TNF- -308G/A polymorphism has been investigated in few studies for an association with susceptibility to bullous pemphigoid (BP) and alopecia areata (AA). Yet, these findings had so far not been independently replicated, and no data on a possible association of TNF -308G/A polymorphism with these diseases in Iranian population were available.
OBJECTIVES:
In the present study, a possible effect of TNF- -308G/A variation on susceptibility to BP or AA disease was evaluated.
METHODS:
Genomic DNA was extracted from the blood of the patients with BP and AA as well as control subjects which genotyped for the TNF- -308 G/A polymorphism. TNF- gene expression levels were analyzed by real-time RT-PCR.
RESULTS:
No association was observed between the TNF- -308 G/A variation and susceptibility to BP or AA diseases in our Iranian cohort. In contrast to AA patients, expression of TNF- gene was significantly higher in BP patients compared to control group. TNF- gene was found to be similarly expressed in mutant and wild-type genotypes.
CONCLUSIONS:
TNF- -308G/A polymorphism is not associated with the risk to develop of BP and AA in our Iranian cohort. Furthermore, this polymorphism is contributed to altering the levels of gene expression in BP disease.
Bullous pemphigoid (BP) and alopecia areata (AA) are two organ-specific autoimmune diseases of the skin and hair follicle, respectively. BP is a difficult-to-treat autoimmune disease characterized by the presence of autoantibodies directed against collagen XVII and structural components of the skin which presents with blisters and erythema, frequently in conjunction with urticarial plaques [1]. The clinical presentation of AA is characterized by patches of non-scarring hair loss with a wide range of a single patch of hair loss on the scalp to complete loss of all body hair in severe cases [2]. Various pathogenic factors such as the release of cytokines are essential for induction of autoantibodies and clinical presentation of these diseases [3, 4, 5, 6, 7]. Tumor necrosis factor-alpha (TNF-), a multifunctional proinflammatory cytokine, was originally reported as a circulating factor which results in tumor necrosis but has since also been suggested as a key regulator of inflammatory responses [8]. Elevated serum and tissue levels of TNF- have been shown in many inflammatory conditions, including BP and AA [9, 10, 11, 12].
Cytokine gene polymorphisms, including TNF-, may influence the induction and release of cytokines, contribute to the disease-associated cytokine imbalance, and thereby affect the susceptibility to autoimmune diseases [13, 14]. While TNF- cytokine gene polymorphisms have been studied substantially in several autoimmune diseases, few studies have been performed in patients with AA [15, 16, 17] and only one study in BP [18]. Nevertheless, no results have been reported so far on the association between TNF- gene polymorphism and development of AA or BP in Iranian population. Since TNF- polymorphism might be associated with susceptibility to the diseases, the present study designed to examine the frequency of -308G/A TNF- polymorphism in Iranian BP and AA patients comparing with healthy individuals. Due to different gene expression of TNF- as a result of polymorphism, the RNA expression of TNF- was evaluated in the patients with different allelic variation and furthermore, compared with control subjects.
Materials and methods
Ethical approval
Local Ethics Committee (Human Research Ethics Committee of Skin Research Center, Shahid Beheshti University of Medical Sciences) considered and approved the study protocol and informed patient consent was obtained. The investigation conforms to the principles outlined in the 1964 Declaration of Helsinki.
Study design
This study enrolled 50 consecutive patients (20 patients with BP and 30 patients with AA) who admitted to Shohada Tajrish, Loghman Hakim, and Razi hospitals in Tehran in 2013–2017 (Table 1). All patients with lack of demographic data and inappropriate processing of initial laboratory specimens were excluded from the study. The initial data analysis of the patients was carried out for presentation and immediate peri-procedural assessment and diagnosis of BP and AA according to their investigational assessment guidelines [19, 20]. Several relevant information were obtained from all study participants such as suffering from autoimmune diseases and history of past BP or AA using respective questionnaire. We also studied 35 healthy unrelated volunteers as control subjects from the same population without any evidence of previous BP or AA. All samples collected by the Medical and Nursing staff of the Skin Research Center, Shohada Tajrish, Loghman Hakim, and Razi hospitals at Tehran, Iran.
Polymorphism analysis
All study participants provided blood for DNA preparation. Genomic DNA was isolated from peripheral blood cells using a genomic DNA isolation kit (DNG™ – Plus; SinaClon, Iran) according to the manufacturer’s protocol and amplified by polymerase chain reaction (PCR). Primers, as well as PCR and restriction digestion protocols, were used to identify TNF- -308G/A polymorphism described elsewhere [21, 22]. NcoI was the restriction enzyme used for digestion after PCR amplification determining the TNF- genotypes. The PCR products were separated by electrophoresis on 3% agarose gel.
Extraction of RNA and quantitative real-time RT-PCR
RNA was extracted from circulating leucocytes in blood samples of 50 patients and 35 control subjects using RNX-Plus kit (SinaClon, Iran) according to the manufacturer’s instructions followed by cDNA synthesis for qRT-PCR. TNF- RNA expression was assayed by real-time RT-PCR using SYBR Green q-PCR expression assays. TNF- gene expression was analyzed by primer sequences were designed by ABI PCR equipment (Applied Biosystems, USA): TNF-, forward: 5’-CCC ATG TTG TAG CAA ACC CT-3’, reverse: 5’-TGA GGT ACA GGC CCT CTG AT-3’; with annealing temperatures of 59C. The primer set for glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as housekeeping gene was obtained from previously reported sequences [21, 23].
Demographic and clinical characteristics in patients with BP and AA as well as control subjects. Statically significant differences were compared between groups using chi-square or t-test analysis
Characteristics
Frequency (%)
value
Patients with BP ( 20)
Patients with AA ( 30)
Controls ( 35)
BP vs. Control
AA vs. Control
Age (mean, years)
69.6 2.9
28.8 2.0
49.7 3.3
0.0001
0.0001
Gender, male/female
6/14 (30/70)
17/13 (56.7/43.3)
20/15 (57.1/42.9)
0.05
0.96
Age of onset
67.5 3.0
21.5 2.4
–
–
–
Disease duration (years)
20.2 6.2
5.22 0.8
–
–
–
Autoimmune diseases
6 (30)
1 (3.3)
4 (11.4)
0.08
0.22
Familial history of disease
1 (5)
6 (20)
1 (2.9)
0.68
0.02
Focal infection
6 (30)
1 (3.3)
11 (31.4)
0.91
0.004
Skin diseases
5 (25)
4 (13.3)
13 (37.1)
0.35
0.02
Stress
11 (55)
23 (76.7)
17 (48.6)
0.64
0.02
Depression
5 (25)
6 (20)
5 (14.3)
0.32
0.54
values were performed based on the chi-square or t-test and a value of 0.05 was considered statistically significant. Significant values are which shown in bold. BP, bullous pemphigoid; AA, alopecia areata; , number.
Allele frequencies and genotype distributions of TNF- -308G/A gene polymorphism in the study population. Logistic regression analysis was used to compare statically significant differences between groups
TNF-
Allele/genotype
Frequency (%)
value
Patients with BP
Patients with AA
Controls
BP vs. Control
AA vs. Control
( 20)
( 30)
( 35)
G-308A (rs1800629)
Genotype
G/G
17 (85)
21 (70)
29 (82.9)
0.56
0.26
G/A
3 (15)
6 (20)
4 (11.4)
A/A
0
3 (10)
2 (5.7)
Total
20 (100)
30 (100)
35 (100)
Allele
G
37 (92.5)
48 (80)
62 (88.6)
0.51
0.18
A
3 (7.5)
12 (20)
8 (11.4)
values were performed based on the logistic regression test and a value of 0.05 was considered statistically significant. BP, bullous pemphigoid; AA, alopecia areata; , number.
Statistical analysis
Statistical analysis of the data was carried out by SPSS statistical software program, version 23. The Chi-square () test was used for analyzing the differences in genotype distribution, allele frequencies, and consistency with Hardy-Weinberg equilibrium. test, analysis of variance (ANOVA), or t-test was used for analyzing the relationships between polymorphism and the clinical and demographic features. All data were expressed as mean SEM. Logistic regression analysis was performed to eliminate confounding influences. TNF-/GAPDH RNA expression are presented as a ratio of the patients to that of controls which compared based on the Mann-Whitney U test. A value less than 0.05 was considered statistically significant and corrected for the number of comparisons using Bonferroni method.
Results
Demographic data and clinical characteristics of the study population
In the present study, 85 subjects were analyzed to determine whether TNF- gene variation is contributed with the risk of BP or AA in Iranian patients comparing with healthy individuals. Demographic data and clinical characteristics of the patients and controls are presented in Table 1. According to our analysis, except age which was significantly different between patients and controls, significant difference was found in some risk factors including familial history of disease, infection, other skin disease, and stress between AA patients and control individuals. While the distribution of the -308G/A in BP patients ( 0.13, 0.07) was within the Hardy-Weinberg equilibrium, AA patients ( 4.21, 0.03) and control individuals ( 6.63, 0.01) deviated from this equilibrium.
Demographic data and clinical characteristics in BP and AA patients and control subjects as well as patients with polymorphic and wild genotypes in TNF- -308G/A gene polymorphism. Statically significant differences were compared between groups using chi-square or t-test analysis
Characteristics
Patients with BP Mean/ (%)
Patients with AA Mean/ (%)
G/G 17
G/A A/A 3
G/G 21
G/A A/A 9
Age (mean, years)
72.4 2.9
53.6 4.8
0.02
26.3 2.4
34.5 3.3
0.07
Gender, male/female
4/13 (23.5/76.5)
2/1 (66.7/33.3)
0.13
10/11 (47.6/52.4)
7/2 (77.8/22.2)
0.12
Age of onset
70.2 2.9
51.6.8 5.1
0.02
19.9 2.7
25.1 4.8
0.34
Disease duration (years)
19.5 7.1
24.0 12
0.80
5.0 1.0
5.6 1.7
0.76
Autoimmune diseases
5 (29.4)
1 (33.3)
0.89
1 (4.8)
0
0.50
Familial history of disease
1 (5.9)
0
0.66
5 (23.8)
1 (11.1)
0.42
Focal infection
4 (23.5)
2 (66.7)
0.13
1 (4.8)
0
0.50
Skin Diseases
4 (23.5)
1 (33.3)
0.71
3 (14.3)
1 (11.1)
0.81
Stress
9 (52.9)
2 (66.7)
0.66
19 (90.5)
4 (44.4)
0.006
Depression
3 (17.6)
2 (66.7)
0.07
6 (28.6)
0
0.07
values () were performed based on the chi-square or t-test and a value of 0.05 was considered statistically significant. BP, bullous pemphigoid; AA, alopecia areata; , number.
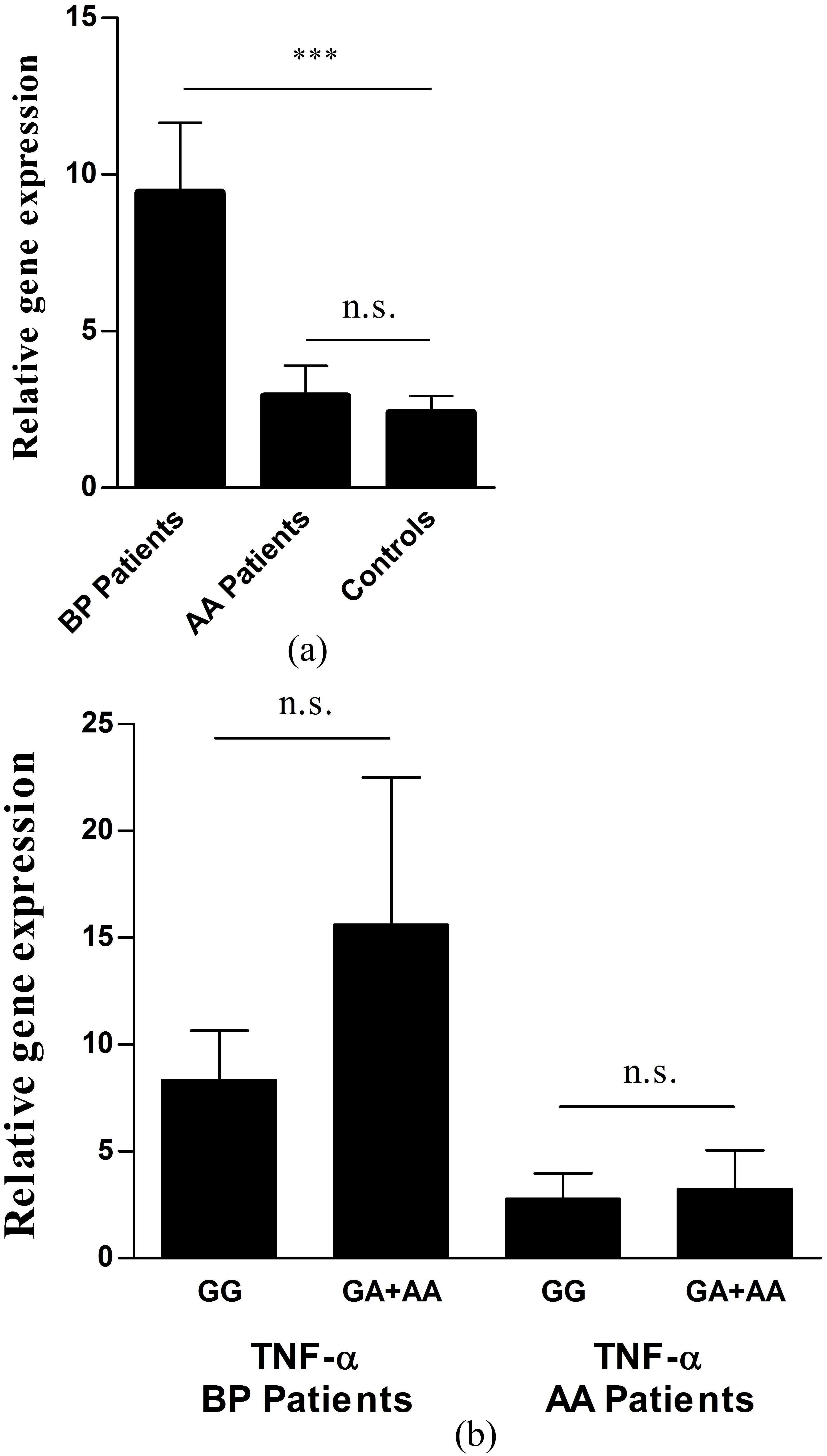
TNF- RNA expression of the patients with BP or AA and control subjects. Figures represent a comparison of gene expression between patients and controls (a) or between wild and polymorphic genotypes in the patient group (b), expressed as the percentage of GAPDH gene expression of patients relative to control subjects. RNA expression levels of both groups are presented as mean SEM and were compared based on the Mann-Whitney U test. ***: 0.0001, n.s.: non-significant. TNF- -308G/A genotypes: wild: G/G, polymorphic: G/A A/A. RNA expression levels are presented as mean SEM and were compared based on the Mann-Whitney U test which remains non-significant.
No association between TNF- -308G/A polymorphism and BP or AA disease in an Iranian cohort
To verify a possible relationship between disease development and -308G/A polymorphism of TNF-, frequencies of alleles were investigated which are summarized in Table 2. The ‘A’ allele frequency was similar in the patients with BP and control subjects (7.5% vs. 11.4% respectively, 0.5). Logistic regression analysis revealed that the minor allele ‘A’ at this locus of TNF- might not be an independent risk factor for developing BP; the calculated odds ratio (OR) was 0.62 (95% confidence interval (CI): 0.20–2.40). Although the frequency of allele ‘A’ is higher in patients with AA compared to healthy individuals (20% vs. 11.4% respectively), this difference does not achieve the levels of significance (OR 1.93, 95% CI: 0.73–5.11, 0.18).
Increased gene expression of TNF- in BP patients, but not in patients with AA
To investigate whether BP and AA diseases influence gene expression, a quantitative analysis of the TNF- gene was performed which is shown in Fig. 1a. The RNA expression levels (TNF-/GAPDH) showed a significant elevation in circulating leukocytes obtained from patients with BP compared with control subjects (9.43 2.22 vs. 2.39 0.54, 0.0003). In contrast, gene expression of TNF- was similar in patients with AA compared with control subjects (2.92 0.97 vs. 2.39 0.54, 0.73). Further investigation in BP patients revealed a higher TNF- gene expression in mutant genotypes (GA AA) to that of wild one (GG) in the patient group (15.62 6.88 vs. 8.33 2.31). However, this difference did not reach significance level ( 0.2). TNF- gene expression was similar in mutant and wild-type genotypes, respectively (3.23 1.80 vs. 2.79 1.18, 0.9). Therefore in contrast to AA disease, this polymorphism might be contributed to altering the levels of gene expression in BP disease (Fig. 1b).
Association of demographic data and clinical characteristics with genotypes
Further analysis was performed to investigate any association between clinical and demographical features and TNF- genotypes of patients which are shown in Table 3. According to our analysis, while there was significant difference in age and age of disease onset between the BP patients and controls, stress was significantly prevalent in patients with AA comparing to the controls.
Discussion
Bullous Pemphigoid (BP) is a rare autoimmune skin disease characterized by autoantibodies against structural components of the dermal-epidermal junction (BP180 and BP230) which cause blisters and erosions on skin [1]. These components of basement membrane zone are similarly expressed in the anagen hair follicles of human scalp [24, 25]. Although the role of cytokines has been shown in the pathogenesis of BP and alopecia areata (AA) [3, 4, 5, 6, 7], there are controversies about the major cytokine profile in these diseases. Various significant alleles have been proposed in several studies due to the different ethnic background of populations. Herein, beside HLA genes which are obviously associated with autoimmune diseases, TNF- is one of the most studied genes in their pathogenesis. Despite positive associations, no specific gene variant has yet been identified as a cause of Bullous pemphigoid (BP) or alopecia areata (AA), and associated alleles should be identified in each particular population. In the present study, no association was found neither between the presence of the -308G/A polymorphism in the promoter region of the TNF- gene and BP patients, nor AA patients in Iranian population.
TNF- gene, due to encoding one of the most potent proinflammatory cytokines and the autoimmune modulator, is considered as a significant candidate determining genetic susceptibility to the development autoimmune diseases. This gene is located in HLA class III (6p21) which is a highly polymorphic region [26]. The location of TNF-, as well as it’s biological activities, make it a good candidate in which polymorphisms within this region influence the pathogenesis of several autoimmune diseases. In contrast to other TNF- gene polymorphisms with little or no association, a single nucleotide substitution at -308 nucleotides in the TNF- promoter is contributed to transcription elevation of the gene, higher plasma TNF- levels, and disease susceptibilities [27, 28]. Nevertheless, contradictory findings have so far been reported. In a previous study, it has been shown that the plasma levels of TNF- are significantly higher in patients with acute myocardial infarction compared with healthy individuals [21]. In addition, these results showed a significantly high expression of TNF- mRNAs and proteins in the patients with ‘A’ allele comparing with ‘G’ allele in TNF- gene variation which tends to be related to increased transcription of TNF- gene [21]. Although BP and AA share the common features with autoimmune diseases [29], the contribution of TNF- -308G/A polymorphism in the disease process, in particular, its effect on transcription levels remains largely unclear.
Although previous findings have been shown an association between TNF- -308G/A polymorphism and AA [15], other report failed to reach significance when corrected for multiple contrasts [16]. To our knowledge in the case of BP, there is lacking data regarding the investigation of cytokine gene polymorphisms in BP patients and it has yet been conducted only in one study in a Chinese population [18]. To date, there is no available report investigating TNF- -308G/A variant in Iranian ethnicity, neither in AA nor in BP. In this study, frequencies were found to be similar for either genotypes or alleles in patients and controls which suggest no association of this gene variant with susceptibility to these autoimmune diseases. This polymorphism at position nucleotide -308G/A in the promoter region affect the expression of TNF- gene [27]. Herein, our findings showed discrepant results concerning TNF- gene expression in BP and AA diseases. While there was a significant difference in gene expression between patients and control individuals in BP disease, our data did not achieve statistical significance in expression levels of TNF- in patients with AA compared to the control subjects. On the other hand, our results confirmed that the TNF- gene has similar activity in the patients with ‘A’ allele comparing with ‘G’ allele in both diseases. Indeed, the frequencies of ‘A’ allele in TNF- -308G/A polymorphism differ from 4% in the Mexican population [15] to 24% in Australians [30]. Based on our results, the ‘A’ allele frequency in TNF- -308G/A polymorphism in BP and AA patients are 7.5 and 20%, respectively. This frequencies are in agreement with our previous study [21] as well as other Iranian reports [31]. Nevertheless, Iranian population is one of the most heterogeneous populations in the world [32] and case-control studies in the Iranian Kurdish or Turkish ethnic groups indicate an ‘A’ allele frequencies of 8 and 9.5%, respectively [33, 34]. These controversies may be due to different factors such as multifactorial nature of different types of diseases, variations in designing different studies, and genetic heterogeneity within and between the studied populations. In addition to this, activation and presence of other molecules that interact with the TNF- promotor region can also take into account. Of note, genetic polymorphism investigations have shown a wide difference in allele frequencies in the various ethnic groups [35, 36]. Herein, the difference of risk allele frequency between populations may explain the variations in disease prevalence among those populations [37]. Natural selection and certain environmental conditions can also modulate the balance in allele frequencies across populations [38].
In Conclusion, a common gene polymorphism in the TNF- locus was investigated as a risk factor for the development of two autoimmune diseases. Our findings suggest that polymorphism in the TNF-promoter might not be contributed to the susceptibility of BP and AA. Although this polymorphism has an effect on promoter hyperactivity and in turn increased TNF- transcription in BP patients, this effect was not seen in AA patients. To our knowledge, this is the first study evaluating these factors in Iranian patients with BP and AA. Given the presence of various ethnic groups in Iran, screening of several populations from different regions and ethnicities especially with larger sample size could help to validate these results and draw any representative picture of Iranian population. In the present study, we did not investigate the relationship between polymorphism and TNF- secretion. Future studies may identify this association.
Footnotes
Acknowledgments
We would like to thank Medical and Nursing staff of the Skin Research Center, Shohada Tajrish, Loghman Hakim, and Razi Hospitals at Tehran, Iran for helpful collaboration.
References
1.
SchmidtE. and ZillikensD., Pemphigoid diseases, Lancet381 (2013), 320–332.
2.
AlkhalifahA.AlsantaliA.WangE.McElweeK.J. and ShapiroJ., Alopecia areata update: Part I. Clinical picture, histopathology, and pathogenesis, J Am Acad Dermatol62 (2010), 177–188, quiz 189–190.
3.
AmeglioF.D’AuriaL.BonifatiC.FerraroC.MastroianniA. and GiacaloneB., Cytokine pattern in blister fluid and serum of patients with bullous pemphigoid: Relationships with disease intensity, Br J Dermatol138 (1998), 611–614.
4.
RicoM.J.BenningC.WeingartE.S.StreileinR.D. and HallR.P., Characterization of skin cytokines in bullous pemphigoid and pemphigus vulgaris, Br J Dermatol140 (1999), 1079–1086.
5.
RhodesL.E.HashimI.A.McLaughlinP.J. and FriedmannP.S., Blister fluid cytokines in cutaneous inflammatory bullous disorders, Acta Derm Venereol79 (1999), 288–290.
6.
BilgicO.SivrikayaA.UnluA. and AltinyazarH.C., Serum cytokine and chemokine profiles in patients with alopecia areata, J Dermatol Treat27 (2016), 260–263.
7.
Suárez-FariñasM. et al., Alopecia areata profiling shows TH1, TH2, and IL-23 cytokine activation without parallel TH17/TH22 skewing, J Allergy Clin Immunol136 (2015), 1277–1287.
8.
CarswellE.A.OldL.J.KasselR.L.GreenS.FioreN. and WilliamsonB., An endotoxin-induced serum factor that causes necrosis of tumors, Proc Natl Acad Sci USA72 (1975), 3666–3670.
9.
AvdagićN. et al., Tumor necrosis factor-alpha serum level in assessment of disease activity in inflammatory bowel diseases, Med Glas (Zenica)10 (2013), 211–216.
10.
HagelA.F. et al., Plasma histamine and tumour necrosis factor-alpha levels in Crohn’s disease and ulcerative colitis at various stages of disease, J Physiol Pharmacol66 (2015), 549–556.
11.
D’AuriaL.MussiA.BonifatiC.MastroianniA.GiacaloneB. and AmeglioF., Increased serum IL-6, TNF-alpha and IL-10 levels in patients with bullous pemphigoid: Relationships with disease activity, J Eur Acad Dermatol Venereol12 (1999), 11–15.
12.
Kasumagic-HalilovicE.ProhicA. and CavaljugaS., Tumor necrosis factor-alpha in patients with alopecia areata, Indian J Dermatol56 (2011), 494–496.
13.
TrajkovD.Mishevska-PerchinkovaS.Karadzova-StojanoskaA.PetlichkovskiA.StrezovaA. and SpiroskiM., Association of 22 cytokine gene polymorphisms with rheumatoid arthritis in population of ethnic Macedonians, Clin Rheumatol28 (2009), 1291–1300.
14.
DurãesC. et al., Polymorphisms in the TNFA and IL6 genes represent risk factors for autoimmune thyroid disease, PloS One9 (2014), e105492.
15.
CristinaC.-S. et al., Tumor necrosis factor alpha promoter-308G/A polymorphism in Mexican patients with patchy alopecia areata, Int J Dermatol51 (2012), 571–575.
16.
GalbraithG.M. and PandeyJ.P., Tumor necrosis factor alpha (TNF-alpha) gene polymorphism in alopecia areata, Hum Genet96 (1995), 433–436.
17.
SayedM.H.E.El-HefnawyA.-H.M.Al-MashaikyF.S. and SayedS.B.E., Tumor necrosis factor α promoter -308G/A polymorphism in patients with patchy alopecia areata, Egypt J Dermatol Venerol34 (2014), 36–40.
18.
ChangY.T. et al., Cytokine gene polymorphisms in bullous pemphigoid in a Chinese population, Br J Dermatol154 (2006), 79–84.
19.
FelicianiC. et al., Management of bullous pemphigoid: The European Dermatology Forum consensus in collaboration with the European Academy of Dermatology and Venereology, Br J Dermatol172 (2015), 867–877.
20.
OlsenE.A. et al., Alopecia areata investigational assessment guidelines – Part II. National Alopecia Areata Foundation, J Am Acad Dermatol51 (2004), 440–447.
21.
GhaderianS.M.H.Akbarzadeh NajarR. and Tabatabaei PanahA.S., Tumor necrosis factor-α: Investigation of gene polymorphism and regulation of TACE-TNF-α system in patients with acute myocardial infarction, Mol Biol Rep38 (2011), 4971–4977.
22.
WarzochaK. et al., Genetic polymorphisms in the tumor necrosis factor locus influence non-Hodgkin’s lymphoma outcome, Blood91 (1998), 3574–3581.
23.
AkatsuT.NakamuraM.SatohM. and HiramoriK., Increased mRNA expression of tumour necrosis factor-alpha and its converting enzyme in circulating leucocytes of patients with acute myocardial infarction, Clin Sci (Lond)105 (2003), 39–44.
24.
ChuangY.H.DeanD.AllenJ.DawberR. and WojnarowskaF., Comparison between the expression of basement membrane zone antigens of human interfollicular epidermis and anagen hair follicle using indirect immunofluorescence, Br J Dermatol149 (2003), 274–281.
25.
MitevaM.MurrellD.F. and TostiA., Hair loss in autoimmune cutaneous bullous disorders, Dermatol Clin29 (2011), 503–509.
26.
WilsonA.G.SymonsJ.A.McDowellT.L.McDevittH.O. and DuffG.W., Effects of a polymorphism in the human tumor necrosis factor alpha promoter on transcriptional activation, Proc Natl Acad Sci USA94 (1997), 3195–3199.
27.
ElahiM.M.AsotraK.MatataB.M. and MastanaS.S., Tumor necrosis factor alpha -308 gene locus promoter polymorphism: An analysis of association with health and disease, Biochim Biophys Acta1792 (2009), 163–172.
28.
El-TahanR.R.GhoneimA.M. and El-MashadN., TNF-α gene polymorphisms and expression, SpringerPlus5 (2016), 1508.
29.
WengrafD.A. et al., Genetic analysis of autoimmune regulator haplotypes in alopecia areata, Tissue Antigens71 (2008), 206–212.
30.
DalzielB.GosbyA.K.RichmanR.M.BrysonJ.M. and CatersonI.D., Association of the TNF-alpha -308G/A promoter polymorphism with insulin resistance in obesity, Obes Res10 (2002), 401–407.
31.
MaddahM. et al., Association of tumour necrosis factor-alpha G/A -238 and G/A -308 single nucleotide polymorphisms with juvenile idiopathic arthritis, Int J Immunogenet43 (2016), 391–396.
32.
RafieeL.SaadatI. and SaadatM., Glutathione S-transferase genetic polymorphisms (GSTM1, GSTT1 and GSTO2) in three Iranian populations, Mol Biol Rep37 (2010), 155–158.
33.
GolshaniH.HaghaniK.DoustiM. and BakhtiyariS., Association of TNF-α 308G/A polymorphism with type 2 diabetes: A case-control study in the Iranian Kurdish Ethnic Group, Osong Public Health Res Perspect6 (2015), 94–99.
34.
BonyadiM.AbdolmohammadiR.JahanafroozZ.SomyM.-H. and KhoshbatenM., TNF-alpha gene polymorphisms in Iranian Azari Turkish patients with inflammatory bowel diseases, Saudi J Gastroenterol20 (2014), 108–112.
35.
Race, Ethnicity, and Genetics Working Group, The use of racial, ethnic, and ancestral categories in human genetics research, Am J Hum Genet77 (2005), 519–532.
36.
IoannidisJ.P.A.NtzaniE.E. and TrikalinosT.A., ‘Racial’ differences in genetic effects for complex diseases, Nat Genet36 (2004), 1312–1318.
37.
MylesS.DavisonD.BarrettJ.StonekingM. and TimpsonN., Worldwide population differentiation at disease-associated SNPs, BMC Med Genomics1 (2008), 22.
38.
MatteiJ. et al., Disparities in allele frequencies and population differentiation for 101 disease-associated single nucleotide polymorphisms between Puerto Ricans and non-Hispanic whites, BMC Genet10 (2009), 45.