
Abstract
Monoclonal antibodies and vaccines have widely been studied for the immunotherapy of cancer, though their large size appears to limit their functionality in solid tumors, in large part due to unique properties of tumor microenvironment. Smaller formats of antibodies have been developed to throw such restrictions. These small format antibodies include antigen binding fragments, single-chain variable fragments, single variable domain of camelid antibody (so-called nanobody (Nb) or VHH). Since their serendipitous discovery, nanobodies have been studies at length in the fields of research, diagnostics and therapy. These antigen binding fragments, originating from camelid heavy-chain antibodies, possess unusual hallmarks in terms of (small) size, stability, solubility and specificity, hence allowing cost-effective production and sometimes out performing monoclonal antibodies. In addition, these small camelid heavy-chain antibodies are highly adaptable tools for cancer research as they enable specific modulation of targets, enzymatic and non-enzymatic proteins alike. Molecular imaging studies benefit from the rapid, homogeneous tumor accumulation of nanobodies and their fast blood clearance, permitting previously unattainable fast tumor visualization. Moreover, they are endowed with considerable therapeutic potential as inhibitors of receptor-ligand pairs and deliverers of drugs or drug-loaded nanoparticles towards tumors. In this review, we shed light on the current status of nanobodies in diagnosis and imaging of tumor and exploiting nanobodies revert immunosuppressive events, modulation of immune checkpoints, and as deliverers of drugs for targeted tumor therapy.
Keywords
Introduction
Advantages of nanobodies over conventional monoclonal antibodies
Advantages of nanobodies over conventional monoclonal antibodies
Representation of a heavy-chain antibody (HcAb) and its antigen binding fragment, called nanobody. A. In comparison to a monoclonal antibody (mAb), which includes two heavy and two light chains, a HcAb only contains heavy chains. Moreover, HcAbs also lack one constant domain, the antigen binding region only consists of a single fragment, called a nanobody. The tail region of the antibodies forms the Fc part and is able to trigger the immune system. B. Schematic representation of the nanobody entity, composed of framework regions (FR1–4) alternated with three complementary determining regions (CDR1–3). Mutations in FR2 region renders the structure more hydrophilic as compared to conventional antibody fragments. Moreover, the CDR3 loop is extended and enables recognition of hidden or buried epitopes.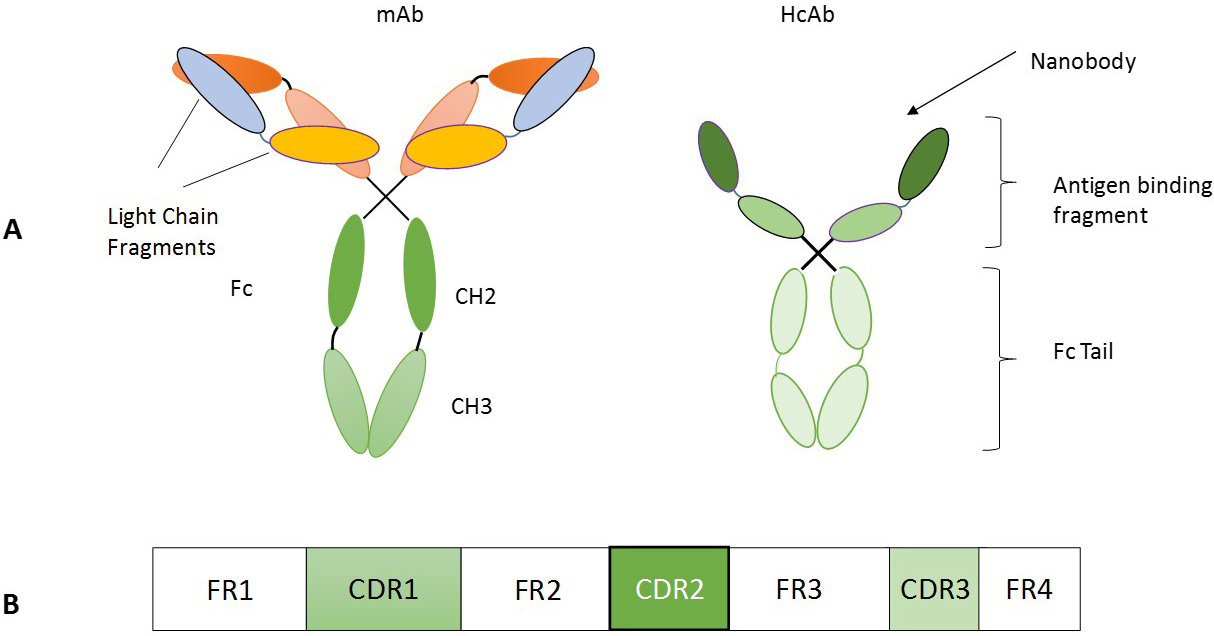
Summary of therapeutic nanobodies in clinical trials
Monoclonal antibodies and vaccines have been extensively studied for the diagnostics and treatment of many diseases including cancer [1, 2]. The large size though limits the function of monoclonal antibodies in solid tumors, in large part due to unique properties of tumor microenvironment such as high pressure of tumor interstitial fluid [3]. In order to tackle such limits, smaller formats of antibodies have been developed, including antigen binding fragments, single-chain variable fragments, single variable domain of camelid antibody (so-called nanobody (Nb) or VHH) Fig. 1 [4, 5]. The existence of efficient heavy-chain-only antibodies in the serum of camelids (dromedaries, camels, llamas, alpacas, guanacos and vicuñas) was revealed serendipitously nearly 30 years ago [6]. These heavy chain-only antibodies (HCAbs) display alike affinity to their cognate antigen, even though these have only one single variable domain (VHH) for antigen recognition [7]. Studies have revealed that these autonomous VHH are the smallest natural intact antigen-binding fragment and retain their full antigen-binding potential [8, 9]. Nanobodies have a very small size (15 kDa) and dimensions in the nanometer range (
Cancer is considered a cluster of diseases with different molecular changes, including gene mutations and amplifications, copy number alterations, changes in tumour suppressor and DNA repair genes, and epigenetic modifications. Development of a successful tumour therapy is challenging due to low specificity of the drug and toxic effect on adjacent non-tumour cells. Besides the surrounding tumor microenvironment which include stromal components such as CAFs, TAMs TANs, Endothelial Cells etc. and non-stromal components such as ECM, etc., promote tumorigenesis by limiting drug efficacy in tumors and inducing drug resistance [14, 15, 16]. A dynamic targeted therapy relies on the specific delivery of an active drug to the target using different possible affinity reagents such as those mediated by a lectin-carbohydrate, ligand-receptor or antibody-antigen recognition [17, 18, 19]. Apparently, for maximal effect, the specific receptor targeted by the affinity reagent should be overexpressed at the surface of the diseased cells. Thus, active targeting refers to site-specific ligand-mediated accumulation of drugs into the diseased site due to an increased expression of a specific biomarker for that malignancy [20]. During the past few decades monoclonal antibodies (mAbs) have been widely used as a treatment modality for cancer therapy. The mAbs strongly diminish the growth of tumor cells by binding to their transmembrane receptors, growth factors, or cytokines, through inhibiting the cognate signal transduction or inducing apoptosis [2, 21]. However, the large size (
Bispecific nanobodies in targeted tumor therapy
Bispecific nanobodies in targeted tumor therapy
Antibody fragments with therapeutic potential. A conventional antibody comprises two heavy and two light chains while a nanobody or HcAb contains heavy chains only. Single-chain variable fragment (scFv) is a class of engineered antibodies generated by the fusion of the heavy (VH) and light chains (VL) of immunoglobulins through a short polypeptide linker. BsAbs combine specificities of two antibodies and simultaneously address different antigens or epitopes. At present, three forms of bi-specifics exist with definite benefits viz., the bi-specific T-cell engager (BiTE), dual-affinity retargeting proteins (DARTs), and tandem diabodies (TandAbs). Abbreviation: bsAb, bispecific antibodies; bsFab, bispecific Fab fragment; HcAb, heavy chain only antibodies.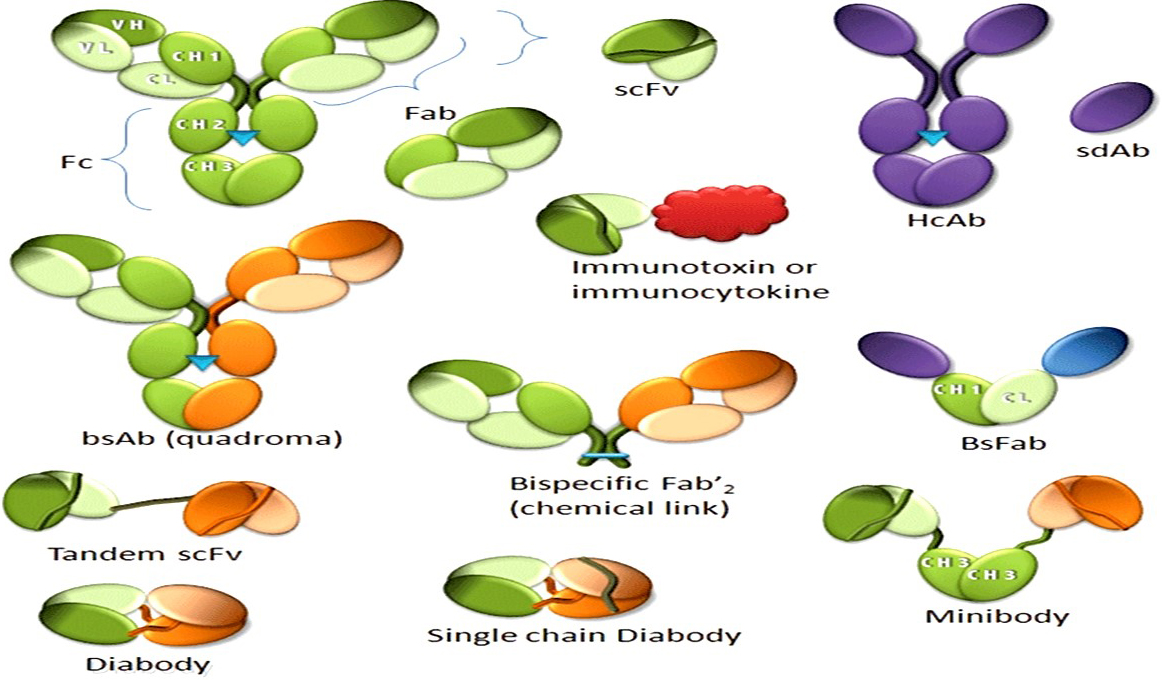
Schematic depiction of the bridging of B-cells and CD8
T-lymphocytes and their subsets are crucial component of the adaptive immune system and demonstrate significant antitumor activity [25]. T-cells secrete granzymes and perforins, thereby induce tumor cell death and chemokines promoting recruitment and activation of other immune cells to counter tumor activities [25]. Conversely, tumor cells and the surrounding living and non-living stroma secrete factors such as chemokines etc. promoting suppression of T-lymphocytes to supress the anti-tumor immune response [26]. Nevertheless, many therapeutic approaches involving nanobodies have been employed to offset the tumor induced inactivation and suppression of T-cells. Studies revealed that the checkpoint inhibitors in combination with bi-specific antibodies promotes T-cell linkage with tumour cells which reduces tumour mass and tumor induced immune suppression [27]. Several nanobodies have been thus developed to target tumor tissues (Table 3) [28, 29, 30, 31, 32]. At present, three forms of bi-specifics exist with definite benefits viz., the bi-specific T-cell engager (BiTE), dual-affinity retargeting proteins (DARTs), and tandem diabodies (TandAbs) Fig. 2 [33]. BiTE nanobodies (such as Blinatumomab) are comprised of two scFv fragments and were developed to bridge T-cells with tumour cells. Among the two scFv fragments, one scFv fragment binds T-cell markers (such as CD3) while the other scFv fragment binds antigens on the tumor cells, in this manner bridging tumour cells and T-cells [34]. Blinatumomab is an FDA approved nanobody, developed to treat the aggressive leukemia (B-cell lymphoblastic leukemia (ALL)) [35]. The nanobody was FDA approved and binds T-cells (CD3) and B-cells (CD19) markers connected with a glycine-serine linker and demonstrated significant efficacy Fig. 3. The main problem with blinatumomab is its short half-life, and therefore entails high therapeutic dosage to reach requisite T-cell activation [36].
To overcome the short half-life of BiTEs, Dual affinity retargeting proteins (DARTs) have been developed as an alternative. Unlike BiTEs, DARTs have hetero-dimerised Fv fragments, with the VL of target A and VH of target B on Fv1 fragment and the VL of target B and VH of target A on the Fv2 fragment [37]. These combinations mimic the natural IgG molecule and have increased the half-life/serum retention of these nanobody molecules from 1.25
Schematic depiction of the PD-L1 inhibiting nanobody KNO35 in the treatment of cancer. A. The tumour cells induce immunosuppression by exploiting the immune checkpoints such as PDL1/PD-1 axis. B. Inhibiting the immune checkpoints using nanobodies such as KNO35 reverts the tumor induced immunosuppression and subsequent development of anti-tumor immune response.
The effector components of the immune system are regulated by immune checkpoints to prevent autoimmune diseases and induce self-tolerance. However, cancer cells in combination with tumor stroma components exploit this mechanism and evade immune surveillance to suppress the immune response and establish the tumour microenvironment [42]. T-cells and natural killer cells mainly express checkpoint receptors such as CTLA-4, TIM-3, PD-1, LAG-3, and PD-L1 [43, 44]. Several drugs, monoclonal antibodies and small molecules have been developed to inhibit immune checkpoints, promoting antitumor immune response [45]. However, the conventional antibody checkpoint inhibitors exhibit low binding affinity, low penetration, decrease stability and production [46]. KN035 nanobody developed against the PD-L1 receptor demonstrated enhanced affinity (approx. 1000 times) for the PD-L1 receptor compared to the conventional mAb [47]. KN035 binds to the PD-L1 receptor through a loop of 21 amino acids by hydrophobic and ionic interactions with Ile54, Tyr56 and Arg113 residues [48]. Binding of KNO35 to the PD-L1 receptor promotes subsequent activation of T-cells thereby inducing anti-tumor response Fig. 4. Similarly, a nanobody known as sdAbK2 was developed against PD-L1, which has a dual role in diagnosis (nuclear imaging), as well as a therapeutic agent with a binding affinity of 3.75 nM, equivalent to avelumab, an anti-PD-L1 monoclonal antibody [49]. This nanobody also showed excellent performance when labelled with technetium-99m for diagnosis and screening of PD-L1 elevated breast cancer, melanoma and kidney cancer with high signal to noise ratio [50].
Furthermore, a ground breaking approach to synthesise and deliver a checkpoint inhibitor antibody/ nanobody using probiotic bacteria was developed to overcome toxicity issues with conventional checkpoint inhibitors [51]. Besides, advances in synthetic biology facilitated the development of genetically engineered bacteria with genes for desired therapeutic proteins and a lysis circuit operon (Synchronized Lysis Circuit) [52]. These bacteria grow and replicate until a threshold population density is reached and undergo cell lysis releasing the synthesised therapeutics which can further be used as a drug delivery vehicle [53]. Similarly, Gubatri et al. developed a probiotic E. coli Nissle 1917 system expressing genes for dynamic lysis and for nanobodies against PDL-1 and CTLA-4 [54]. This system was further tested in syngeneic mice models and demonstrated significant systemic immune response with enhanced T-cell activation [54]. TIM-3 (T-cell immunoglobulin and mucin domain 3) is also a crucial component of immune checkpoints and several inhibitors have been developed to target TIM-3 during cancer therapy. In vitro studies involving novel nanobody developed to inhibit TIM-3 receptor displayed significant anti-proliferative activity in an acute myeloid leukemia cell line [55]. However, manipulating immune checkpoints can also cause substantial toxicities and off target affects that require expert management.
Nanobody drug conjugates as tumor therapy
Chemotherapy is the use of drugs to destroy rapidly growing cells in the body, however, the challenge with this approach and to a lesser extent radiotherapy is off-target effects, which leads to acute toxicity in healthy cells [56]. The combinatorial approach involving use of targeted therapy such as an antibody/nanobody with a non-targeted therapy like chemotherapy was an advance on previous approaches [57, 58]. Fang et al. used a VHH7 domain (
Photo-thermal therapy is an emerging approach to induce tumour cell death by combining photosensitisers (nanoparticles) and laser light. These nanoparticles generate heat and reactive oxygen species when absorbed and excited by lasers (NIR), and induce tumour cell death. Branched gold nanoparticles are one such photosensitiser which showed promising results in killing cancer cells [61]. Bieke et al. [20] developed a nanobody conjugated with branched gold nanoparticles against human epidermal growth factor receptor 2 (HER2). These nanobodies showed high binding affinity for HER2 prominent in breast and ovarian cancers and destroyed HER2 positive SKOV3 cells within five minutes of irradiation [20]. These nanobodies may present as an effective targeted photothermal therapy. Photodynamic therapy is a similar approach where tumour cell death is induced by singlet O2 produced upon irradiation [61]. In light of this, a nanobody conjugated with IRDye700DX (photosensitizer) against EGFR was developed and anti-tumour activity was examined in an orthotopic mouse. It was observed that nanobody conjugated with IRDye700DX induced 90% tumour cell necrosis one-hour post injection [62]. Another approach to manipulate nanobodies in therapeutics is the nanobody-enzyme conjugates, which have showed promising activity in tumour elimination. cAb-CEA5:
Nanobodies in diagnostics and imaging
In addition to their use as therapeutic agents nanobodies also make highly effective and non-invasive molecular imaging reagents and diagnostic tools due to their high penetration, quick elimination, low immunogenicity and ease of production and selection [65, 66, 67]. Early diagnosis of tumors is essential to augment odds of survival. Nbs supported by their small size, high stability, and high target specificity and affinity have been engineered into Nb-detective constructs for non-invasive in vivo molecular imaging [68, 69]. The constructs developed reach promptly a maximal contrast between signal in the pathological tissues and that in healthy tissues [66, 69]. For optimal in vivo molecular imaging, promptness in reaching maximal contrast is crucial. Furthermore, Nbs have a very short half-life and the excess of non-targeting Nbs are rapidly cleared from the bloodstream due to rapid clearance via kidney and bladder. This rapid clearance from blood assures a high tumor to background ratio at early time points after administering the Nb probe [70]. Several imaging techniques have been developed to date for clinical application and manifestation, such as single photon emission computed tomography (SPECT), magnetic resonance imaging (MRI), optical, ultrasound, and photo-acoustic imaging positron emission tomography (PET), computed tomography (CT) [71]. In following sections, we will be shedding light on how nanobodies can be manipulated in detecting and defining tumor markers and nanobodies in molecular imaging.
Nanobody based probes in tumor imaging
Nanobody based probes in tumor imaging
In addition to tumor therapy, nanobodies can aid in early diagnosis and cancer prevention by identifying or defining tumor biomarkers. Furthermore, study performed by Chen et al. [72] in detection of cancer biomarker alpha-fetoprotein (AFP) guarantees that the application can withstand harsh conditions. The subtlest detection (0.0005 ng/mL) was achieved utilizing anti-AFP nanobodies in immune-PCR [72]. In vitro cell-based ELISA assays involving nanobodies developed for the detection of carbonic anhydrase IX enzyme (CAIX), tumor-associated glycoprotein 72 (TAG-72), HER2, and prostate-specific membrane antigen PMSA, demonstrated momentous outcomes [73, 74, 75, 76]. Besides, use of multiple or a mixture of nanobodies demonstrated an improved performance. In addition, nanobodies used to detect cancer biomarker alpha-fetoprotein (AFP) touched a detection limit of 0.47 ng/mL. Patris et. al. proposed a chip format sandwich ELISA with anti-HER2 nanobodies covalently bound onto a screen-printed electrode (SPE) with a detection limit of 1
The generation of single domain nanobody is less costly compared to conventional antibodies and therefore a sophisticated and dissolute approach to generate nanobodies against (unknown) cancer biomarkers is by performing immunization with patient samples. Utilising this strategy lead to in the identification of a novel breast cancer-specific biomarker, cytokeratin 19 [78]. Likewise, nanobody based reverse proteomics was exploited in glioblastoma multiforme (GBM) and further mass-spectrometry analysis on nanobody-antigen pairs, the new GBM biomarkers TRIM28 and
Nanobodies in molecular imaging
Nanobodies have very low molecular weight compared to conventional monoclonal antibodies and have small size that is exceedingly strategic especially in the field of molecular imaging as it enables rapid tumor accumulation and homogenous distribution as well as efficient blood clearance, contributing to high tumor-to-background ratios [80]. Besides, conjugation of several kinds of imaging agents with nanobodies and their high specificity renders their use relatively safe [80, 81]. Many techniques have developed which involve use of nanobodies for imaging tumors including SPECT, PET etc. Single-photon emission computed tomography (SPECT) is a
8B6 a
Positron emission tomography (PET) and single photon emission computed tomography (SPECT) images obtained using nanobodies that are labelled with distinct radionuclides in preclinical and clinical studies. I. Uptake of 
At present,
Recently, a study exploited the extra cellular matrix (ECM) targeting for non-invasive imaging of tumor progression, metastasis, and fibrosis using a nanobody NJB2, specific for an alternatively spliced domain of fibronectin. The study revealed that in in vivo immuno-PET/CT imaging, NJB2 detects primary tumors and metastatic sites with excellent specificity in multiple models of breast cancer, including human and mouse triple-negative breast cancer, and in melanoma. Furthermore, NJB2 was able to detect not only PDAC tumors but also early pancreatic lesions called pancreatic intraepithelial neoplasias, which are challenging to detect by any current imaging modalities, with excellent clarity and signal-to-noise ratios that outperformed conventional 2-fluorodeoxyglucose PET/CT imaging [101]. Also, OA-cb6 nanobody with
Nanobodies, nanobody-based heavy chain antibodies, and nanobody-drug conjugates have a huge potential as antitumor therapeutics. Nanobodies may overcome some of the obstacles that hamper therapies with antitumor mAbs. In vivo studies have underscored the favorable biodistribution of nanobodies, including deep penetration into tumors. Numerous nanobody-based biologics have shown antitumor efficacy in preclinical studies in vivo. Moreover, naked nanobodies can antagonize growth factor receptors and block ion channels and ecto-enzymes in the tumor microenvironment. Also, fusion of one or more nanobodies to the hinge and Fc-domains of a human immunoglobulin yields highly soluble and versatile heavy chain antibodies. Importantly, because nanobodies do not bind light chains and because they do not show any tendency to aggregate, nanobody-based bispecific hcAbs do not suffer from the VH–VL pairing problem of bispecifc conventional antibodies. Heavy chain antibodies are roughly half the size of conventional antibodies and, thus, may show better tissue penetration than conventional mAbs, while retaining the capacity to recruit the complement system, NK cells, and macrophages.
Furthermore, molecular imaging is the foundation for accurate diagnosis and pre-treatment staging of various diseases, monitoring the response to therapy and providing surveillance after therapeutic intervention. Recent advances in molecular imaging using nanobody-based probes have enhanced the possibility of high-contrast imaging of different types of tumors within much shorter time period after tracer injection, when compared to the conventional intact antibody based approaches. Nanobodies are smaller than intact antibodies and can penetrate into solid tumor tissue more efficiently, thereby representing a promising class of targeting ligands for non-invasive molecular imaging of specific targets of interest. The maturity in nanobody technology would improve our understanding of the molecular alterations in various types, subtypes and stages of cancers and other diseases, which can help the choice of suitable targeted therapeutics for each individual patient. However, although it has been more than 2 decades since nanobodies were first described, the translation of these promising imaging agents and technologies to the clinic has been very slow. Meanwhile, the development of a new diagnostic probe is an iterative process that requires substantial effort and sometimes luck. The reasons for slow clinical translation is complex and may include considerable regulatory hurdles, limited potential market, lobbying by the manufacturers of other molecular imaging probes, lack of reimbursement strategies for novel imaging agents, etc. Despite these hurdles, the exciting results obtained to date with nanobodies for molecular imaging clearly indicated that these tracers will have multifaceted applications in future clinical practices. Assuming that progress will continue at the present pace, it is likely that the future repertoire of clinicians will include an increasing battery of nanobody-based antitumor therapeutics.
Footnotes
Acknowledgments
The author is thankful to the support and assistance by the Stroke Research Chair (SATCAS) Majmaah University Almajmaah KSA.
Conflict of interest
The author declares no conflict of interest.