discussed.
Keywords
Internalizing symptoms in children are highly prevalent and associated with considerable impairment in children’s functionality and adjustment (Crawford et al., 2011; Hankin & Abramson, 2001; Rapee et al., 2009). Thus, research has sought to understand the risk and maintenance factors involved in order to contribute to the improvement and development of prevention and intervention programs.
The growth and development of internalizing symptoms in children affect their functionality in various areas of their lives, such as school and social relationships (Buchanan-Pascall et al., 2018; Cosma et al., 2018; Rapee et al., 2009). Epidemiology studies have shown that the incidence of anxiety disorders in children and adolescents ranges between 10 –25%, while depression occurs at a rate of 5 –15% (Crawford et al., 2011).
Parenting Practices and Internalizing Symptoms
Parenting practices have been consistently identified as a risk factor for the development of childhood internalizing symptoms (Degnan et al., 2010). Parenting practices refer to specific behaviors that parents use during the interaction with their child. Such parenting practices can be care, protection, control, discipline, and warmth (de Haan et al., 2009; Hermandez - Guzman et al., 2013; Parker et al., 1979). Researchers have often aimed to identify negative parenting practice behaviors that contribute to the development of internalizing symptoms in children (Coln et al., 2013; Luckyx et al., 2011; Rose et al., 2017; Wood et al., 2003). For example, studies have shown that low parental care, rejection, overprotection, and control contribute to the development of mental disorders in children, such as depression and anxiety (Parker, 1990; Young et al., 2011). Further, research has indicated that children who had an unsafe and unstable relationship with their parents are more likely to develop anxiety and depression (Branje et al., 2010; Warren et al., 1997). The meta-analysis of Pinquart (2017), which integrated research from 1,015 studies on the association of parenting dimensions with internalizing symptoms in children and adolescents, supports these results. Specifically, psychological control, authoritarian, and neglectful parenting were associated with higher levels of internalizing symptoms.
Both cross-sectional and longitudinal studies have found that negative parenting is associated with internalizing symptoms in children (Bukowski & Adams, 2005; Gallagher, 2002; Kiff et al., 2011; Rothbart & Bates, 2006). Given the demonstrated link between negative parenting practices and childhood internalizing symptoms, and the importance of identifying those children who are more likely to develop internalizing symptoms, current research seeks to identify mechanisms through which children develop internalizing symptoms or factors which influence this development. Two mechanisms or factors that have received repeated investigation regarding their relation to parenting practices and internalizing symptoms are child victimization and negative affectivity (Affrunti & Woodruff-Bordern, 2016; Crawford et al., 2011).
Victimization, Internalizing Symptoms, and Parenting Practices
Victimization is one mechanism that is related to both internalizing symptoms and negative parenting practices. Research has often demonstrated that negative parenting practices, such as rejection, alienation, lack of interest and understanding, overprotection, and permissive parenting are related to child victimization (Beran, 2009; Bowes et al., 2009; Dehue et al., 2012; Georgiou, 2008a; 2008b; Lereya et al., 2013; Nikiforou et al., 2013; Papanikolaou et al., 2011; Rigby et al., 2007; Shin & Kim, 2008; Stevens et al., 2002; Veenstra et al., 2005; Wood, 2006). Subsequently, children who are excluded and rejected are at risk for the development of internalizing symptoms. Indeed, research has shown that over time social isolation and victimization were linked to subsequent increases in internalizing problems, like depression, suicidal ideation, anxiety, and emotional problems (Chan, 2013; Cole et al., 2015; Georgiou & Fanti, 2014; Isolan et al., 2013; Lester et al., 2012; Thomson & Leabeater, 2012; Turner et al., 2013; Zwierzynska et al., 2013).
When taken together, results presented suggest that children who interact with parents with negative parenting practices may be at risk for peer victimization, and their victimization may be associated with elevated internalizing symptoms. Despite the separate links between parenting practices, internalizing symptoms, and victimization, only a single study has examined these factors within the same mediation models. Specifically, Ioannidou and Georgiou’s (2021) study showed that negative parental care and overprotection increase the possibilities of a child being victimized, which increases the chances of developing internalizing symptoms. Therefore, this research has proved that victimization can function as a mediator of the relation between parenting practices and internalizing symptoms in children. The present study has re-examined these mediation models considering additionally the impact of a moderating factor, that is negative affectivity.
Negative Affectivity, Internalizing Symptoms, and Parenting Practices
Negative affectivity has been investigated repeatedly and appears to affect the relation between parenting practices and internalizing symptoms. According to Krog and Duel (2003), negative affectivity refers to negative emotional reactions to others and oneself. Several studies have examined the moderating role of negative affectivity on the relation between parenting practices and internalizing symptoms in children (Colder et al., 1997; Crockenberg & Leerkes, 2006; Degnan et al., 2010; Lengua et al., 2000; Morris et al., 2002; Oldehinkel et al., 2006; Rubin et al., 1998). Gilliom and Shaw’s (2004) research showed that the combination of negative parenting practices (high psychological control and low sensitivity/care) and children’s negative affectivity are associated with adaptation problems in these children. Moreover, the study of Morris et al. (2002) found that parents exercise more psychological control over children with negative affectivity, and these children are more likely to develop internalizing problems.
Aims of the Study
Study findings support that negative parenting practices are associated with child internalizing symptoms. This relation is probably related to and influenced by other factors. Two such factors, victimization and negative affectivity, have been separately related to parenting practices and internalizing symptoms. However, no studies have investigated the influence of negative affectivity on peer victimization on the relationship between parenting practices and internalizing symptoms. Since parenting practices may be associated with internalizing symptoms through peer victimization and negative affectivity may interact with such a relation, investigating them within a single model represents an essential addition to the literature. The present study sought to address these issues and investigated parenting practices, internalizing symptoms, victimization, and negative affectivity within single theoretical models. Specifically, the present study investigated how negative affectivity moderates the mediating effect of victimization on the relation between parenting practices (maternal and paternal care, and maternal and paternal protection) and internalizing symptoms in children. We hypothesized that negative affectivity would moderate the mediating effect of victimization on the relation between maternal and paternal care and internalizing symptoms. Additionally, negative affectivity would moderate the mediating effect of victimization on the relation between maternal and paternal protection and internalizing symptoms.
Methods
Participants and Procedure
Participants were 374 children and adolescents, aged 10 to 14 years, and their parents/guardians. As shown in Table 1, 217 children attended the fifth and sixth grade of elementary school, and 157 children attended the first and second grade of high school (M = 12.04, SD = 1.03). Of the 374 children, 174 were boys (46.5%), and 200 were girls (53.5%). Regarding parents’ educational level, 42% of mothers and 40% of fathers had a secondary education, 58% of mothers and 57% of fathers had a university education. 87% of children lived with both parents, 10% had divorced parents, and 3% were single-parent families.
Participants by Gender and Grade
Participants by Gender and Grade
The study was approved by the Cyprus National Bioethics Commission, the Ministry of Education and Culture of Cyprus, the Office of the Commissioner for the Protection of Personal Data, and the schools’ directors. Initially, the researchers gave a sealed envelope to parents/guardians, which included the information leaflet for the purposes of the study, the parental consent form, the parent demographics form, and the parents’ questionnaire. Data collection started after parents/guardians gave their written consent for their child to participate in the study. The children completed the student demographic form and the relevant research questionnaires on the school premises during a lesson.
Parenting Practices
The Parental Bonding Instrument was used to assess parenting practices (Parker et al., 1979). In this self-report questionnaire, consisting of 25 items, the child assesses the behavior of the father and mother separately on a 4-point Likert scale. The questionnaire consists of two scales, care (12 questions) and protection (13 questions), which lead to four different types of parental practices (maternal and paternal care, and maternal and paternal protection). Examples of questions about maternal/paternal care are: “He/she made me feel I wasn’t wanted”, “He/she seemed emotionally cold to me”, and for maternal/paternal protection: “He/she tried to control everything I did”, “He/she was overprotective of me”. The internal consistency was α= 0.88 for the Maternal Care scale, α= 0.81 for the Maternal Protection scale, α= 0.88 for the Paternal Care scale, and α= 0.84 for the Paternal Protection scale.
Internalizing Symptoms
The Child Behaviour Checklist –Parent Report CBCL Scale was used to assess internalizing symptoms - it was completed by the parents (Achenbach, 1991). The questionnaire consists of 113 statements describing their child’s behavior on a 3-point Likert scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true) For the purposes of this study, only the anxiety/depression scale was used. Examples of anxiety/depression items are: “very afraid or anxious”, “crying”, “feeling, complaining that no one loves him/her”. The internal consistency of the scale was satisfactory α= 0.93.
Victimization
The Revised Olweus Bully/Victim Questionnaire was used to assess victimization. It is a self-report questionnaire administered to children from 8 to 16 years of age and consisted of 40 questions and two subscales, one on victimization and one on bullying (Olweus, 1996). However, only the victimization subscale was used in this study. Children were asked to answer on a 5-point Likert scale (0 = not at all to 5 = very valid) whether they have experienced the victimization incident that describes each question in the last month. Examples of items of the victimization scale are: “Someone or some of my classmates taunt me”, “Someone or some of my classmates yell at me some offensive adjectives”. This questionnaire has shown good internal consistency α= 0.95.
Negative Affectivity
The Positive and Negative Affect Scale was used to measure children’s negative affectivity (Laurent et al., 1999). This questionnaire consists of two scales, positive affectivity and negative affectivity. For the purposes of the present study, only the negative affectivity scale was used. The negative affectivity scale includes 15 words describing common negative emotions (sad, frightened, upset, guilty). The child was asked to rate to what extent these negative emotions describe how she/he felt during the last weeks, on a scale of 1 (not much or not at all) to 5 (a lot). The internal consistency of the negative affectivity scale was satisfactory α= 0.93.
Results
Statistical Analyses
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25. At first, descriptive statistics, correlations, and internal consistencies were calculated. Then, the process method was performed in SPSS for the construction of the moderated-mediation models. The moderated-mediation model involves mediation models that require the addition of a moderate factor (James & Brett, 1984). The moderated-mediation model argues that the relationship between predictive variable (X) and variable effect (Y), through an intermediate variable (M), differs depending on the levels of a moderate variable (W) (Langfred, 2004). That is, the effect of X on M and the effect of M on Y is affected by the levels of W.
Descriptive Statistics and Correlation Analyses
The means, standard deviations, and bivariate correlations between the variables are presented in Table 2. As expected, parenting practices, victimization, negative affectivity, and internalizing symptoms were significantly inter-correlated. Multicollinearity did not appear to be infringed, as the Tolerance index was greater than 0.2 and the VIF index was less than 10.
Descriptive Statistics and Bivariate Correlations
Descriptive Statistics and Bivariate Correlations
**p < 0.01.
Four complexes, unique moderated-mediation models were built through the Process method in SPSS to examine the moderating role of negative affectivity in the mediating effect of victimization on the relation between parenting practices and internalizing symptoms. For these four models, Model 58 was used in Process, which allows a moderator (W), moderating the two paths: X ->M and M ->Y, and also moderating the indirect effect of the predictive variable (X) on the effect variable (Y) through the mediator (M).
As shown in Fig. 1 , there was a significant, negative interaction between maternal care and negative affectivity towards victimization, b = –0.44, 95% CI (–0.59, –0.29), p < 0.001. At the same time, a significant, positive interaction between victimization and negative affectivity towards internalizing symptoms, b = 0.07, 95% CI (0.02, 0.12), p < 0.01 appeared. Also, the direct effect of maternal care on internalizing symptoms was statistically significant, b = –0.18, 95% CI (–0.27, –0.08), p < 0.001. Finally, the indirect effect of maternal care on internalizing symptoms through victimization was negatively, statistically significant in children with negative affectivity, b = –0.40, BcaCI (–0.51, –0.30). Thus, the mediating effect of victimization on the relationship between maternal care and internalizing symptoms was moderated by negative affectivity.

Moderated-mediation model. Negative affectivity as moderator in the indirect effect of maternal care on internalizing symptoms through victimization.
In the second moderated-mediation model, as shown in Fig. 2 , a significant, negative interaction between paternal care and negative affectivity towards victimization, b = –0.44, 95% CI (–0.59, –0.28), p < 0.001 appeared. At the same time, there was a significant, positive interaction between victimization and negative affectivity towards internalizing symptoms, b = 0.06, 95% CI (0.01, 0.10), p < 0.05. Also, the direct effect of paternal care on internalizing symptoms was statistically significant, b = –0.16, 95% CI (–0.27, –0.05), p < 0.01. Finally, the indirect effect of paternal care on internalizing symptoms through victimization was negatively, statistically significant in children with negative affectivity, b = –0.46, BcaCI (–0.59, –0.34), showing the moderating role of negative affectivity in the mediating effect of victimization on the relationship between paternal care and internalizing symptoms.

Moderated-mediation model. Negative affectivity as moderator in the indirect effect of paternal care on internalizing symptoms through victimization.
In the third moderated-mediation model, as shown in Fig. 3 , no significant interaction between paternal protection and negative affectivity towards victimization, b = 0.11, 95% CI (–0.01, 0.23), p > 0.05 appeared. However, there was a significant positive interaction between victimization and negative affectivity towards internalizing symptoms, b = 0.05, 95% CI (0.00, 0.09), p < 0.05. Also, the direct effect of paternal protection on internalizing symptoms was statistically significant, b = 0.08, 95% CI (0.03, 0.13), p < 0.001. Finally, the indirect effect of paternal protection on internalizing symptoms through victimization was positively, statistically significant in children with negative affectivity, b = 0.09, BcaCI (0.04, 0.15). Therefore, it appeared that negative affectivity moderates the indirect effect of paternal protection on internalizing symptoms through victimization.
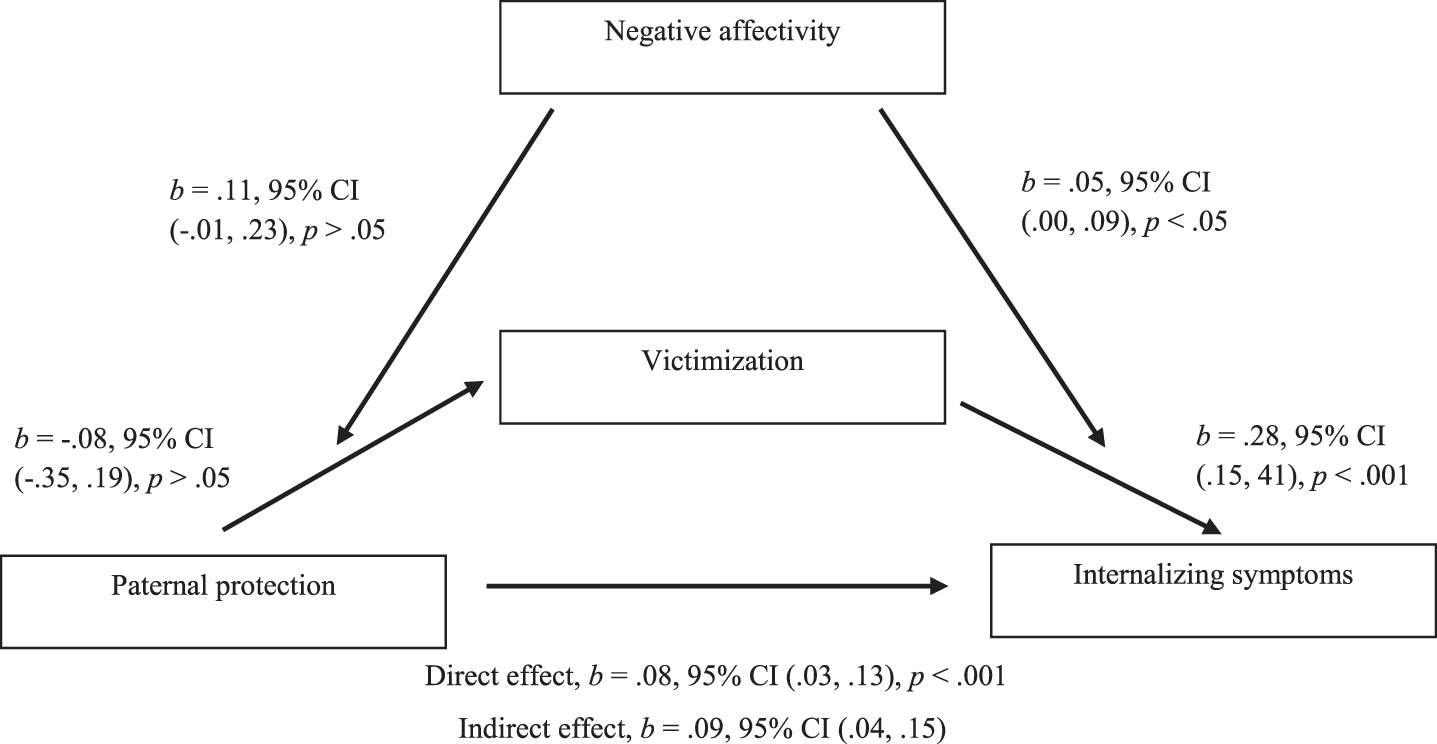
Moderated-mediation model. Negative affectivity as moderator in the indirect effect of paternal protection on internalizing symptoms through victimization.
In the fourth model there was no significant interaction between maternal protection and negative affectivity towards victimization, b = –0.04, 95% CI (–0.20, 0.11), p > 0.05. Also, there was no significant interaction between victimization and negative affectivity towards internalizing symptoms, b = 0.04, 95% CI (–0.01, 0.09), p > 0.05. The direct effect of maternal protection on internalizing symptoms was not statistically significant, b = –0.01, 95% CI (–0.07, 0.04), p > 0.05. The indirect effect of maternal protection on internalizing symptoms through victimization was not moderated by negative affectivity, b = –0.03, BcaCI (–0.14, 0.07), as the confidence intervals included 0. Therefore, it indicated that negative affectivity does not moderate the indirect effect of maternal protection on internalizing symptoms through victimization.
The present study investigated the moderating influence that negative affectivity can have on peer victimization in the association between parenting practices and child internalizing symptoms. Study findings confirmed that negative affectivity moderates the mediating effect of victimization on the relation between maternal and paternal care and internalizing symptoms. This relation indicates that children who interact with parents who show low care, such as rejection and lack of importance, are more likely to be victimized when characterized by negative affectivity, which, in turn, increases internalizing problems in children deriving from victimization. That is, negative affectivity increases the negative impact of victimization, and its consequences in future behaviors. Children displaying negative emotions towards themselves and others are more likely to provoke the reaction of others (Krog & Duel, 2003). On the other hand, low parental care causes even more negative emotions in children, making it difficult for them to feel worthy and to be able to build trusting relationships (Affrunti & Woodruff-Bordern, 2016; Brendgen et al., 2005; Crawford et al., 2011; Crockenberg & Leerkes, 2006; Gilliom & Shaw, 2004; Lengua et al., 2000). These factors increase the risk for children to become a victim of school bullying (Atik & Guneri, 2013; Gómez-Ortiz et al., 2014; Lereya et al., 2013) and to develop internalizing symptoms (Gómez-Ortiz et al., 2014; Lereya et al., 2013; Lester et al., 2012).
Study findings also confirmed that negative affectivity moderates the mediating effect of victimization on the relation between paternal protection and internalizing symptoms. This finding suggests that when children with negative affectivity interact with an overprotective father, they are more easily targeted as victims and therefore develop more internalizing problems. When a father is overprotective with his child, especially if negative emotions and affectivity characterize the child, this seems to result in more negative feelings of the child towards himself/herself (Gilliom & Shaw, 2004; Lengua et al., 2000; Morris et al., 2002). These factors increase the risk for children to become victims of school bullying (Georgiou, 2008a) and to develop internalizing symptoms (Lester et al., 2012; McLeod, Weisz, & Wood, 2007; McLeod, Wood, & Weisz, 2007; Reijntjes et al., 2010).
Contrary to expectations, negative affectivity did not moderate the indirect effect of maternal protection on internalizing symptoms through victimization. It seems that maternal protection results in victimization in children, and their victimization is associated with the development of more internalizing symptoms (Chan, 2013; Cole et al., 2015; Rigby et al., 2007; Stevens et al., 2002; Veenstra et al., 2005; Wood, 2006; Young et al., 2011), but this relation is not affected by children’s negative affectivity. Despite children’s negative affectivity, this finding suggests that when mothers maintain an overprotective attitude towards their children, the latter may have difficulties managing stressful situations and may develop negative feelings about themselves. This - in turn - may increase the risk for children to become victimized in school (Cook et al., 2010; Georgiou, 2008a; Rigby et al., 2007) and develop internalizing symptoms (Isolan et al., 2013; Moore et al., 2017; Turner et al., 2013).
Moderated-mediation models seem to highlight that children’s negative affectivity moderates the mediating effect of victimization on the relation between parenting practices and internalizing symptoms in children. Research has so far examined separately how victimization and negative affectivity are related with the association of parenting practices and internalizing symptoms (Accordino & Accordino, 2011; Affrunti & Woodruff-Borden, 2016; Cole et al., 2015; Crawford et al., 2011; Dehue et al., 2012; Demanet & Van Houtte, 2012; Georgiou, 2008a; Lester et al., 2012; Rigby et al., 2007; Stevens et al., 2002; Tennant et al., 2019; Veenstra et al., 2005). Therefore, results from moderated-mediation models enrich the state-of-the-art. With the help of these models, it is possible to prove that children displaying negative affectivity are more likely to be victimized and develop internalizing symptoms when parents use negative parenting practices.
Limitations and Future Research
The fact that the presented data were gathered from children’s and parents’ self-reports, with, e.g., the latter having probably difficulties with recognizing and accepting their children’s difficulties, could be considered a limitation of the present study. At the same time, all measurements used in this study were questionnaires. Future studies should use various measurement methods, such as teacher report, observation, and interview. Also, the sample characteristics likely reduce the generalizability of the current findings, as the sample comes only from the Greek-Cypriot population. Another limitation worth mentioning is the cross-sectional design of the study. First, due to the cross-sectional nature of the study, no causal inferences about the direction of the relation of variables studied could be made. Second, the cross-sectional nature of the study limits the strengths of mediation and moderation conclusions (Weems & Stickle, 2012). For future studies, it would be helpful to develop more models that simultaneously examine mediation and moderated relations regarding the development of internalizing problems. Further, longitudinal studies would also provide more detail on the developmental course of links between parenting, victimization, negative affectivity, and internalizing pathology.
Conclusions
The present study investigated the effects of parenting practices, victimization, and negative affectivity on child’s internalizing symptoms through complex and unique moderated-mediation models. Findings represent novel insight into the pathways to children’s internalizing symptoms. Specifically, the findings suggest that peer victimization is one mechanism through which children who have parents implementing negative parenting practices may develop internalizing symptoms. However, this mechanism may depend on children’s negative affectivity. These findings may serve to inform parent training as part of prevention and intervention programs for childhood internalizing symptoms.
Footnotes
Bio Sketches
Louiza Ioannidou, Dr., Lecturer at the Department of Psychology and Social Sciences of Frederick University and an accredited School Psychologist. Her research interests mainly focus on bullying and victimization, personality traits, parental bonding, psychopathology, and psychotherapy in children and adolescents.
Maria Zafiropoulou, visiting Professor at the Department of Psychology and Social Sciences of Frederick University and an accredited Clinical Psychologist. Her research focuses on the identification, evaluation, and treatment of cognitive, emotional, and behavior problems in childhood.