
Abstract
Immunotherapy is now at the forefront of cancer therapeutic development. Gliomas are a particularly aggressive form of brain cancer for which immunotherapy may hold promise. Pritumumab (also known in the literature as CLNH11, CLN-IgG, and ACA-11) was the first monoclonal antibody tested in cancer patients. Pritumumab is a natural human monoclonal antibody developed from a B lymphocyte isolated from a regional draining lymph node of a patient with cervical carcinoma. The antibody binds ecto-domain vimentin on the surface of cancer cells. Pritumumab was originally tested in clinical trials with brain cancer patients in Japan where it demonstrated therapeutic benefit. It was reported to be a safe and effective therapy for brain cancer patients at doses 5–10 fold less than currently approved antibodies. Phase I dose escalation clinical trials are now being planned with pritumumab for the near future. Here we review data on the development and characterization of pritumumab, and review clinical trails data assessing immunotherapeutic effects of pritumumab for glioma patients.
Introduction
The history of antibody therapeutics for cancer treatment has morphed from an exciting and promising beginning to one with profound disease modulation [1]. Considering current advances, it seems likely that new approaches will be developed and employed as therapeutic protocols mature. Early successes in the field were primarily restricted to individual monoclonal antibodies (mAbs) or to monotherapy. Currently, promising cocktails of therapeutic mAbs are being developed [1], driven by the natural human immune response that is neither monoclonal nor polyclonal but rather oligoclonal [2]. Based on available preliminary evidence and the principles of immune biology, the use of mAbs as oligoclonal cocktails (mixtures of 2–4 mAbs) for treating human diseases, including cancer will likely be effective [2]. Antibody combinations could significantly reduce or, in some cases, largely replace cytotoxic chemotherapy, which is standard of care in many oncology treatments. After surgical resection of solid tumors, systemic chemotherapy and now mAb therapy [3] is improving survival and quality of life in patients. Newer delivery platforms and approaches to antibody-drug-conjugates (ADCs), either alone or in conjunction with immune modulation may prove to be viable alternatives in therapeutic management of cancer. Also, combination approaches with traditional chemotherapies or targeted therapeutics are also showing promise in various cancers.
Current technology is capable of developing therapeutic antibodies to any particular epitope [4, 5]. Cancer patients can generate tumor-specific B lymphocytes which can be isolated to develop human mAbs against tumor-associated antigens. In cancer, the best source of anti-tumor antibodies is from sentinel lymph nodes [6, 7]. Pritumumab, the therapeutic antibody reviewed here, is a classic example of a natural human anti-cancer antibody. It is a natural human IgG1 kappa antibody developed by the human hybridoma technology, using the human UC729-6 fusion partner and B lymphocytes isolated from a regional draining lymph node of a patient with cervical carcinoma [8]. In the literature, this pritumumab mAb is also referred to as CLNH-11, CLN-IgG, or ACA-11 [9]. Pritumumab was shown to exhibit high specificity and binding to brain tumor cells including glioblastoma (GBM), as well as to low grade astrocytoma and anaplastic (malignant) astrocytoma [9]. Due to rapid diffuse infiltration of individual tumor cells into the surrounding brain parenchyma before its clinical diagnosis, gliomas are an aggressive and difficult to treat disease. For these reasons, median survival of GBM is about 15 months, and 5-year survival rate is about 3% [10]. Due to the high specificity and binding to brain cancer cells and the unmet need of effective therapy, pritumumab was tested in multiple clinical trials in Japan to treat 249 brain cancer patients. Results of the clinical trials showed there was a 9-fold benefit to patients treated with pritumumab compared to standard therapy of care [9].
Pritumumab likely represents a natural immune response to tumor antigen [3, 4], and clinical trials suggest it has anti-tumor activity [5]. In the original patient from whom the B lymphocyte was isolated, the bioavailability of the target antigen induced a natural immune response resulting in the generation of the pritumumab IgG. This review summarizes the various findings of pritumumab, the first human monoclonal antibody used to treat cancer patients, and highlights its effectiveness in patients with gliomas.
Characteristics of pritumumab
Development and preclinical studies of pritumumab
Clone generation. Pritumumab was secreted by a human-human hybridoma generated by fusing a B-lymphocyte from a regional draining lymph node of a cervical carcinoma patient, with UC-729-6, a human lymphoblastoid B-cell line [2]. This clone was originally designated CLNH11, also referred to as CLN-IgG, and ACA-11; the World Health Organization (WHO) designated this antibody as pritumumab, a human IgG1 kappa antibody. Hybridoma subclones secreting pritumumab were generated for high secretion and adapted to grow in serum-free media [11, 12]. The antibody used for clinical trials in Japan was generated in serum-free media and purified under GMP conditions. Subsequent to this, primarily for economic reasons, a recombinant form was made and expressed by CHO cells [13]. Clone generation, specificity analyses, and general properties of pritumumab have been described in detail previously [9] including its antibody-dependent cellular cytotoxicity (ADCC) and complement-dependent cellular cytotoxicity (CDCC) activities [14, 15].
Using both cell lines and tissue samples, the specificity profile of pritumumab demonstrates its immunoreactivity to primarily tumor tissue and cancer cells, but not to normal cells and tissues of various histologic types, in enzyme immunoassay (EIA) and immunohistochemistry (IHC) [9, 16, 17]. Pritumumab was reported to show immunoreactivity with malignant gliomas, particularly GBM, anaplastic astrocytoma, and craniopharyngioma, but not to normal adult or fetal brain tissue or other extraneural tissue in both formalin-fixed and frozen sections [9].
Pritumumab demonstrated high ADCC activity (36%) against primary cultured cells from various types of GBM and anaplastic astrocytoma tissues and cells, but a low activity (
Antigen characterization
Under non-reducing conditions, purified pritumu- mab reacts with a molecular weight of 226,000 from A549 lung cancer cells [18, 19]. However, under reducing conditions, purified pritumumab reacts with two chains of molecular weights 60,000 and 53,000, from different cell lines including A549. Scatchard analysis showed pritumumab affinity of 4.5
IHC summary of tissues using the original hybridoma-derived pritumumab
IHC summary of tissues using the original hybridoma-derived pritumumab
Vimentin is a member of the intermediate filament (IF) family of structural proteins and is ordinarily not exposed on the cell surface [20]. Though the exact mechanism is as yet unknown, EDV has been shown to be expressed only on the surface of certain cells that are in some way metabolically altered, including a variety of cancer cells [9, 13]. The amino acid sequence of the EDV version is identical to vimentin but the configuration of the C2 core region creates a new epitope that is not present on native vimentin. As such, pritumumab does not recognize vimentin derived from normal cells.
The binding of colloidal gold-conjugated pritumumab to EDV expressed on U251MG cells was analyzed using electron microscopy [22]. The colloidal gold-pritumumab particles were restricted to the outer leaflet of plasma membrane on several blebs around the root of podosome-like projections on the leading edge of the cell. These data suggest that part of the U251MG cell population have special cytoconstituents on the plasma membrane that are bulb-formed architecture (ectosome protrusion) and the EDV molecule can be expressed over the surface of its membranes. It was reported the surface expression of EDV was increased at G2/M phase of the cell cycle [22]. However, the cytophysical function of this expression of EDV is still unclear.
Immunohistochemical analysis with horseradish peroxidase (HRP)-conjugated pritumumab on various tissue sections revealed strong positive staining in brain, breast, cervical, colon, liver, melanoma, and pancreatic cancer tissue sections, and no reactivity was seen in normal uterine smooth muscle sections. In addition, normal brain cells and blood vessels were negative. Normal adult and fetal brain tissues were negative by IHC. These data are summarized in Tables 1 and 2.
IHC summary of brain tumors using the original hybridoma-derived pritumumab
Cases of recurrent malignant glioma treated with radiolabeled pritumumab
*All cases were treated previously with radiotherapy, chemotherapy (ACNU) and interferon; **Survival time from the first treatment of radiolabeled pritumumab (R-mAb); # Average dose of 15.0 Gy; Gb: Glioblastoma; MA: malignant astrocytoma; PR: Partial response, NC: no change, PD: progressive disease.
Six weeks after implantation of 10
Clinical studies
Pritumumab has been tested extensively in clinical trials in Japan. All patients recruited for these studies in a drug washout period – off therapy for at least one month prior to their first dose of pritumumab. All recruited patients were appropriately consented at their respective hospitals.
Pritumumab treatment protocols. The Food and Drug Administration proposed that the amount of DNA contained in a single injection of a biotherapeutic should be 10 pg or less. After GMP purification from the original hybridoma clone, 6–8 pg of DNA were detected in every mg of pritumumab antibody. Based on this, the maximum dose of pritumumab was set at 1 mg per administration, since this dose would not exceed the mandated 10 pg of DNA [24]. Pritumumab concentration was kept constant, but the frequency of administration was varied, either once or twice weekly.
Phase I: In a Phase I setting [24, 25] pritumumab was administered IV or directly into the tumor once or twice weekly for 4 weeks, to 17 patients with malignant glioma to assess safety. In 2 out of the 17 cases, adverse events were observed; one patient showed elevated liver enzymes (glutamic oxaloacetic transaminase, GPT; and glutamate-pyruvate transaminase, GOT) on day 3 and the other showed a slight fever and a reduction in leukocytes after week 1. Both patients recovered by week 6, in spite of continuing treatment. In all other cases, no marked changes were observed; so it was determined that no particular problems were observed regarding the safety of pritumumab under the conditions of the study. From these studies it was determined that the half-life of pritumumab in the serum was approximately 73 hours.
In one case in which a patient received pritumumab directly into the tumor, a reduction of tumor size was observed; no reduction in tumor size was observed in the other direct tumor injection cases. In one case of IV treatment, a reduction in tumor size was observed at 13 weeks after continuous treatment of pritumumab. No clear conclusion regarding the route of administration could be obtained from this study [24].
Early Phase II: Since no major toxicities were observed during the Phase I study and since two patients exhibited a measurable reduction in tumor size, an early Phase II study was conducted at multiple clinical sites to examine the efficacy and safety of pritumumab in patients with malignant glioma over a longer administration period [26].
Similar to the Phase I dosing, pritumumab was administered in the early Phase II study at a dose of 1 mg once or twice weekly over a period of 24 weeks [26]. Although only 50% of cases receiving twice weekly pritumumab were evaluated for efficacy (21/42) and the number of death and drop out cases was high due to the specific characteristics of malignant gliomas, the efficacy rate (partial response, PR or better in terms of reduction in tumor size) was 38.1% (19.1% of all cases). Median survival was 23 and 34 weeks, with hazard ratio 2.157 and 95% confidence interval [CI], 0.9 to 5.2,
Contemporaneous survival analyses demonstrate median survival ranging from 4.5–18 months for malignant glioma/anaplastic astrocytoma (average, 7.9 months), and 2.9–7.6 months for glioblastoma (average, 5.7 months). A meta-analysis of 40 clinical trials of glioblastoma/anaplastic astrocytoma revealed a median survival of 6 months with 1 drug, and 7.8 months with 2 drugs. Further, efficacy rates for glioblastoma and malignant astrocytoma were 36.4% and 28.6%, respectively, suggesting that pritumumab is effective in these two kinds of tumors. Compared to that, malignant glioma patients had a median survival of 23.3 months (1 mg once weekly pritumumab) and 15.3 months (1 mg twice weekly pritumumab), with average median survival of 19.3 months. Similarly, for patients with glioblastoma, pritumumab treatment resulted in median survival of 5.75 months (1 mg once weekly pritumumab) and 8.5 months (1 mg twice weekly pritumumab), with average median survival of 7.1 months.
Japanese clinical trial summary data on pritumumab. Glioblastoma patients treated at 1 mg/kg had a median survival of 23 weeks. Glioblastoma patients treated at 2 mg/kg had a median survival of 34 weeks. Malignant astrocytoma patients treated at 1 mg/kg had a median survival of 93 weeks. Malignant astrocytoma patients treated at 2 mg/kg had a median survival of 61 weeks. Astrocytoma patients treated at 2 mg/kg had a median survival of 107 weeks.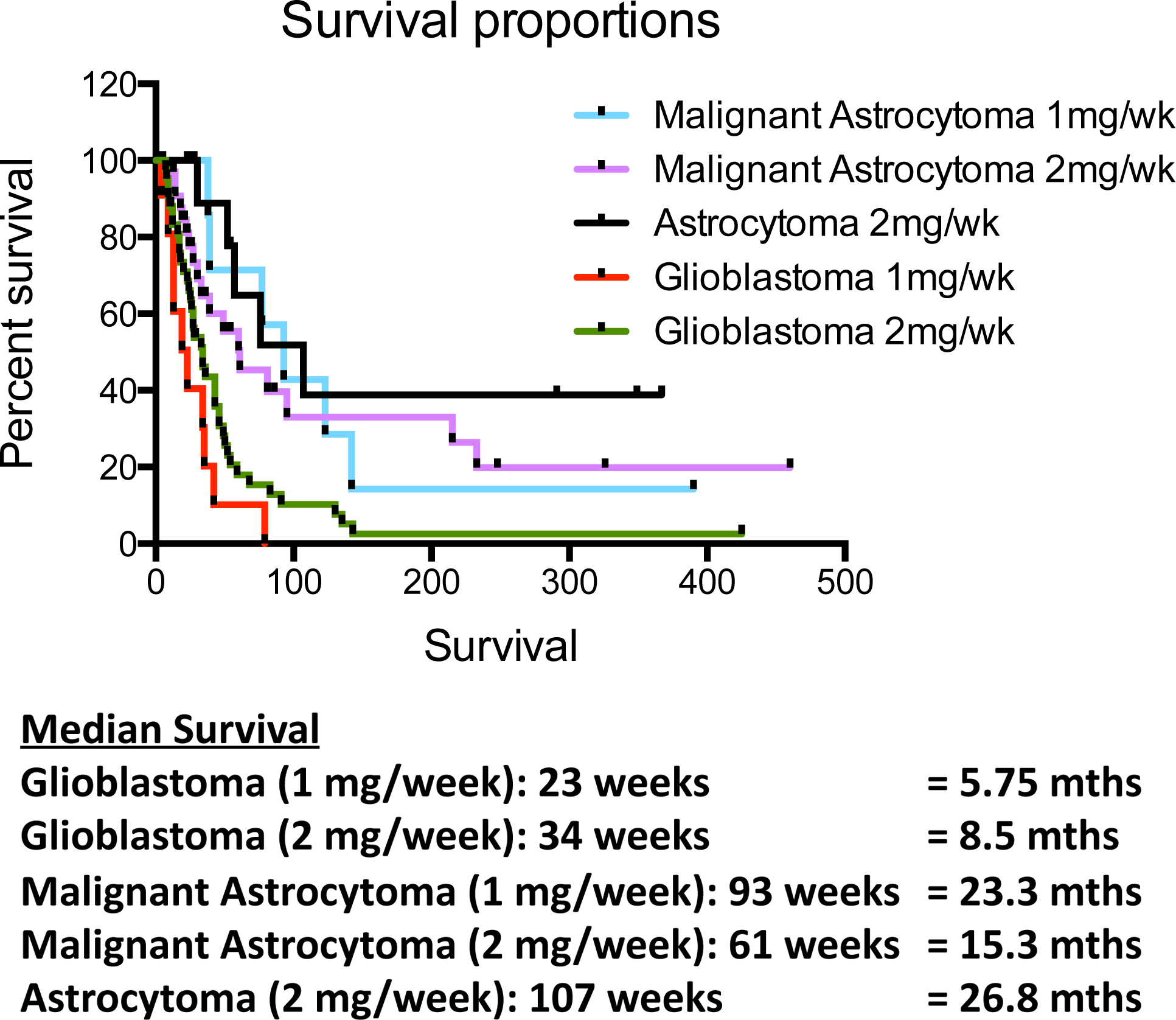
Subjective and objective symptoms (adverse effects) were observed in 5 cases (number of adverse reactions 13; incidence of adverse reactions, 11.9%) out of the 42 cases that were enrolled in this study. All of these adverse reactions were minor and disappeared without intervention during continuous treatment of pritumumab. In addition, no obvious relationship between the age of the patient and the affect of pritumumab on tumor shrinkage, total number of pritumumab administrations and tumor shrinkage or total dose of pritumumab and tumor shrinkage were observed. These results suggest that pritumumab is effective in glioblastoma and malignant astrocytoma when administered once or twice weekly and no major toxic events were associated with pritumumab administration.
Late Phase II: Since the incidence of adverse reactions during the 24-week early Phase II trial administration period of pritumumab was low, and as no severe adverse reactions were observed, pritumumab was judged to be safe and permitted to start late Phase II studies [27]. The primary purpose of the late Phase II study was to confirm dosage and administration requirements of pritumumab determined in the early Phase II study in a larger number of cases.
In 45 of 67 cases that were assessed for the late Phase II trial, the efficacy rate (PR or better, using the rate of reduction of tumor size as end-point) was 17.8% (8/45). The efficacy rate in terms of MR or better was 26.7% (12/45). In total assessment, the efficacy rate in terms of neurological symptoms and performance status were 8.9% and 11.1%, respectively. Compared by histological diagnosis, high efficacy rates were observed for malignant astrocytoma (26.3%, 5/19) and astrocytoma (37.5%, 3/8). In contrast, in patients with glioblastoma, very few cases of PR of better were observed. Stratified analysis of patient background factors and efficacy of pritumumab revealed a significantly higher efficacy in primary brain tumor patients than in recurrent brain tumor patients.
Adverse reactions were observed in 5 of 67 patients assessed for the safety of pritumumab (number of adverse reactions, 10; incidence of adverse reactions, 7.5%). During the 24-week treatment with pritumumab, 18 patients died (due to enlargement of tumor or pneumonia) and in 26 cases, treatment was discontinued. The overall results of these studies suggest that pritumumab has a clinical anti-tumor effect on gliomas [27]. Furthermore, treatment with pritumumab was considered to be safe as no severe adverse drug effects resulting from pritumumab treatment were observed.
In conclusion, this late Phase II study demonstrated the anti-tumor affect and safety of twice weekly IV administration of pritumumab at a single dose of 1 mg for 24 weeks in patients with malignant astrocytoma [27]. The 2-doses per week group had better clinical outcomes than the 1-dose per week group, suggesting that a higher dose may be more effective. The five-year survival data with a Phase II group of 39 brain cancer patients [27] had an overall survival rate of 28%, which is a 9-fold benefit over standard care.
In a targeted radioimmunotherapy study [28, 29], pritumumab labeled with
Anti-idiotype response: To monitor the development and occurrence of an anti-idiotypic response in patients treated with pritumumab, a murine anti-paratactic antibody to pritumumab was generated and verified by computational modeling [29, 31]. This anti-idiotype can monitor the immune responses in pritumumab-treated patients. When the antigen-mimicking anti-idiotypic antibody can be induced in the treated patients, it can elicit anti anti-idiotypic antibody, which behaves like pritumumab [29, 31]. Repetitive treatment with pritumumab induced a pritumumab-like antibody in responders. Based on the data, pritumumab-treated patients who developed an anti-idiotypic response demonstrated improved survival compared to those who did not develop an anti-idiotypic response. Those who responded with either stable disease to moderate, partial, and complete responses did develop an anti-idiotype response, and those patients who had progressive disease did not develop an anti-idiotype response. It is useful to measure the idiotypic antibody response in patients who are responding to antibody-specific therapy. Clinically, the presence of an anti-idiotypic antibody response suggests the patients who receive antibody-based therapy could rebuild a host anti-tumor response. This information likely suggests a mechanism of anti-tumor effect and immunity through antigen-antibody binding. An anti-idiotype response is a reflection of the natural immune response and may provide clues as to mechanisms of action.
Pritumumab likely has disparate mechanisms of action (MOA). At low doses (as used in the clinical studies described in this review), an anti-idiotype response was observed. Typical antibody therapy uses several hundred milligrams per dose and at this level, traditional MOAs of ADCC and CDC are observed. This suggests that the dose of antibody could dictate the MOA. Lower dose, as seen with pritumumab, likely induce an anti-idiotypic response, where higher doses lead to a tolerized anti-idiotype response, with ADCC/CDC effector functions driving anti-tumor effects.
Conclusions
As a natural human antibody derived by human hybridoma technology, pritumumab shows highly specific binding to EDV, selectively expressed on cancer cells, primarily glioblastoma and other primary brain cancers. Pritumumab was tested in clinical studies against gliomas. Evaluation of the efficacy of pritumumab indicated that 14.8% of glioblastoma patients, 26.8% of malignant astrocytoma patients, and 44.4% of astrocytoma patients benefited from therapy. Importantly, no major adverse drug effects were seen and no severe host reaction to the administered antibody was observed making long-term repetitive treatment reasonable. Taken together with specific reactivity, permeation, and accumulative properties as well as safety, these data suggest that pritumumab is useful for the treatment of gliomas.