
Abstract
BACKGROUND:
Hepatitis B virus infection is a global public health problem. The virus has infected more than one-third of the global population. It has been estimated that 360 million chronic carriers are living around the world with a high risk for developing cirrhosis, hepatic carcinoma and hepatic failure.
OBJECTIVE:
The aim of this study was to determine the prevalence of some hepatitis B markers among pregnant women attending antenatal clinic in Sokoto Specialist Hospital, Nigeria.
METHODS:
The hepatitis testing was carried out using the Skytec-Rapid Diagnostic HBV-5 rapid kit (Skytec-Rapid Diagnostic, USA). The kit is based on lateral flow chromatographic immunoassay for the qualitative detection of HBsAg, HBsAb, HBeAg, HBeAb, and HBcAb in human serum or plasma. Panel format can conveniently test for five targets at once and utilizes all markers to help distinguish between acute and chronic infections.
RESULTS:
Out of 117 pregnant women tested, 15 were positive for HBsAg (12.8%), 6 positive for HBsAb (5.1%), 1 for HBeAg (0.9%), 14 tested positive for HBeAb (12.0%), and 14 tested for HBcAb (12.0%). The prevalence of HBsAg, HBsAb, HBeAg, HBcAb and HBcAb was compared based on ethnicity. HBsAb was significantly higher among the Hausa ethnic group (
CONCLUSION:
The study observed a high prevalence of various hepatitis B viral markers among pregnant women attending antenatal care in Specialist Hospital Sokoto. There is need for routine screening of all pregnant women and infants born to hepatitis B positive mothers. Government and non-governmental organizations should intensify efforts to enlighten the general population on the public health importance of the disease and the importance of hepatitis screening. There is also need for the development of a treatment protocol for the management of pregnant women positive for hepatitis B to prevent mother to child transmission. There is an urgent need for the implementation of evidenced-based best practice of providing universal vaccination against hepatitis B for all hepatitis B negative women of child bearing age in particular and all Nigerians in general.
Introduction
Hepatitis B infection can be transmitted both vertically and horizontally. Although the universal neonatal vaccination and catch up vaccination of teenagers along with targeted vaccination of at-risk population have decreased the prevalence of HBV infection in the West dramatically [1]. Hepatitis B virus has infected more than one-third of the global population. It has been estimated that 360 million chronic carriers are living around the world with a high risk for developing cirrhosis, hepatic carcinoma and hepatic failure [2]. Hepatitis B can be transmitted vertically from mother to foetus or neonate during pregnancy, labour or breast feeding or horizontally via sexual relationship and unsafe blood transfusion, nosocomial transmission, transplantation and tattooing [3, 4].
Vertical transmission is responsible for 35%–40% of the HBV incident cases worldwide [5]. Most of the infected persons have acquired the infection during perinatal or early childhood. Risk of chronicity depends on the age of acquisition and route of transmission and is highest among neonates who acquire infection vertically [6, 7, 8]. Acute HBV infection in the early pregnancy is associated with 10% risk of perinatal transmission [9], but infection close to or during labour may infect more than 60% of neonates [10]. Neonatal HBV infection is often asymptomatic in early life but is associated with increased risk of liver disease in later life. In vertically HBV infected children, risk of developing liver cancer is 200 times more than that of general population [11]. HBV is transmitted through percutaneous or parenteral contact with infected blood, body fluids, and by sexual intercourse [12]. All persons who are hepatitis B surface antigen (HBsAg) positive are potentially infectious. The many millions of people around the world who become HBV carriers are a constant source of new infections for those who have never contracted the virus [26]. Blood is infective many weeks before the onset of the first symptoms and throughout the acute phase of the disease. The infectivity of chronically infected individuals varies for highly infectious (HBeAg positive) to often sparingly infectious (anti-HBeAg positive). Hepatitis B is the only sexually transmitted infection for which there is a protective vaccine [13]. In countries where HBV is highly endemic, the hepatitis B surface antigen (HBsAg) prevalence rate is 8% or higher with most infection occurring during infancy and early childhood. Infection occurs commonly in all age groups although the high rate of chronic infection is primarily maintained by transmission during infancy and early childhood where endemicity is low (HBsAg prevalence rate of below 2%). Infection occurs in young adult, especially those belonging to known risk group. In area with HBV endemicity, perinatal route is the main route of transmission. Perinatal transmission is common especially when HBV infected mothers are also HBeAg positive. HBeAg positive mother are more than 70% likely to transmit HBV while from HBsAg positive, HBeAg negative mother; it is less than 10% [14]. Other high-risk adult populations include person with multiple heterosexual partners, men who have sex with men and healthcare workers. Despite the existence of a safe and effective vaccine, Nigeria has remained a hyper endemic area for hepatitis B virus infection, with an estimated 12% of the total population being chronic carries [15]. Hepatitis virus infection continues to be a substantial and devastating health problem, with new cases still being reported annually [16]. The Prevalence of HBV infection among antenatal population may be a reliable indicator of hepatitis B virus prevalence rate in general population. Hence, screening antenatal women for HBsAg can give a reliable prevalence of the disease in the population and provide an avenue for preventing mother to child transmission of the virus. A demographic Health Survey (DHS) [17] in 2003 showed that in developing countries in Africa, 68% of women report for antenatal care while at least 70% of women reported for antenatal care in Nigeria. About 74% of women who accessed antenatal care in Nigeria are from urban areas. Most women presenting for antenatal care in Nigeria, are most likely to wait until the second trimester and a relatively substantial proportion present only in the third trimester [18]. Seroprevalence study on HBsAg in Nigeria have shown that the prevalence of the infection in pregnant women range from 2–15% [19]. A previous report that investigated the prevalence of hepatitis B among pregnant women in Nnewi Nigeria obtained a prevalence of 6% [20].
Prevalence of hepatitis B in various areas [30]
Prevalence of hepatitis B in various areas [30]
Estimating the prevalence of HBV infection among pregnant women is very important information on the control of vertical transmission of the disease. Pregnancy can potentially be a clinical access point for the antenatal population in Nigeria and other resource limited settings. Effective interventions during pregnancy and child birth can potentially help prevent vertical transmission of HBV in Nigeria and other resource-limited settings [21]. The screening for HBsAg is routine in pregnancy in most developed countries of the world. It is a recommendation of Royal College of Obstetrician and Gynaecologist (RCOG) of the United Kingdom that pregnant women be routinely screened for HBsAg [22].
Diagnosis of hepatitis is confirmed by demonstration in sera of specific antigens and/or antibodies. Three clinically useful antigen-antibody systems have been identified for hepatitis B [Hepatitis B surface antigen (HBsAg) and antibody to HBsAg (anti-HBs); M Antibody (anti-HBcIgM and anti-HBcIgG) to hepatitis B core antigen (HBcAg) and Hepatitis B e antigen (HBeAg) and antibody to HBeAg (anti-HBe)]. The presence of HBsAg indicates that the person is potentially infectious [23]. The presence of HBeAg is associated with relatively high infectivity and severity of disease [24]. Anti-HBc is the first antibody to appear. Demonstration of anti-HBc in serum indicates HBV infection, current or past. IgM anti-HBc is present in high titer during acute infection and usually disappears within 6 months, although it can persist in some cases of chronic hepatitis. This test may therefore reliably diagnose acute HBV infection. IgG anti-HBc generally remains detectable for a lifetime [25]. Anti-HBe appears after anti-HBc and its presence correlates to a decreased infectivity. Anti-HBe replaces HBeAg in the resolution of the disease [26]. Anti-HBs replace HBsAg as the acute HBV infection is resolving. Anti-HBs generally persist for a lifetime in over 80% of patients and indicate immunity [27]. Acute hepatitis patients who maintain a constant serum HBsAg concentration, or whose serum HBeAg persists 8 to 10 weeks after symptoms have resolved, are likely to become carriers and at risk of developing chronic liver disease [28].
During HBV infection, the serological markers vary depending on whether the infection is acute or chronic as described in the table below [29].
The aim of this study is to determine the prevalence of hepatitis B viral markers among pregnant women attending antenatal clinic in Specialist Hospital Sokoto Nigeria. Findings from the study can be used to justify the need for routine testing of pregnant women attending antenatal care in Specialist Hospital, Sokoto State, Nigeria for hepatitis B virus markers. It can also potentially facilitate the formulation of a policy on preventive programmes aimed at reducing the incidence of hepatitis B virus markers. It will also help justify the need for the provision of universal vaccination against hepatitis B in Sokoto State in particular and the Nigerian nation in general.
Methodology
Study site
This study was conducted in the Department of Haematology and Blood Transfusion Science of the School of Medical Laboratory Science, Usmanu Danfodiyo University Sokoto in collaboration with Department of Obstetrics and Gynaecology of Specialist Hospital Sokoto, Nigeria.
Study area
Sokoto State is located in the extreme North Western part of Nigeria near to the confluence of the Sokoto and Rima river with an annual average temperature of 28.3
Study design
This case study is designed to investigate the prevalence of hepatitis B viral markers among 117 consecutively-recruited pregnant women attending antenatal care in Specialist Hospital Sokoto, Nigeria.
Inclusion criteria
The inclusion criteria include; age (
Exclusion criteria
The following were excluded for the study; non-pregnant women, pregnant women
Sample size
In this case study a total of 117 pregnant women attending antenatal clinic at Specialist Hospital Sokoto was screened. Number was calculated using the formula below.
where,
Therefore:
Specimen collection
Three milliliters of venous blood sample was taken from each pregnant woman into a non-anticoagulated sample tube. Blood samples will be allowed to stand at room temperature for clotting and retraction. Thereafter, the samples were centrifuged to give a clear serum. The serum will be separated and stored at
Methods of detection HBV markers
The hepatitis testing will be carried out using the Skytec-Rapid Diagnostic HBV-5 rapid kit (Skytec-Rapid Diagnostic USA). The kit is based on lateral flow chromatographic immunoassay for the qualitative detection of HBsAg, HBsAb, HBeAg, HBeAb, and HBcAb in human serum or plasma. Panel format can conveniently test for five targets at once and utilizes all markers to help distinguish between acute and chronic infections. The product uses the colloidal gold and membrane chromatography technology, and measures HBsAg, HBeAg in serum with dual-antibody sandwich method, and measures HBsAb with dual-antigen sandwich method, and measures HBeAb and HBcAb with neutralization competitive inhibition method.
Data collection and analysis
Data were collected into excel spread sheet and transferred into the data editor of Statistical Package for Social Sciences (SPSS, Version 20) software. Data were expressed as percentages and mean and standard deviation. Statistical significance was compared using Chi-square test. A
Prevalence of hepatitis B virus markers based on ethnicity
Prevalence of hepatitis B virus markers based on ethnicity
Prevalence of hepatitis B virus markers based on age
Prevalence of hepatitis B virus markers among the pregnant subjects based on their education level
Prevalence of Hepatitis B markers among the pregnant subjects.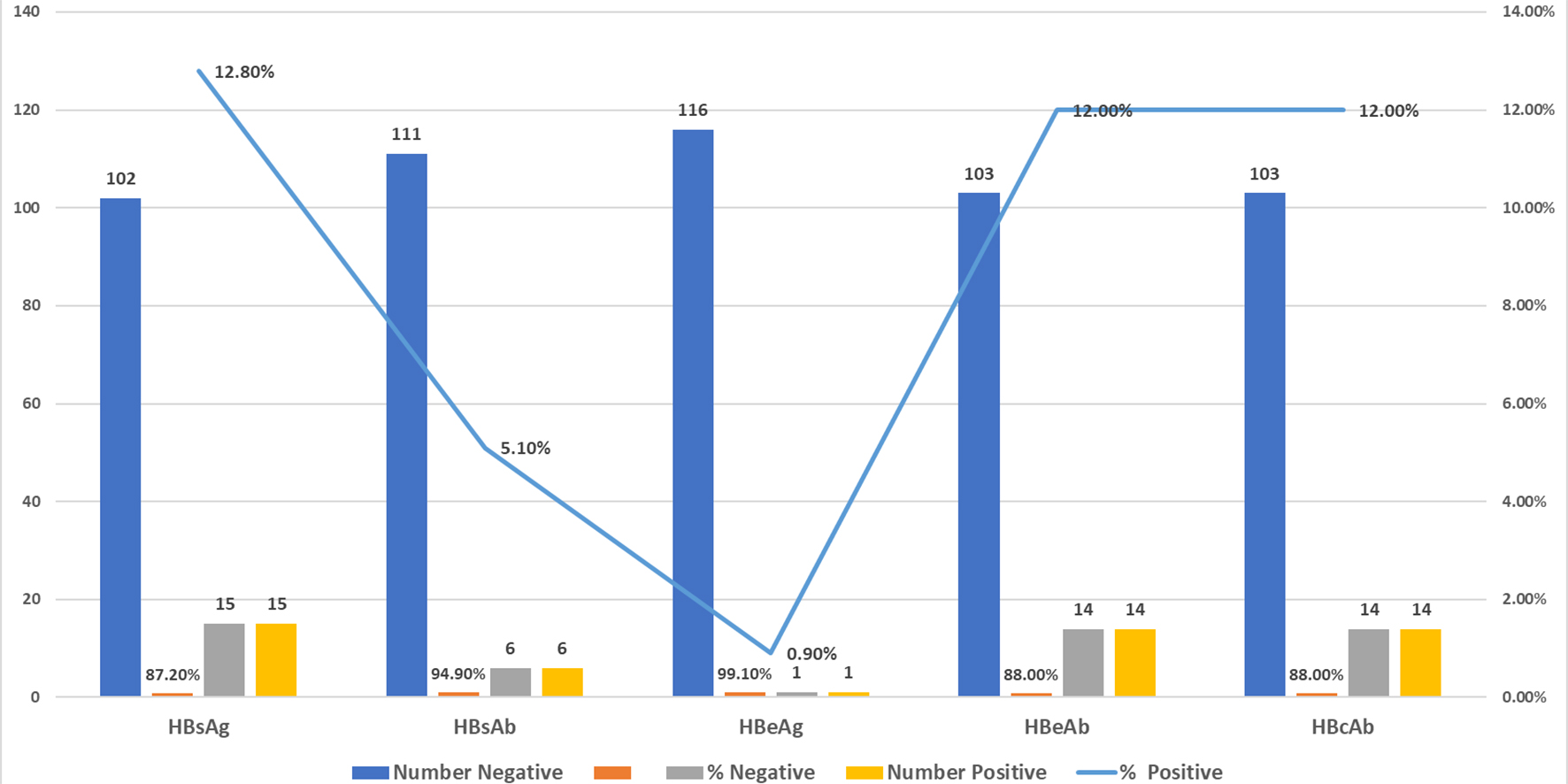
Prevalence of hepatitis B virus markers among the pregnant subjects based on history of previous blood transfusion
Prevalence of hepatitis B virus markers among the pregnant subjects based on previous history of jaundice
Prevalence of hepatitis B virus markers among the pregnant subjects based on employment status
Prevalence of hepatitis B virus markers among the pregnant subjects based on a previous history of still birth
The results of prevalence study of the five-virus marker (HBsAg, HBsAb, HBeAg, HBcAb and HBcAb) are presented below. Out of 117 pregnant women tested, 15 were positive for HBsAg (12.8%), 6 positives for HBsAb (5.1%), 1 was positive for HBeAg (0.9%), 14 tested positives for HBeAb (12.0%), and 14 tested for HBcAb (12.0%). Figure 1 shows the prevalence of Hepatitis B markers among the Pregnant subjects. The prevalence of HBsAg, HBsAb, HBeAg, HBcAb and HBcAb was compared based on ethnicity. HBsAb was significantly higher among the Hausa ethnic group (
Discussion
Viral hepatitis infection remains a public health problem in developing countries. The prevalence of hepatitis B infection varies in different parts of the world from country to country, and from one region to another and from one population group to another in a country [33]. The result of this study showed a 12.8% prevalence for HBsAg among the pregnant women attending antenatal clinic at Sokoto Specialist Hospital Sokoto. This finding is consistent with previous report which indicated a prevalence of 12.8% in General Hospital Minna [34]. Our finding in this study is also consistent with previous reports from different parts of Nigeria; 15.8% in Maiduguri [35], 13.8% in Lagos [36], 11.6% reported in Maiduguri [37], 11% in Makurdi [38], 8.3% in Zaria [39] and 8.2% reported among subjects in North-Eastern Nigeria [40]. Lower prevalence was however observed in other parts of Nigeria; 2.19% in Benin City [41], 4.3% and 2.89% observed in Port Harcourt [42, 43] respectively and 5.7% in Ilorin [44]. Finding from this study is also higher than that reported in other parts of Africa; 6.3% reported among pregnant women in Tanzania [45] and 3.7% in Ethiopia [46]. Among them 205 pregnant women tested in Kenya, the prevalence of HbsAg was 9.3% [47]. A cross-sectional study done at the antenatal clinic of the University College Hospital Ibadan involving one hundred and eighty pregnant women indicated HBsAg prevalence of 8.3% [48].
One of the ways to reducing the prevalence of HBV is by implementing a universal vaccination against HBV. In Nigeria there is absence of universal infant vaccination programme. Universal vaccination against HBV has brought about a dramatic reduction in the prevalence of HBsAg in countries that have implemented nationwide vaccination programme [49]. In a previous report [50] among new students entering a Malaysian University for medical and paramedical studies, the prevalence of HBsAg declined from 1.27% in 2005 to 0% in 2011 as a result of the increasing number of students being vaccinated under the expanded programme on immunization in Malaysia. Student healthcare workers represent a high-risk group for hepatitis B virus (HBV) transmission and should be vaccinated as early as possible before the start of their career. An overview of specific HBV policies in European Union countries indicates that HBV vaccination is mandatory for medical students and student nurses in five countries and recommended in nine. Pre-vaccination testing was done in five countries and serotesting after vaccination in 12 countries [51]. Nigeria and other countries in sub Saharan Africa can potentially learn from these evidenced-based best practices by introducing universal vaccination programme for hepatitis B. Previous reports in Nigeria [52], South Africa [53], Kenya [54], Egypt [55], Pakistan [56], Dominican Republic [57], Lao [58], Cameroon [59], Ethiopia [60] and Brazil [61] all indicated a low level of hepatitis B vaccination uptake, lack of post exposure prophylaxis, poor knowledge and awareness about hepatitis B, a high rate of needle stick injury and low rate of detectable and protective anti HB-S titres among students and healthcare professionals. However, report from studies in developed countries show a significantly higher immunity status and high vaccination uptake as well as availability of post exposure prophylaxis [62]. In most developed countries, as part of occupational safety measures, all health care workers and medical students in training are required to be vaccinated against HBV as a pre-employment and pre-enrolment requirement [63, 64].
The result of this study indicated 12.0% prevalence for HBeAg which is higher than the 11% prevalence observed among 5261 parturient women in Iran [65]. Our observed prevalence of HBeAg of 12.0% is higher than a prevalence of 11% observed in a previous report among pregnant women in Iran [66]. It is however, lower than a prevalence of 15.9% reported among pregnant women in the Philippines [67]. Similarly, out of a total of 1262 pregnant women who were examined for HBeAg in China, a positive prevalence of 0.9% was observed [68]. The majority of people who get HBV infection after the neonatal period tend to clear the virus over time. The natural history of hepatitis B infection follows three phases: immune tolerant, immune active and immune inactive phases. During the immune active phase when the virus is actively replicating and HBV DNA is high, HBeAg becomes positive and the individual is at a higher risk of transmitting the virus. The high prevalence observed among pregnant women in this study has implications on HBV infection in pregnancy and the risk of vertical transmission from mother to child. Pregnant mothers who test positive for both hepatitis B surface antigen (HBsAg) and hepatitis B e antigen (HBeAg) have 70–90% risk of transmitting infection to their newborn infants and about 10–40% risk if they test positive for only HBsAg [69]. Therefore, pregnant women should be routinely screened for HBsAg and hepatitis B vaccine administered at birth to the infants whose mothers test positive [70, 71].
The finding of HBsAb prevalence of 5.1% observed in this study is consistent with a previous report in Madina Almonawara [72] which indicated HBsAb prevalence rate of 7.98%. The prevalence of HBsAb of 5.1% observed in this study is lower than the Hepatitis B seroprotection rates (anti HBsAb
In this study the prevalence of HBcAb obtained was 12.0%. This prevalence is lower than the 75.3% reported among pregnant women in Ghana [77]. Presence of anti-HBs and anti-HBc antibody are indications of previous exposure to HBV infection. Similarly, among pregnant women in China, HBcAb positivity was observed in 23.1% and [68].
In this study the prevalence of HBeAb obtained was 12.0%. Our finding is lower than a 22.6% prevalence observed among a total of 1262 pregnant women screened in China [68]. Also, among pregnant women screened in Kenya, the prevalence of HbeAb was (8.8%) [72]. A cross-sectional study done at the antenatal clinic of the University College Hospital Ibadan involving one hundred and eighty pregnant women indicated HBeAb prevalence of 53.3% [48]. These variations, noticed may be related to the peculiarities in the mode of transmission of HBsAg and difference in HBV Markers dictated by socio-cultural practices and environmental factors.
A higher frequency of HBV infection was found in the 15–20 years age, 21–25 years of age and 31–35 years of age. At these age people are more sexually active. They are also more likely to be involved in high risk behaviours that put them potentially at risk (maintenance of multiple sex partners, having unprotected sexual intercourse, intravenous drug abuse, tattooing and other high risk socio-cultural life styles) that put them potentially at risk for Hepatitis B. This observation is worrisome since the most productive and economically viable age groups of the pregnant women population are most affected. There is the urgent need for renewed intensification of prevention programmes aimed at changing high-risk behaviors among pregnant women. Population in Sokoto is predominantly Muslim. There may be need to build capacity among Islamic Clerics in the area to facilitate their awareness about mode of transmission and ways to prevent Hepatitis B infection. Given proper information and training, religious leaders can become strong allies in hepatitis B infection prevention and control in view of their influence and acceptance among the people they lead. Also, religious organizations can also serve as useful channels for disseminating messages about hepatitis B since congregations do have reverence for places of worship and for religious leaders.
Majority of the pregnant women tested have not had tertiary education. This may be the reason for the high prevalence of HBsAg positivity in this study. Previous report indicated that HBV infection was higher among subjects of low educational status.
Although HBV infection is considered one of the most important occupation infectious hazards in developed countries [78]. The result of this study did not reveal statistical significance between HBV Markers seropositivity and the different occupation of the pregnant women studied. It is however advocated that women who are occupationally exposed to the hepatitis B should be vaccinated against Hepatitis B virus.
In this study the prevalence of HBeAg obtained was 0.9%. Presence of HBeAg is not required for infectivity or replication. It is not part of the structure of the virus. Some patients with active viral replication do not produce HBeAg due to the presence of HBV variants. The presence of HBeAg indicates active viral replication in hepatocytes with high risk for developing hepatocellular carcinoma [79]. In the study, women positive for HBeAg accounted for 26.7%. HBeAg transverses the placenta and induces an immune tolerance to the capsid viral antigen and elimination of infected hepatocytes in the infected newborn is therefore impossible without intervention [80]. A cross-sectional study done at the antenatal clinic of the University College Hospital Ibadan involving one hundred and eighty pregnant women indicated HBeAg prevalence of 26.7% [48]. The HBV e antigen (HBeAg) comes from the core of the HBV and is a portion of the core. When the core of the HBV degrades in the serum, this antigen is created and can be detected. Because HBcAg will be totally degraded in the serum, it is not detectable in the serum. Thus, when the HBeAg marker becomes positive, it is equivalent to a positive HbcAg marker and shows that the Hepatitis B virus is replicating actively and the patient is infectious. The HBV e antibody (HBeAb) is the body’s immune reaction to the HBeAg and like HbsAb, it can combine with the HbeAg. It usually appears after the HBeAg turns to negative, which also means that the HBV replication activities have decreased and the patient is less infectious or not infectious at all.
Conclusion and recommendations
The study observed a high prevalence of various hepatitis B viral markers among pregnant women attending antenatal care in Specialist Hospital Sokoto. Since the virus can be transmitted from infected mother to the offspring especially at birth, the presence of hepatitis B infection in women in general and pregnant women in particular calls for concern. There is need for routine screening of all pregnant women and infants born to hepatitis B positive mothers. Government and non-governmental organizations should intensify efforts to enlighten the general population on the public health importance of the disease and the importance of hepatitis screening. There is also need for the development of a treatment protocol for the management of pregnant women positive for hepatitis B to prevent mother to child transmission. There is an urgent need for the implementation of evidenced- based best practice of providing universal vaccination against hepatitis B for all hepatitis B negative women of child bearing age in particular and all Nigerians in general.