
Abstract
With the flourishing of innovation in drug discovery into a new era of personalized therapy, the use of monoclonal antibodies (mAbs) in the treatment of various ailments lies at the forefront. Major improvements in genetic sequencing and biomedical techniques as well as research into mAbs emphasize on determining new targets for advanced therapy while maximizing efficacy for clinical application. However, a balance has to be achieved concerning developing a target with low toxicity combined with high specificity and versatility, to allow a specific antibody to facilitate several biotic effects, ranging from neutralization of virus mechanisms to modulation of immune response and maintaining low global economic cost. Presently, there are approximately 30 mAbs’ permitted for therapeutic use with many more being tested in clinical trials. Nevertheless, the heavy cost of mAbs’ production, stowage and management as well as the subsequent hindrances to their development are outweighed by mAbs’ clinical advantages. Compared to conventional drugs, since mAbs use as pharmacologic iotas have specific physical features and modes of action, they should be considered as a discrete therapeutic category. In this review, the history of mAb generation and the innovative technological applications of mAbs that has advanced in clinical practices is reviewed.
Introduction
Since 1980s, therapeutic monoclonal antibodies (mAbs) have emerged into helpful and lucrative group of discoveries. Currently, mAbs encompass the mainstream of recombinant proteins presently utilized in clinics, with approximately 150 products under research sponsored by companies worldwide. Starting with the most idea generated in academe, biotech firms forged numerous technologies and methods to generate beneficial mAbs, despite several failures. Although initially, most pharmacological firms were averse to accept the innovative tools, most now incorporated the use of many mAbs in scientific research. Collectively, genetically-developed mAbs generally have advanced possibilities of approval success as compared to small-molecule drugs, and are therefore useful for diversification of the therapeutics pipeline.
The first mAb was developed in 1975 and was fully licensed in 1986. The developments of mAbs represent a novel way in target specific mutations and defects in protein structure as wells as their expression in a wide range of diseases where chronic ailments are aimed. Nowadays, with key innovations in genomic sequencing and the transformation of elementary therapeutic research into clinical practice, humanized mAbs are a rapidly rising group of recombinant molecules in clinical trials [1]. The global value of the antibody market is approximately $20 billion per year [2] with about 30 mAbs currently approved by the FDA for human use in the treatment of various diseases and conditions including cancer, transplantation, chronic inflammatory diseases, infectious and cardiovascular diseases [3]. In fact, antibodies have become popular and vital research tools in many techniques including western blotting, immunohistochemistry, immunocytochemistry, enzyme-linked immunosorbant assay (ELISA), immuno precipitation and flow cytometric analysis. In addition, antibodies are also being considered for clinical therapies, including suppression of the immune system following organ transplantation [4, 5], in the treatment of cancers such as leukemia and inhibition of angiogenesis [6].
History
In 1984, Kohler and Milstein were awarded the Nobel Prize in appreciation of the prominence of their contribution to the improvement of invention means for mAbs. The discovery occurred in 1975, when normal antibody-producing B-lymphocytes were fused with myeloma tumor cells; resulting in clones of cells termed as hybridoma’s [7]. Since their first production, a completely new era in biotechnology has been initiated. The general technique which is known as ‘hybridoma technology’ proved to be a wide range of mAbs which can bind to protein, carbohydrate, nucleic acid and hapten antigens, and may even have catalytic activities [8]. These lead too many practical application for mAbs to be applied in research or in health care [9] leading to some patent disputes [10].
Generation of mAbs using the hybridoma technique
The technology has been enhanced over the years, particular by pre-selection of antigen-binding B-cells and by screening with antigen-coating filters [11]. Hybridoma technology was first extended to somatic cell genetics, allowing mutant antibodies to be selected [5]. Their functional properties are transformed by interchanging heavy chain constant regions and antibodies to be made with twofold higher specificities [12]. The gene technology later transformed the potential antibody genes which can be further altered. New vistas seemed to be reviving the elapsed anticipation of the old discipline i.e. antibody immunochemistry. Initially, antibody genes were acquired from hybridoma cloned into plasmid vectors and was expressed as complete antibody in mammalian cells [13] in bacteria segments [14]. The easy manipulation of genes using new technologies by cutting and pasting of restriction fragments, or by site mutagenesis, allows the construction of new antibody reagents and fine mapping of antibody structure-function relationships.
Flowchart illustrating the production of mAbs by a hybrid technology.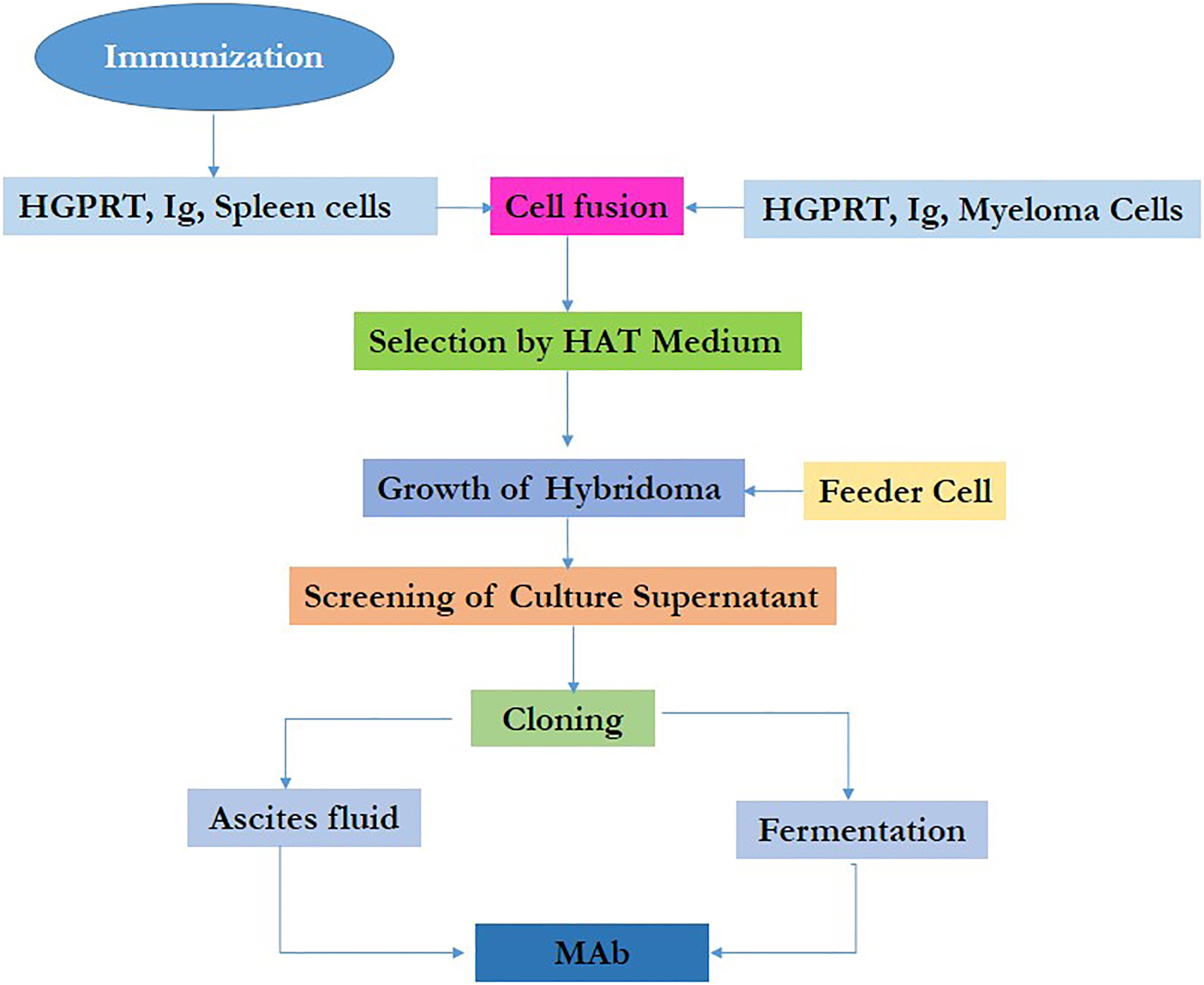
Additionally, a new approach is also proposed with the aim of bypassing hybridoma [15]. Antibody genes are cloned directly from the lymphocytes of immunized animals and are expressed in bacteria, following which the antibody produced is screened for binding antigens [16]. As does hybridoma technology, the process relies on animal immunization to yield many antigen-specific cells. In animals, antibodies of low affinity first produce antigen-induced cell proliferation followed by the generation of high affinity variants as a result of point mutation and selection.
The generation of hybridoma involves immunization of a certain species against a specific epitope on an antigen and obtaining the B-lymphocytes from the spleen. The B-lymphocytes are then fused (either by chemicals or by virus-induced methods) with an immortal myeloma cell line lacking the hypoxanthine-guanine-phosphoribosyltransferase (HGPRT) gene but not containing any other immunoglobulin-producing cells. These hybridoma cells are then cultured in-vitro in selective medium (i.e. medium containing hypoxanthine-aminopterinthymidine) where only the hybridoma’s (i.e. the fusion between the primary B-lymphocytes and myeloma cells) survive. The survival occur as they have inherited immortality gene from the myeloma cells as well as selective resistance from the primary B-lymphocytes (since myeloma cells lack HGPRT, they cannot synthesize nucleotides de novo as this is inhibited by aminopterin in the selective medium) [17]. The initial culture of hybridoma’s contains a combination of antibodies derived from many different primary B-lymphocyte clones, each secreting its own individual specific antibody into the culture medium (i.e. the antibodies remain polyclonal). Each individual clone can be separated by dilution into different culture wells. The cell culture medium can then be screened from many hundreds of different wells for the specific antibody activity required. Subsequently, the desired B-lymphocytes grown from the positive wells are then re-cloned and retested for their activities [18]. The positive hybridoma’s and mAbs generated can then be stored in liquid nitrogen. Hybridoma technology can immortalize these cells while gene technology immortalizes genes. In both cases however, it is an animal that ‘invent’ the new molecule Fig. 1.
There are several required components for enhancing antibody efficacy including immunogenicity, antigen-binding affinity, effector functions and pharmacokinetics. Immunogenicity involves minimizing non-human sequences by creating chimeric, humanized or human versions of the antibodies with the presence of as few T-lymphocyte epitopes as possible [19]. The antibody fragments are usually less immunogenic due to a lack of Fc domain [20]. Antigen-binding affinity can be further improved by using phage display libraries to isolate antibodies with strong affinities for the antigen. However, sometimes antibodies with a lower affinity for the antigen may be required to allow better tumor penetration [21]. Effector functions can be improved by genetically engineering the Fc region to contain point mutations or glycan modifications. Yamane-Ohnuki and Satoh reported the development of defucosylated antibodies, which have higher affinities for the low affinity immunoglobulin gamma Fc region receptor III-A (FcgRIIIa) receptor and enhanced antibody dependent cell-mediated cytotoxicity (ADCC) [22]. A particularly interesting aspect of antibody efficacy is its unique pharmacokinetic characteristics once the particle reaches inside the body. For example, it has been noted that the bioavailability of IgG in plasma is partially dependent on its interaction with the neonatal Fc receptor (FcRn) named Fc/Brambell receptor [23]. The FcRn functions as a salvage receptor that leads to the rescue of immunoglobulin G (IgG) internalized in cells from degradation by lysosomes thus causing recycling of antibodies into the plasma and prolonging its half-life [24]. The plasma half-life of IgG can also be increased by developing antibodies (e.g. through phage display) with increased affinity for FcRn [25]. In addition, antibody fragments treated with polyethylene glycol (PEG) have also been shown to have an increased plasma half-life [26].
Beneficial modifications to mAbs
MAbs can also be modified for additional effects. Teicher and Chari discussed the possibilities of creating conjugated antibodies by coupling effector mole-cules to mAbs (e.g. plant or bacterial toxins, enzymes, radionuclides and cytotoxic drugs) [27]. Chemical coupling of effector molecules to mAbs is usually done with the aid of chemical ligands (i.e. joining molecules). The sites for coupling on the mAbs usually include thiol groups (e.g. eSH groups on cysteine residues), amine groups (e.g. eNH2 groups on lysine residues) or carbohydrates. Additionally, cysteine, lysine or carbohydrate attachment sites can be added anywhere into mAbs using site-directed mutagenesis, although the function of the monoclonal antibody must be maintained [28]. For example, an antibody bound to a toxin can be targeted against a tumor. This can also be produced by genetic engineering where a DNA sequence coding for the specific toxin can be added to the end of the single-chain variable fragment (scFv) chain region in the genome in order that they co-transcribe [29]. Bispecific antibodies can target two separate epitopes with each arm of the Fab portion. They can be produced by chemical cross-linking of IgG, Fab or scFv fragments or via the generation of a ‘hybrid hybridoma’ [30].
MAbs as drugs: The current status
To date, more than 100 different monoclonal antibody diagnostic products are currently available [31, 43] with some listed in Table 1. They are used not only
Commercial available mAbs in the market
Commercial available mAbs in the market
for routine diagnostic procedures but also for therapeutic purposes in larger quantities. The use of mAbs in biomedical research has been and will continue to be important for the identification of proteins, carbohydrates, and nucleic acids. Their use has led to the elucidation of many molecules that control cell replication and differentiation thus advancing the knowledge on the relationship between molecular structure and function. These advances in basic biological sciences have improved our understanding of host response to 1) infectious-disease agents and toxins produced by these agents 2) transplanted organs and tissues 3) spontaneously transformed cells (tumors) and 4) endogenous antigens [32]. MAbs are important reagents used in biomedical research, microbiological research, in the diagnosis of hepatitis, acquired immune deficiency syndrome (AIDS), influenza, herpes simplex, and in the treatment of chronic diseases such as infections and cancer [33]. These antibodies are produced by the cell lines or clones obtained from animals (in-vivo and in-vitro).
MAbs form the basis of a number of diagnostic tests when used in-vitro. For example, mAbs against a hormone can detect pregnancy only ten days following conception. Specific mAbs are used for rapid diagnosis of hepatitis, influenza, herpes simplex and chlamydia infections. MAbs play an important role in diagnostic medicine to determine the concentration of specific proteins in blood or urine. For example, an unusually high blood level of a prostate-specific antigen, indicated by its interaction with a mAbs, can provide an early warning that an individual may have developed prostate cancer. Additionally antibodies can also be used in protein purification. When a purified antibody is added to a crude mixture of proteins, the specific protein being investigated selectively combines with the antibody and precipitates from the solution thus allowing detection [34].
It has been nearly 30 years since Kohler and Milstein described a technique for immortalizing antibody producing cells, identifying their products and cloning the cells to obtain mAbs. MAbs are important diagnostic reagents used in biomedical research and for the diagnosis of viral and bacterial diseases. The production of mAbs is neither straightforward nor easy. The common production steps are immunization of mice and selection of mouse donors for generation of hybridoma cells, screening of mice for antibody production, preparation of myeloma cells fusion of myeloma cells with immune spleen cells, cloning of hybridoma cell lines by “limiting dilution” or expansion as well as stabilization of clones by ascites production purification of mAbs, antibody engineering for ligand binding and diagnostic kits preparation. These mAbs are produced either in vitro or in vivo. The modern attractiveness of mAbs is almost directly related to the advancement of recombinant mAbs technology. There are approximately 100 different diagnostic kits based on mAbs technology currently available in the market. The worldwide markets of the clinical diagnostics are estimated to be approximately $19 billion, with an annual growth rate of nearly 5% per year.
Commercial issues surrounding mAbs
Some of the relative lack of commercial success of mAbs may be attributed to the high costs of its administration. For example, in leukemia treatment, it costs approximately £37,000 for a year’s supply of alemtuzumab [35]. Furthermore in cancer treatment, antibodies are rarely, if ever, curative. For example, bevacizumab (avastin
Applications of mAbs in diagnosis and treatment
Once mAbs for a given drug or substance have been produced, they can be used for the detection of the substance of interest. The western and immune dot blot tests detect the protein on a membrane. They are also very useful in immunohistochemistry, which detect antigen in fixed tissue sections and immunofluorescence test by detecting the substance in a frozen tissue section or in live cells [38, 39]. Besides being a source of pure antibody for diagnosis of infectious diseases, mAbs provide a means of:
Enumeration of human lymphocyte sub populations
For this purpose, anti-CD3 (cluster of differentiation 3) identifies all mature T cells, anti-CD4 (cluster of differentiation 4) identifies subsets containing T-helper cells while anti-CD8 (cluster of differentiation 8) identifies cytotoxic T cells.
Analysis of viral antigens
MAbs are used in the classification and diagnosis of viral diseases with the best example as the dissection of the antigenic structure of the influenza virus. MAbs have been used against the hemagglutinin glycoprotein exposed on the surface of the viruses and these antibodies can neutralize the virus. In this way, every antigenic drift or shift can be identified. MAbs are used to map areas of antigenic variation on the virus particle. Such functional mapping has also been done for polio virus and certain retroviruses.
Analysis of putative protective antigens
MAbs can define antigen structure and help identify certain antigenic determinants that evoke a protective immune response. Non-immunodominant determinants can also be identified and their reactivity analyzed. With the help of mAbs, synthetic peptides have been produced as subunit vaccines, with configurations which corresponded to the protective antigen.
Analysis of immunologically competent cell surface molecules
MAbs can be used to map and study the various regions of an immunoglobulin molecule and the basis for immunoglobulin variability. For example, anti CD8 inhibits the killing by cytotoxic T cells. The anti-Ia (anti-La antibodies) molecule inhibits T-cell responses to macrophage processed antigen [38]. A cocktail of anti CD3+ complement kills T-cells in human bone marrow can be used to prevent graft versus host reaction [39].
Blood grouping
Anti-blood group monoclonal provide a more reliable standard reagent than the use of conventional antisera.
HLA typing
MAbs provide a reliable means of HLA antigen detection using individual specificities to the A, B, C and DR loci. HLA typing is specifically used prior to renal transplantation from the donor to the recipient.
Cancer diagnosis
Antibodies that can distinguish between malignant and normal cells have been generated. Malignant melanoma and acute lymphocytic leukemia cells are among the few that can be differentiated. Radioactive anti carcino-embryonic antigen is used to localize colonic tumors or secondaries on scanning. It may be possible to deliver cytotoxic drugs conjugated to mAbs right into tumor-specific cell types or the new “magic bullet” therapy.
In autoimmunity and immune deficiency
Imbalances in the ratio of T-helper and T suppressor subsets indicate immunodeficiency or autoimmunity. These states are accurately monitored by using mAbs against specific T-cell antigens. MAbs to the thyroid stimulating hormone and adrenocorticohormone receptors are used to study both graves’ disease and myasthenia gravis.
In the control of fertility
MAbs are also used against hormones and reproductive tract antigens such as human chorionic gonadotropin, luteinizing hormone and luteinizing hormone releasing hormone to control fertility.
Monoclonal mutants
Mutants lacking Fc structures are used for defining the biologic roles of Fc domains and for in-vivo neutralization of toxic drugs, for example in cases of digoxin overdose. Hybridoma technology has not only improved the quality and discriminating power of diagnostic and investigative serology but also promises to provide new reagents that will be useful in the diagnosis and treatment of many disease processes.
Cancer treatment
The treatment of cancer involves using mAbs that bind only to cancer cell-specific antigens and can induce immunological responses against the target cancer cells. Such mAb could also be modified for delivery of a toxin, radioisotope, cytokine or other active conjugate [38]. In addition, it is also possible to design bi-specific antibodies that can bind with their Fab regions both to target antigens and to a conjugate or effector cells. In fact, every intact antibody can bind to cell receptors or other proteins with its Fc region [39, 40]. Some examples of mAbs approved by the FDA include bevacizumab, cetuximab, panitumumab and trastuzumab [41].
Autoimmune diseases
MAbs used for autoimmune diseases include infliximab and adalimumab, which are effective in rheumatoid arthritis, Crohn’s disease and ulcerative Colitis due to their ability to bind to and inhibit TNF-
Conclusion
Due to their specificity and flexibility, mAbs present an attractive option for the development of new therapies and molecular drug targets against a wide variety of common diseases. Considerations when choosing the types of mAbs for development include its method of production, avidity, its effector function and its delivery to its target tissue (e.g. a smaller scFv may be able to penetrate a tumor more effectively than a full-sized antibody). However, despite some of its drawbacks, there is still major interest from pharmaceutical companies to develop mAbs for both clinical and diagnostic use, which will dictate the future of treatment and management of common, chronic conditions from both clinical and economical perspectives.
Footnotes
Conflict of interest
The authors declare conflict of interest as NIL.