
Abstract
BACKGROUND:
Calcium and vitamin D deficiency is common among Iranian women of childbearing age and poses adverse effects on pregnancy outcomes. The aim of the current study was to determine the prevalence of vitamin D and calcium in a sample of Iranian pregnant women and to assess its correlation with the feto-maternal outcomes.
METHODS:
In this prospective cross-sectional study, a sample of pregnant women between 15 to 45 years who were in the third trimester were recruited from a number of hospitals in Tehran. Data were collected by the means of a self-developed questionnaire, interviews, physical examination, and paraclinical tests including measuring the serum level of calcium, vitamin D, parathormone (PTH) and phosphorous (Pi). The questionnaire obtained information on age, level of education, socio-economic status, parity, gravidity, calcium intake during pregnancy, as well as feto-maternal outcomes.
RESULTS:
We included a total number of 233 singleton pregnancies. Most of the subjects (58.4%) had vitamin D deficiency and 12.0% suffered from severe vitamin D deficiency. Vitamin D deficiency was adversely associated with the years of education (
CONCLUSION:
The prevalence of vitamin D deficiency during pregnancy among Iranian women is extremely high and is associated with adverse pregnancy outcomes including cesarean delivery, neonatal jaundice and neonatal respiratory infections. Low vitamin D supplementation and sun exposure, lack of physical activity and high BMI are the etiologies. Increasing the knowledge along with vitamin D supplementation during the pregnancy is recommended in Iranian population.
Keywords
Introduction
Calcium and vitamin D deficiency is a global concern compromising the health of mother and infant in pregnancy [1, 2, 3, 4]. A majority of Iranian population have some degree of hypovitaminosis D deficiency, which is even more prominent in young women despite the sunny climate [5]. This is often attributed to the limited sun exposure due to the official norm of clothing for women which obliges almost full body coverage [6], along with an insufficient dietary calcium intake [7].
The maternal calcium and vitamin D status are indicative of satisfactory neonatal calcium hemostasis, skeletal maturation and bone mineralization [8]. Metabolic alterations occur to maintain a constant serum level of ionized calcium during pregnancy. It has been shown that serum concentrations of vitamin D are especially elevated in the third trimester to fulfill the fetal demand, mainly via enhancing the intestinal absorption of calcium [9, 10]. In case the level of vitamin D is below optimal and fails to suppress parathyroid hormone (PTH), PTH will stimulate maternal bone resorption [10].
Supplementation with calcium and vitamin D has been reported beneficial in prevention of several maternal and fetal complications [11, 12, 13], such as gestational hypertension, preeclampsia, neonatal death, preterm birth [14], gestational diabetes mellitus, being small for gestational age [15], maternal morbidity and mortality [16], rickets, craniotabes [17, 18] and impaired intrauterine skeletal growth [19]. Furthermore, serious consequences including hypocalcemic seizures and dilated cardiomayopathy may pose life-threatening risks on the infants [20].
The high prevalence of calcium and vitamin D deficiency in our country augments the vulnerability of pregnant women and newborns to the negative impacts of this public health issue. Currently, there are no guidelines and standard recommendations for routine administration of calcium and vitamin D supplements in pregnancy. To improve the existing policies, obtaining a full understating of the current status and identification of high-risk individuals is necessary. Thus, we assessed the prevalence of calcium and vitamin D deficiency and its correlates in this specific population and investigated the scope of associated feto-maternal complications.
Material and methods
Patients and settings
In this prospective cross-sectional study, women between 15 to 45 years who were in the third trimester of pregnancy were recruited from a number hospital in Tehran. Among all hospitals with obstetrics and gynecology wards, centers which could best represent the general population based on location and socio-economic factors were selected using stratified systematic sampling method. These hospitals were ShahidMostafa Khomeini, Mahdieh, Shohadaye Tajrish, Bahman and Arash. Subsequently, patients were enrolled via simple sampling method from March 2013 to March 2014. Exclusion criteria consisted of parathyroid or adrenal gland disorders, vitamin A and D overuse, granulomatous disease, renal dysfunction, hypoalbuminemia, thyrotoxicosis, sepsis, chemotherapy, blood transfusion, and the use of magnesium sulfate, lithium or thiazide medications. Patients were required to provide informed written consent priorto participation. The study protocol was designed according to the Helsinki Declaration of bioethics and approved by the institutional review board (IRB) and medical ethics committee of Shahid Beheshti University of Medical Sciences. All the patients provided their informed written consents before inclusion in the study.
Data gathering
Data were collected by the means of a self-developed questionnaire, interviews, physical examination, and paraclinical tests including measuring the serum level of calcium, vitamin D, parathormone (PTH) and phosphorous (Pi). The questionnaire obtained information on age, level of education, socio-economic status, parity, gravidity, calcium intake during pregnancy, as well as feto-maternal outcomes. Investigated maternal outcomes were preeclampsia, gestational hypertension, gestational diabetes, cesarean section, premature rupture of membranes (PROM), and preterm labor. For evaluation of fetal outcome, gestational ageat birth, birth weight, jaundice, craniotabes, hypocalcemia-induced seizure and congenital anomalies were considered for as long as 28 days after birth.
Validation of the questionnaire
Ten specialists comprising of three obstetrics- gynecology physicians, two endocrinologists, three epidemiologists and two biomedical statisticians reviewed and scored the questions in three domains (relevance, clarity and simplicity) using a 4-point Likert scale ranging from 1 (completely irrelevant, vague, not-understandable) to 4 (completely relevant, clear, understandable). Afterwards, mean scores in all the three domainswere calculated for each question. Accordingly, some questions were omitted (average score below 2 points) or modified (average score between 2 to 3 points). Also, the specialists assessed the importance of questions. Using Lawshe’s method, content validity was quantified and content validity ratio (CVR) and content validity index (CVI) were calculated. To ensure test-retest reliability, 30 participants filled out the questionnaire for a second time after two weeks. Cronbach’s alpha coefficients were calculated to be 0.6.
Variables and outcome measures
We recorded the serum levels of the vitamin D, calcium, parathormone and phosphorus. The 25-hydroxy Vitamin D was categorized as severe deficiency (
Statistical analysis
A total of at least 233 subjects were estimated to be sufficient (power
Data were analyzed using statistical package for social sciences (SPSS Inc., Chicago, IL, USA) version 24.0. We also used R 3.4.2 software for correlation analysis. “R2OpenBUGS” and “coda” packages have been used for Bayesian analysis. All the data are presented as mean
Results
A total of 233 pregnant women with the mean age of 28.37
The baseline characteristic of 233 pregnant people included in the current study
The baseline characteristic of 233 pregnant people included in the current study
As demonstrated, most of the subjects (58.4%) had vitamin D deficiency and 12.0% suffered from severe vitamin D deficiency. Table 2 summarizes the serum levels of vitamin D, calcium, phosphorus and parathormone D deficiency. The prevalence of vitamin D deficiency was calculated to be 72,103 in 100,000 populations. However, only 8 (3.4%) patients had calcium deficiency and 4 (1.7%) patients had phosphorus deficiency (Table 2).
Table 3 summarizes the association between the serum level of vitamin D and demographics, consumption of food and supplements, physical activity, sun exposure and maternal and neonatal outcome. We found that the serum level of PTH was correlated with serum level of vitamin D (
The serum levels of calcium, Vitamin D, parathyroid hormone and phosphorous in 233 pregnant women included in the current study
Serum characteristics, demographic, lifestyle factors, sun exposure, body composition, maternal and neonatal complications across 25 (OH) D status
BMI: Body Mass Index; MET: Metabolic Equivalent of Task; PTH: Parathormone;
Protective or risk factors for severe deficiency of 25 (OH) D based on Bayesian multiple logistic regression
Receiver-operating characteristics (ROC) curves of predicted probability of model and PTH for severe deficiency of 25 (OH) D. The area under curve (AUC) was calculated to be 0.89 (0.84–0.95) indicative of moderate accuracy.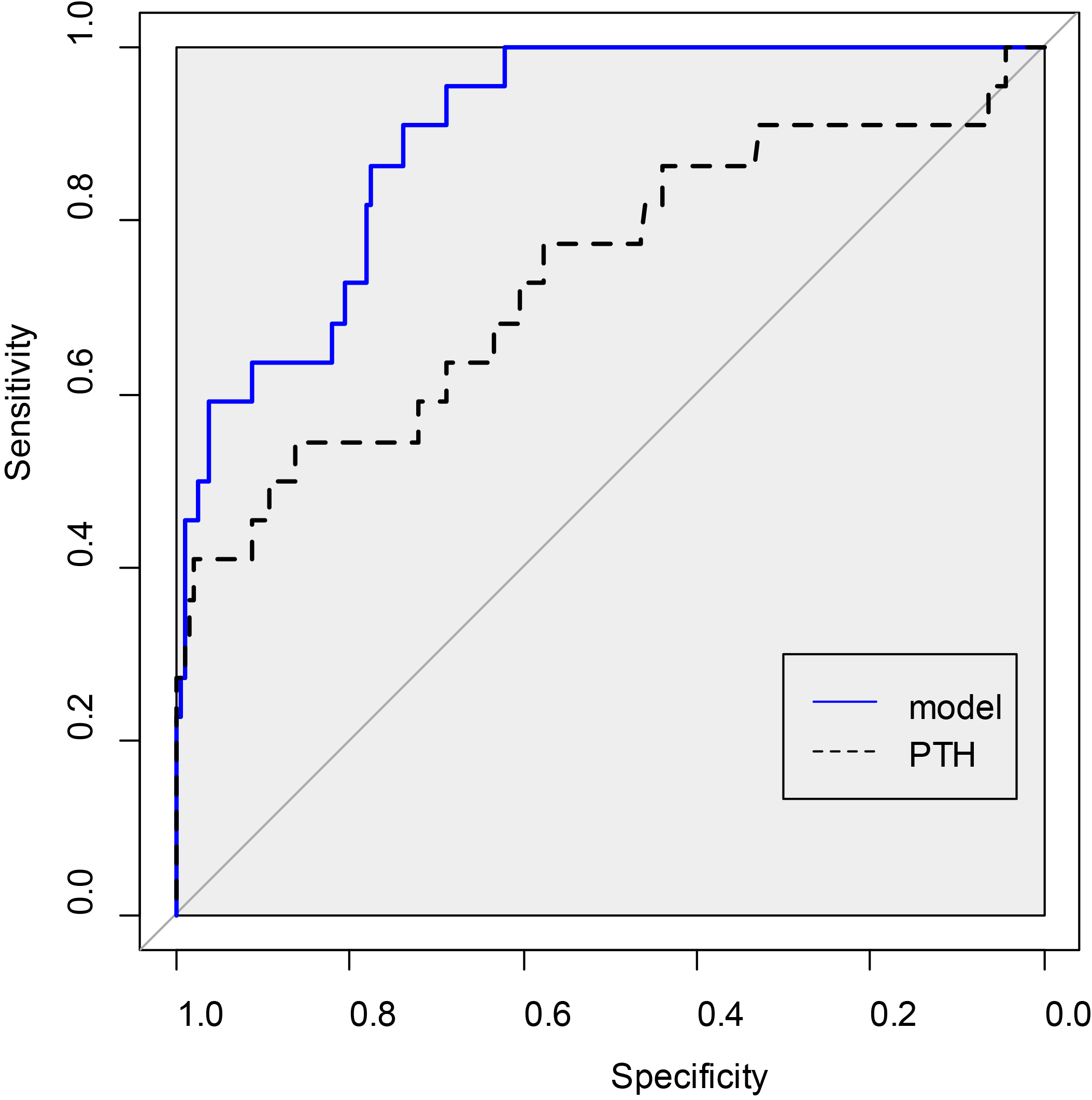
Several lines of evidence suggest that vitamin D deficiency during the pregnancy is associated with adverse pregnancy outcome. In the current study we tried to investigate the prevalence of vitamin D deficiency in singleton pregnancies in capital of Iran. We found that vitamin D deficiency was adversely associated years of education, exercising, MET, sun exposure and BMI. Vitamin D deficiency was also associated with higher rate of cesarean delivery, higher rate of diastolic hypertension, neonatal jaundice and higher rate of neonatal respiratory infections. These finds suggest that vitamin D is a common health problem during the pregnancy which is associated with significant adverse pregnancy and neonatal outcomes.
Several studies have investigated the associated between the adverse pregnancy outcomes and the serum level of vitamin D [21, 22, 23, 24]. Recently, Xu et al. [24] demonstrated that low 25 (OH) D concentrations at the first prenatal visit were associated with increased risk of GDM and might be useful in identifying women at risk of GDM for performing early prevention strategies. In another study, Wang et al. [22] demonstrated that maternal vitamin D insufficiency is common during pregnancy and is independently associated with low birth weight and high risk of small for gestational age in term infants. In a systematic review, Chu et al. [21] reported that there is an association between vitamin D status and reproductive treatment outcomes achieved in women undergoing assisted reproductive techniques (ARTs). They demonstrated that vitamin D deficiency and insufficiency could be important conditions to treat in women considering ARTs [21]. These results are in line with our findings. We reported a high rate of vitamin D deficiency in our series and a strong association was found between the low birthweight, neonatal respiratory infections and NICU admission and vitamin D deficiency. As reported in our results, only a small portion of the subjects in our series received vitamin D supplementation during their pregnancy which is extremely lower that previously reported rates and recommendations [23].
In a study from The Netherlands, the mean serum level of vitamin D was significantly lower in non-western women compared to western women independent of age, socio-economic status and parity [25]. A population-based study on pregnant women and their neonates in Australia reported an overall vitamin D deficiency among 15% of mothers and 11% of neonates. Risk factors were late winter/early spring, birthplace outside Australia, dark skin phenotype, wearing a veil and younger maternal age [26]. In contrast, a country with abundant sunshine such as India has unexpectedly high prevalence of deficiencies, as over 80 percent of rural and urban women are reported to have low calcium intake, below normal vitamin D values and above normal PTH level [27, 28] with significant differences compared to men [28]. In a cohort study in Doha on over 1,800 pregnant women, almost half had vitamin D deficiency. Age below 30 years and low income, as well as inadequate sunlight exposure, daily physical activity and vitamin D supplement intake were risk factors for hypovitamosis D. This problem elevated the risk of GDM, anemia, and preeclampsia [29]. Vitamin D insufficiency and deficiency is frequent among Caucasian women with a prevalence of approximately 90% [30].
The figures seem to be similar in Iran. In a report by Bassir et al., 80% of mothers, who were evaluated at the time of delivery had vitamin D concentrations below 25 nmol/l and PTH level above normal range. However, serum calcium was within the normal range. As a result, vitamin D was nearly undetectable in newborns of deficient mothers [31]. Evaluation of serum calcium in pregnant women in Zabol, Iran showed a constant level along first, second and third trimesters, rising from 8.3 to 8.6. It was revealed that maternal serum calcium level influences the birth weight of neonates [32]. However, Abbasian et al. reported the prevalence of calcium deficiency (
Given the alarming status of this preventable problem, researchers have sought to improve the deficiency via supplementation. In a randomized clinical study on pregnant women at 27 weeks’ gestation, a daily dose of 800 IU vitamin D was more efficient than a single oral dose of 200000 IU vitamin D. Yet, normal level was achieved in a small ratio of treated women [34]. Although vitamin D-containing supplements help increase the serum level, conservative dosages do not have the desired effect [30]. It is suggested that 4,000 IU/day vitamin D3 is necessary to “normalize” vitamin D metabolism and improve birth outcomes including primary cesarean section and comorbidities of pregnancy with no risk of side effects [35]. In a randomized clinical trial by Asemi et al., 500 mg calcium-200 IU cholecalciferol supplements were administerd versus placebo for nine weeks. Consumption of calcium-Vitamin D co-supplements resulted in a significant reduction of serum high-sensitivity C-reactive protein, significant elevation of plasma total antioxidant capacity serum 25-hydroxyvitamin D, and calcium levels. We saw no significant change of the co-supplementation on pregnancy outcomes as well [36].
We note some limitations to our study. The sample size was robustly selected to match the calculated one which might be a heterogeneous group. However, our study had 80% power to detect significant differences regarding the pregnancy outcomes. In addition, we selected the patients form a vast area and several centers which might lead to selection bias. We recommend the future studiesto follow the neonates to assess the long-term effects of maternal vitamin D deficiency and neuropsychiatric development. Overall, further studies with larger study population and longer follow-up periods are recommended.
In conclusion, the prevalence of vitamin D deficiency during pregnancy among Iranian women is extremely high and is associated with adverse pregnancy outcomes including cesarean delivery, neonatal jaundice and neonatal respiratory infections. Low vitamin D supplementation and sun exposure, lack of physical activity and high BMI are the etiologies. Increasing the knowledge along with vitamin D supplementation during the pregnancy is recommended in Iranian population.
Footnotes
Acknowledgments
We would like to thank all the patients and their families who participated in this study. We would also like to acknowledge the editorial assistance of Diba Negar Research Institute for improving the English and style of the manuscript.
Conflict of interest
There isn’t any conflict of interest to be declared regarding the manuscript.