
Abstract
With an increasing volume of health information online, it becomes critical for consumers to improve their search and evaluation skills to retrieve reliable information. The Patient Information Aid (PIA) program is aimed to facilitate information seeking, potentially leading to positive outcomes of online consumer health information and the reduction of negative outcomes. This program consists of an educational website based on findings from a systematic literature review and a qualitative research. By teaching information evaluation skills at-the-point-of-search, the general objective of the PIA website is to improve users’ e-health information literacy. Adopting user-centered design methods, we ran two focus groups with users having various literacy levels. We applied usability heuristics and information architecture strategies to design the PIA website, and developed personas and task scenarios to inform the wireframing. In this paper, we share our experience and insights on designing an educational information literacy program, which can be useful for information professionals working in all areas.
Keywords
Introduction
The volume of online consumer health information (OCHI) is ever-growing and may lead to positive health outcomes. For example, consumers may feel better prepared to make informed decisions, to discuss with a health care provider and feel reassured about their management plans (Bianco et al., 2013; Dolan et al., 2004). A recent systematic literature review of randomized controlled trials with a meta-analysis, showed that professional clinical practice may be improved when patients are given health information (Fønhus et al., 2016). However, the quality of OCHI varies, which may also lead to positive as well as negative health outcomes (Amante et al., 2015; Prescott & Mackie, 2017). While numerous studies have examined Internet access, information needs and retrieval, few have focused on information outcomes (Case & Given, 2016) and even fewer looked at the negative outcomes of OCHI use (El Sherif et al., 2018). Based on the results of a systematic review (Pluye et al., 2019) and a qualitative research study (El Sherif et al., 2018), we are designing an educational program, called the Patient Information Aid (PIA). This program consists of a PIA website and is aimed to facilitate information seeking, enable positive outcomes of OCHI, while reducing negative ones.
This paper presents an example of applying user-centered design methods, usability heuristics and information architecture strategies to design an educational program based on empirical findings from a systematic review and a qualitative research. We introduce the PIA website as a tool to improve OCHI outcomes and hope to provide insights for information researchers and practitioners in the field of e-health literacy and other areas.
Background
The e-health literacy construct integrates three dimensions: computer literacy, information literacy and health literacy (Ronson McNichol & Rootman, 2016). These dimensions are interdependent as a person with a low literacy level also has a low level of health literacy, for example. Furthermore, literacy level is defined as the degree to which a person has the ability to acquire, understand, evaluate, and use information needed to obtain services and make appropriate decisions (Kindig et al., 2016).
A systematic mixed studies review uncovered positive and negative outcomes of OCHI, and a qualitative study identified strategies to reduce negative outcomes. The systematic mixed studies review conducted from 2014 to 2017 investigated the key factors and outcomes associated with OCHI for primary care patients (Pluye et al., 2019). The three most commonly-reported factors were health status, health information literacy, and confidence in OCHI. Moreover, higher e-health literacy levels and increased confidence in OCHI were sufficient conditions for reporting a positive outcome.
The qualitative interpretive study conducted in 2015–2016 described the negative outcomes of OCHI and how they can be reduced from the viewpoint of OCHI consumers, health practitioners and health librarians (El Sherif et al., 2018). In this study, 19 OCHI consumers, seven health practitioners, and three health librarians were interviewed and described their experience with negative OCHI outcomes. Results suggested that a new construct “tensions of OCHI use” has three dimensions: internal, interpersonal and service-related. Moreover, we identified strategies for reducing negative outcomes to be implemented before information search, during the search, and after finding relevant OCHI.
A conceptual framework of OCHI outcomes.
As a result of these review and study, we proposed a conceptual framework (see Fig. 1) of OCHI outcomes (Pluye et al., 2019), and suggested that negative outcomes may be reduced when consumers are supported in searching, assessing and discussing OCHI with their social networks and health professionals (El Sherif et al., 2018). Based on these research findings, we are designing the PIA website as an educational resource for informing consumers how to search, assess and apply OCHI. The general objective of the PIA website is to improve users’ e-health information literacy, i.e., their ability to acquire, understand, evaluate, and use information needed to obtain services and make appropriate decisions.
According to the revised Bloom’s taxonomy (Anderson et al., 2001), the specific educational objectives of the PIA website are to improve users’ knowledge (better recall health-related data and information), comprehension (better understand the meaning, and interpretation of health-related problems and recommendations; and state them in their own words), evaluation (make better judgments about the value of health-related ideas, materials and services), and application (better use health-related ideas, materials and services in current and new situations). We believe that these educational objectives are complementary to the growing volume of OCHI and lists of credible consumer health information websites vetted by health librarians.
Aligned with the qualitative study (El Sherif et al., 2018), the PIA website has been designed to assist users before, during and after searches. Before information search, it provides tips (e.g., how to use Boolean operators) and links to trustworthy and up-to-date lists of reliable sources (e.g., the Medical Library Association’s list of websites). During the search, it provides an evaluation checklist based on Health on the Net (HON) standards to help users evaluate the quality of information retrieved. After finding potentially relevant and reliable information, it teaches users how to save and share information with relatives and health professionals.
We adopted a user-centered approach to design the PIA website, involving users with various e-health literacy levels. User-centered design sees user goals as the real target and considers user data as the main factor for design-related decision-making (Saffer, 2010). This approach helps to uncover diversified user needs, while reducing researchers’ biases and preferences. Our five key steps were: (1) conducting two focus groups with users, (2) developing personas and task scenarios based on the collected data, (3) wireframing by researchers, mobilizing findings from Steps 1 and 2, (4) usability testing on the wireframes with users, and (5) developing and implementing the website with developers. We involved users early in the design process to pinpoint their needs, goals, and preferences, and we always kept users in mind as guided by user-centered design principles (Saffer, 2010). Actively engaging users in design helped us to understand their workflow related to seeking OCHI and the vocabulary most meaningful to them. Meanwhile, we approached design as an iterative process instead of a linear one, meaning we would go back to earlier steps to restart the design cycle as needed.
The first focus group took place in February 2018 with participants having a higher level of literacy. Seven PhD students, researchers and support staff from McGill University’s Department of Family Medicine participated. The focus group lasted 1.5 hours and included a discussion of key issues and workflows of searching for OCHI, as well as an unstructured (open) card-sorting activity. In June 2018, we ran a second focus group with five participants having a lower level of literacy. The participants were all mothers with a lower socioeconomic status, who use the internet regularly for OCHI. It also lasted 1.5 hours and included a structured (closed) card-sorting activity. Beginning with open card-sorting enabled us to brainstorm labels for website content and start organizing them into categories, while the following closed card-sorting provided participants with existing labels and categories and provoked their thoughts on refining the website structure (Rosenfeld et al., 2015). A semi-structured script was developed in consultation with an academic librarian specializing in user experience (EG) and used in both cases. Each focus group had three parts: an introduction and general questions, a card sorting activity, and wrap-up discussions. The first group was conducted in English and the second in French. Both focus groups were audio recorded and summarized in English. All participants were compensated for their time.
The findings from focus groups informed the development of personas (i.e., descriptions of typical types of users) and task scenarios (i.e., real-life use cases) enabling us to better understand how users might think and what they would like to accomplish (Cooper et al., 2014). Our personas covered users with higher, moderate and lower e-health literacy levels. The scenarios included searching health information for various age groups and different healthcare topics (see Table 1). Three personas combined with about six scenarios showcased the main purposes and functions of PIA website. This coverage should sufficiently inform the development of wireframes (using Axure RP8
Personas and task scenarios for different e-health literacy users
Personas and task scenarios for different e-health literacy users
The two focus groups established user requirements and provided insights on website content selection and development, helping us understand what is important and helpful to users. Both user groups expressed a preference for images, video and audio tutorials instead of long text, emphasizing the importance of providing concise information. For example, one participant said: “Just the information on a page, black and white, …is not interesting”. The higher literacy level group expressed concerns related to validating and triaging the information, as well as dealing with different types of search results (e.g., forums or blogs). Participants in this group described the following searching practices: starting with Google or Wikipedia, checking the institutional affiliations of websites and authors, paying attention to the writing (e.g., well-written text with proper sentence structure and no grammatical errors). This group also raised issues related to information sources, discerning the severity of symptoms, understanding how to access the healthcare system, and including non-Western biomedical knowledge.
The lower literacy level group also reported starting the search with Google and specifically mentioned using fewer and simple terms in their searches. The participants demonstrated some awareness of searching for different formats (e.g., images) and the ranking of search results by search engines, about which they want to learn more. They acknowledged that searching and evaluating could be time-consuming, sometimes getting lost or disoriented among tabs and websites. They welcomed a repertoire of reliable local websites, as well as a list of unreliable sites to be avoided. They stressed the importance of being able to provide feedback on our website and the expectation of receiving quick responses, and revisions when applicable.
In addition, the lower literacy level group mentioned their dislike for constant scrolling. The underlying problem is not the lack of mobility or knowledge to operate a mouse or touchpad observed in older adults (Hawthorn, 2000), but users’ reluctance to read and process endless information presented to them. For example, participants complained about “too much information” and asked for “more structured information”. Therefore, we aimed to keep our content succinct and structured to minimize scrolling. Finally, participants in both groups described searching for information for family members, children and aging parents.
Guided by usability heuristics in interaction design (Nielsen, 1994) and information architecture strategies (Rosenfeld et al., 2015), we developed the personas, task scenarios, and wireframes to better organize and present the PIA website content. Based on previous work (El Sherif et al., 2018; Pluye et al., 2019), the PIA website design concerns three searching stages: before, during, and after searching. Based on focus group findings, the stages were labeled and explained as follows: “HELP YOU SEARCH – How to find information”, “HELP YOU EVALUATE – How to validate search results”, and “HELP YOU USE – How to put information into action” (see Fig. 2).
PIA website homepage wireframe.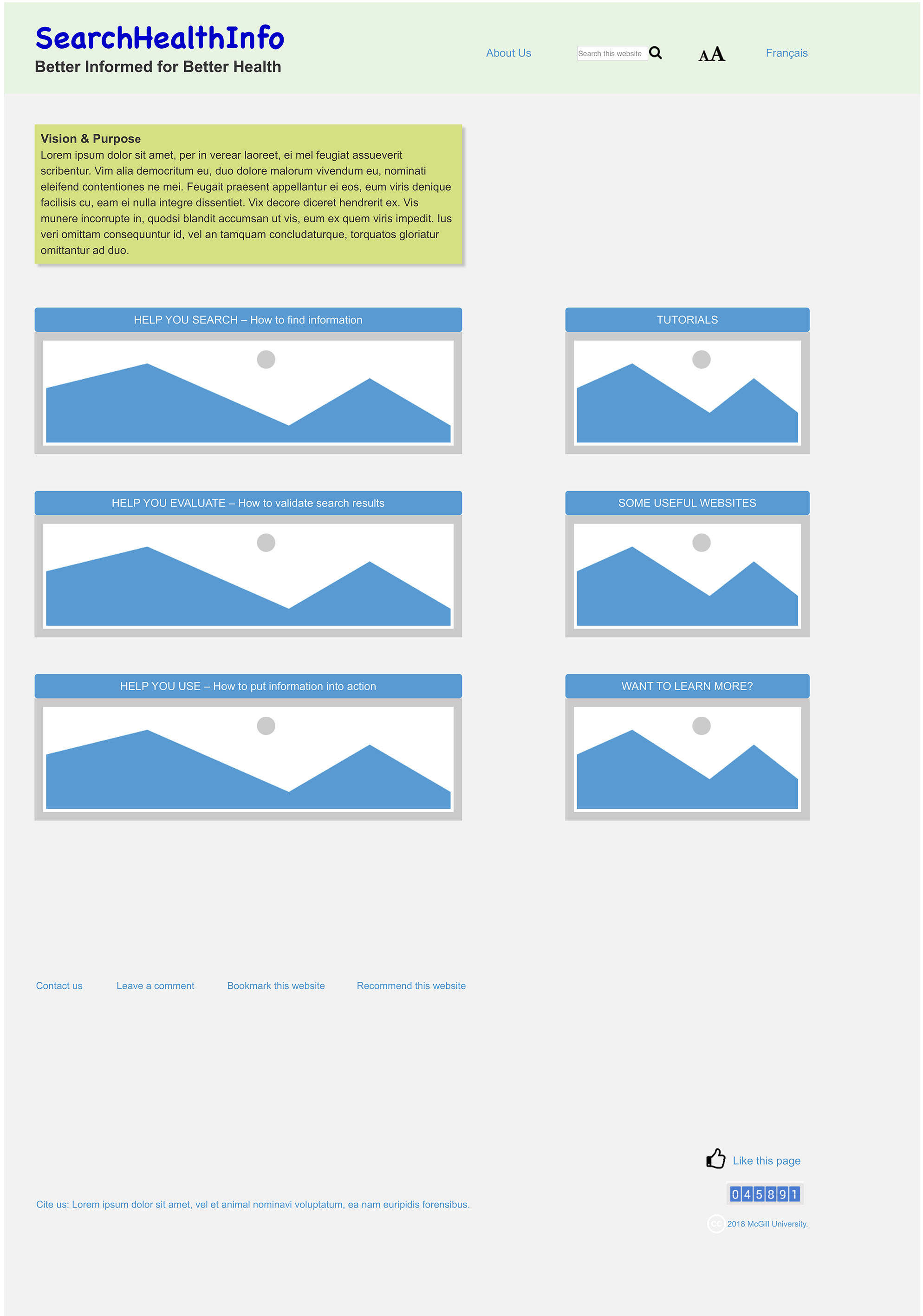
We applied information architecture principles on navigation, labelling, and search systems, including being consistent and user-centric, using both textual and iconic labels, avoiding jargon, and keeping it simple and focused (Rosenfeld et al., 2015). For example, we proposed a search system with autocomplete and autosuggest functions as a part of the global navigation (i.e., present on every page) and clearly labelled it as “search this website” to avoid the possible confusion with an Internet search engine.
Our findings confirmed that the PIA website should include searching tips, explanation of how search engines work, the discussion of different types of websites, and audio and video content. In addition, focus groups provided examples of the usefulness of the heuristics of speaking the users’ language, using the words and concepts familiar to the user instead of system-oriented terms, following real-world conventions, and arranging information in a natural and logical order (Nielsen, 1994).
In line with other usability heuristics, the PIA website will provide immediate and appropriate feedback on clicks or mouse-overs to make the system status visible and clear to users at all times. It will offer a search field on every page and a quick link to all the tutorials on the homepage to minimize users’ memory load and to promote recognition rather than recall. It will include brief hints on mouse-overs as necessary help and documentation in case users need extra explanation of the functions (Nielsen, 1994).
Next steps
Once the interactive HTML medium-fidelity wireframes of our website are completed, we plan to run usability tests with 6–12 new users having lower, moderate, and higher levels of e-health literacy. Each participant will be asked to explore the wireframes on a computer and complete one or two user tasks, which will be presented in real-life situations from previously-developed personas and task scenarios. We will encourage the participants to think aloud during the tasks and to discuss their likes and dislikes about the wireframes after the tasks. The usability testing results will help us finetune the wireframes, leading to the implementation of the PIA website.
The first version of the website will focus on content in French and English, in partnership with organizations providing information on child development, education and health (“Naître et grandir” in Quebec, and “It doesn’t have to hurt” across Canada). Future versions may include more languages and have a broader scope. Meanwhile, we will explore ways of promoting our website via information professionals (at hospitals, universities, and social service units), public librarians, related websites, newsletters and magazines, patient groups, associations, and practice-based research networks.
Footnotes
Acknowledgments
We gratefully acknowledge the ongoing support of our panel of experts: Malik Altakrori, Fabio Balli, Maria Cristiane Barbosa Galvao, Isabelle Marie Vedel, Francesca Frati, Sophie Desroches, Burnand Bernard, and Roland Grad.