
Abstract
BACKGROUND:
Pneumococcal infections are a leading global cause of morbidity and mortality, complicated by the increasing antimicrobial resistance of pneumococcal isolates.
OBJECTIVE:
To evaluate morbidity and mortality associated with both invasive pneumococcal disease (IPD) and non-IPD in Jamaica in both the paediatric and adult population. Pneumococcal isolates (
METHODS:
Risk factors for poor clinical outcomes: death, complicated disease and length of hospitalization (LOH) were evaluated and antimicrobial resistance patterns were determined by Kirby-Bauer disc diffusion.
RESULTS:
The case fatality rate was 6.8%. Independent mortality risk factors included complicated disease [OR 30.9 (3.4–276.6)] and diabetes mellitus [OR 8.3 (1.4–48.8)]. Independent risk factors for the development of complicated disease included sickle cell disease [OR 36.5 (4.2–320.3)] and sepsis [OR 3.5 (1.2–10.4)]. The LOH was increased most in patients with invasive disease (4.6-fold) and resistance to ceftriaxone (4.3-fold). Penicillin (16.0%) and erythromycin (14.9%) resistance was most prevalent, while ceftriaxone (4.3%) resistance was least prevalent.
CONCLUSIONS:
The high burden of IPD in at-risk groups in our population and the associated increase in morbidity and mortality underlie the need for improved preventive and therapeutic management strategies in these patients.
Introduction
Streptococcus pneumoniae is the most common cause of acute otitis media, sinusitis, pneumonia and one of the most important causes of bacterial meningitis worldwide [10, 15]. The overall global morbidity and mortality of invasive disease caused by this pathogen, particularly pneumonia and meningitis, have remained high despite the availability of effective antimicrobial therapy [8]. The case fatality rates for pneumococcal pneumonia in particular, which ranges from 7 to 36%, has remained largely unchanged for the last 50 years [5]. Management of these infections are further complicated by the increasing resistance of the isolates to antibiotics often used in management of these patients [3].
The pathogenesis of pneumococcal disease is the result of a delicately balanced series of complex and as yet incompletely understood interactions between host and bacteria [12]. Pneumococcal colonization, which is most prevalent in the paediatric population, serves as a reservoir for disease through translocation into sterile sites like the bloodstream and meninges or inter-person droplet transmission [12]. An increased risk of invasive pneumococcal disease (IPD) development is associated with defects in the non-specific or specific immune defense mechanisms against colonization, aspiration or invasion of S. pneumoniae [12, 15]. Such underlying conditions that affect immune function include HIV infection, congenital or acquired asplenia and concurrent respiratory infections with influenza virus, Haemophilus influenzae and Mycoplasma pneumoniae. In studies of IPD worldwide, predisposing conditions can be found in approximately 22% to 43% of patients [9].
There is an urgent need for accurate data on the morbidity and mortality associated with both IPD and non-IPD in Jamaica in both the paediatric and adult population. The results of this study will serve to guide the implementation of appropriate preventive and therapeutic management strategies for various groups at risk for developing pneumococcal disease in Jamaica.
Patients/methods
Subjects and bacterial strains
The study was carried out between 2008 and 2009, recruiting patients presenting at the University Hospital of the West Indies (UHWI), the major tertiary referral center in Kingston and St. Andrew in the eastern region of the island. The pneumococcal isolates (
Demographic and clinical data
A standardized data abstraction form was used to collect demographic and clinical information from hospital clinical records. The data collected pertained to age, gender, type of clinical specimen and date of collection, clinical presentation, morbidity, mortality and the presence of any co-morbid illnesses that increase risk for pneumococcal disease. Invasive disease was defined as cases in which pneumococci was isolated from a normally sterile body site such as the blood stream, central nervous system or synovial fluid [17]. The primary clinical outcome measure was death from any cause and secondary outcomes included development of complications and the length of hospitalization (LOH). The development of complications was defined as the need for intensive cardiovascular or respiratory resuscitation measures. The LOH was calculated in days from initial clinical assessment to discharge from the hospital and the LOH for decedents was not included in association analyses including this variable.
Microbiology laboratory procedures
Standard microbiological procedures were followed and bacterial isolates were identified as S. pneumoniae by microscopy, colony morphology, positive optochin sensitivity and bile solubility tests [18]. The sensitivity of pneumococcal isolates to penicillin (P), ampicillin (AMP), amoxicillin-clavulanate (AMC), ceftriazone (CRO), trimethoprim-sulfamethoxazole (SXT) and erythromycin (E) was determined by the Kirby-Bauer disc diffusion method. A control pneumococcal strain (ATCC49619) was utilized during microbiological testing of samples. The pneumococcal strains were stored in tryptic soy broth containing 15% glycerol at
Clinical characteristics of patients presenting with pneumococcal disease
Clinical characteristics of patients presenting with pneumococcal disease
COPD – chronic obstructive pulmonary disease, DM – diabetes mellitus, HIV – human immunodeficiency virus, NB – newborn, SCD – sickle cell disease, URTI – upper respiratory tract infections. *Age data was not available for 2 individuals.
Clinical presentation of pneumococcal infections among various age groups. CNS – meningitis and intracerebral abscess cases, Ear – otitis cases, Eye – conjunctivitis and/or periorbital cellulitis cases, LRTI – pneumonia cases, SSI – skin and skin structure infections, URTI – upper respiratory tract infections. The 2 cases in which age data were not available were necessarily excluded from this analysis.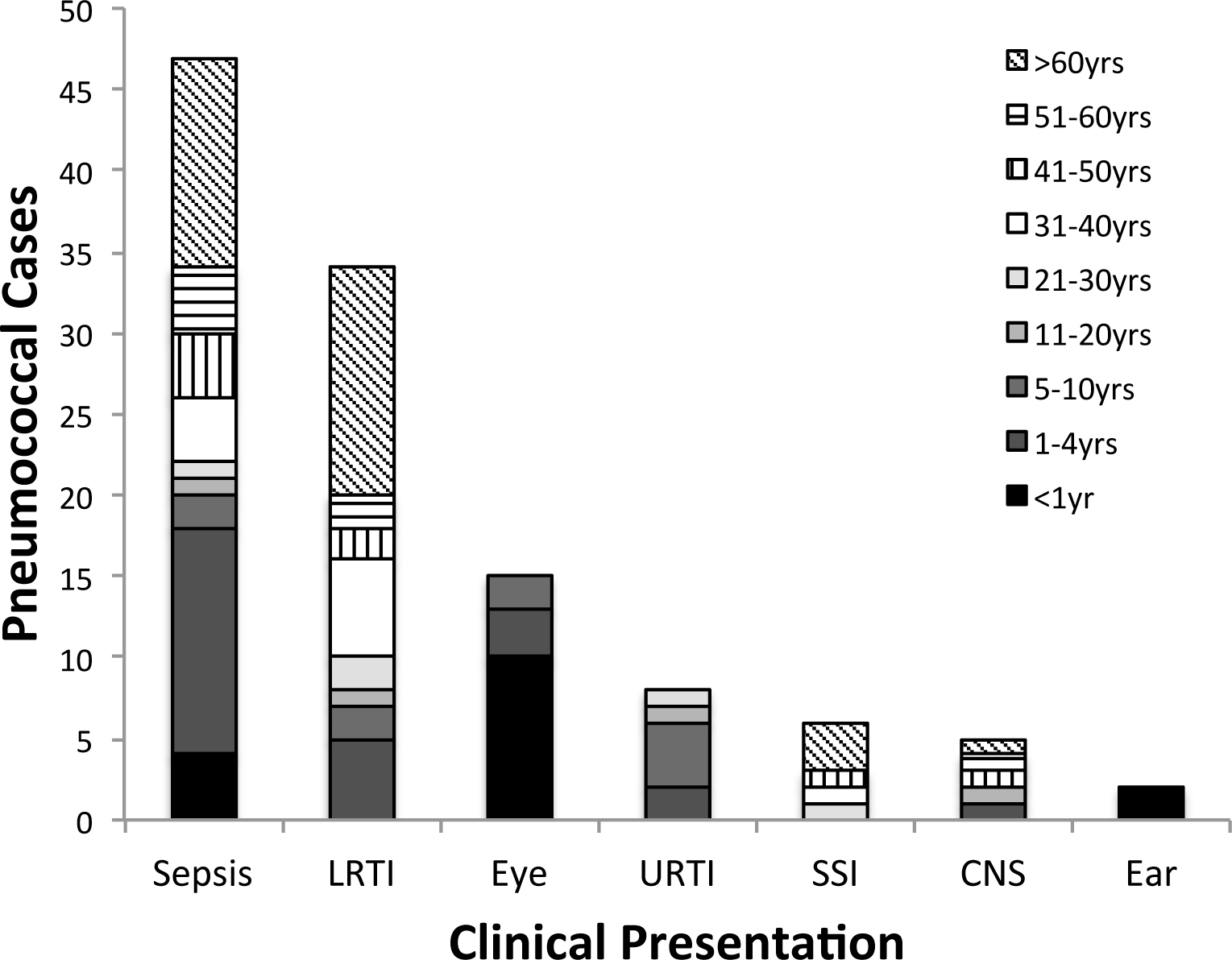
Continuous data variables were expressed as mean
Results
Clinical presentations
Sepsis with or without a known primary focus of infection (52.1%), pneumonia (38.2%) and conjunctivitis (16.0%) accounted for the majority of clinical presentations (Table 1). The majority of these sepsis cases occurred in children younger than 5 years (38.3%) and adults greater than 60 years (27.7%) (Fig. 1). Almost half of sepsis cases occurred without an identified primary infective focus (22/49, 44.9%). In descending order, bacteremia was most prevalent in cases of CNS infections (60.0%), pneumonia (58.3%) and skin and skin structure infections (SSI) (33.3%) but absent in other patients. Most otitis (100%) and conjunctivitis cases (86.7%) occurred in children below 5 years, all in children below 18 years. In contrast, CNS (60.0%), pneumococcal pneumonia (76.4%) and SSI (100%) cases occurred most frequently in adults over 18 years.
Risk factors for pneumococcal disease were present in 34.0% (32/94) cases. These included human immunodeficiency virus infection or acquired immune deficiency syndrome (HIV/AIDS) (7/94, 7.4%), sickle cell disease (SCD) (7/94, 7.4%), diabetes mellitus (DM) (7/94, 7.4%), solid tumors (4/94, 4.3%), hematological malignancy (2/94, 2.1%), chronic obstructive pulmonary disease (2/94, 2.1%), malnutrition (1/94, 1.1%), viral pneumonia (1/94, 1.1%) and extensive burns (1/94, 1.1%). Most of the cases of HIV and DM occurred in the adult population while SCD was present in both the paediatric and adult populations.
Clinical summary of the fatal cases of pneumococcal disease in the UHWI cohort
Clinical summary of the fatal cases of pneumococcal disease in the UHWI cohort
AIDS: Acquired immunodeficiency disease, ARDS: Acute respiratory distress syndrome, HIV: Human immunodeficiency virus, LOH: Length of hospitalization from intake interview to demise, MI: Myocardial infarction.
Risk factors associated with clinical outcome measures
* Note that this translates to a roughly 8-fold decrease in LOH. AMC: Amoxicillin-clavulanate, AMP: Ampicillin, CNS: Central nervous system, CRO: Ceftriaxone, DM: Diabetes mellitus, LOH: Length of hospitalization, OR (95% CI): Odds ratio (95% confidence interval), SCD: Sickle cell disease.
In decreasing order, isolates were most resistant to penicillin (15/94, 16.0%), erythromycin (14.9%), trimethroprim/sulfamethoxazole (9.6%), ampicillin(5.3%), amoxicillin/clavulanate (4.3%) and ceftriaxone (4.3%).
A total of 6 patients died during the course of their illness giving a case fatality rate of 6.8% (6/94). The majority of these deaths (3/6, 50.0%) occurred during the first day; the remaining 3 patients dying on days 16, 17 and 31 of their illness. All but one of these patients was middle aged or elderly, the last being a child of 8 months. A clinical summary of these cases is provided in Table 2. Significant risk factors for death included complicated disease (OR 30.9, 95% CI 3.4–276.6,
Complicated disease occurred in 21 patients(22.3%). The development of complications was significantly associated with the presence of SCD (OR 36.5, 95% CI 4.2–320.3,
Mean LOH was 9.1 days (range 0–56) and was significantly increased 2 to 3-fold in patients with complicated disease, sepsis, CNS infections and isolates resistant to ampicillin or amoxicillin-clavulanate. Patients with invasive disease or isolates resistant to ceftriaxone had an over 4-fold increase in their mean LOH (Table 3). Multivariate linear regression identified ceftriaxone resistance (
Discussion
In our study we describe for the first time the morbidity and mortality of pneumococcal disease that is broadly representative of all age groups of the Jamaican population. The study population also comprised both hospitalized patients, who tend to have more severe disease, and outpatients, whose pneumococcal infection did not require hospitalization. A substantial portion of patients were within the paediatric age group (
Our study highlights the unique challenges of pneumococcal disease management in children and adults in Jamaica and the region. Several risk factors for pneumococcal disease were present in a substantial proportion of our patients and several of these conditions pose serious public heath concerns. HIV/AIDS, for example, is a growing problem in the Caribbean, which is the second most affected area worldwide after Sub-Saharan Africa [7]. The most urbanized parishes in Jamaica report the highest prevalence of HIV cases
The prevalence of DM in the Jamaican population has been estimated at 8% and is of great concern for the adult population given the independent risk for mortality associated with DM in our pneumococcal disease cohort [14, 15].
Paediatric IPD in Jamaican SCD patients has been estimated at 480/100,000 individuals [6]. These rates are much lower than those reported in SCD patients in other developing countries with rates as high as 6900/ 100,000 [19]. Our relatively low rates are due in large part to the success of the Jamaican newborn screening program for SCD begun in 1995, which automatically enrolls SCD children in the Sickle Cell Unit (SCU). The SCU provides free ambulatory health care for these patients and the administration of monthly penicillin prophylaxis up to age 4 years and polysaccharide vaccine (PPV23) administration thereafter [6].
We report that SCD was most strongly associated with the development of complicated pneumococcal disease in this cohort of Jamaican patients, which in turn increases the risk for mortality. It is important to point out however that SCD itself was not associated with mortality in our study population. These factors underscore the need for PCV implementation in this patient population [1, 14].
Antibiotic resistance rates reported in our study are similar to previous estimates and indicate a relatively high resistance to beta-lactams and macrolides, a worrying global trend [16]. While the prevalence of resistance to ceftriaxone, ampicillin and amoxicillin-clavulanate was relatively low in our population, patients with isolates that were resistant to these agents had increased morbidity as measured by length of hospitalization. This did not, however, translate into an increased risk for the development of complicated disease or mortality. Detailed population studies are necessary to evaluate molecular determinants of resistance, transformation and competence in the evolution of S. pneumoniae infections across the country.
Our study is limited by the relatively small number of pneumococcal cases for review, however, we were able to show a strong association between complicated disease and SCD patients, which indicates that routine childhood pneumococcal vaccination in Jamaica may be beneficial. Studies investigating the island-wide prevalence of pneumococcal nasopharyngeal colonization in Jamaica, particularly in children, are urgently needed to clarify this point. In contrast, targeted use of vaccines in elderly patients with conditions such as DM, HIV infection or chronic respiratory diseases, which increase the risk of complicated pneumococcal disease, may be more ideal than routine administration given reported herd-protection effects [4]. Our findings will inform future efforts to improve the management of patients with pneumococcal infections and guide vaccine implementation strategies in Jamaica and the region.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Microbiology Department at the University Hospital of the West Indies for their generous assistance in facilitating collection and processing of pneumococcal isolates at the institution. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest.