
Abstract
Breast cancer being the most malignant and lethal disease persistent among women globally. Immunotherapy as a new treatment modality has emerged in understanding the loopholes in the treatment of breast cancer which is mainly attributed to the potential of tumor cells to evade and survive the immune response by developing various strategies. Therefore, improved understanding of the immune evasion by cancer cells and the monoclonal antibodies against PD- and PD-L1 can help us in the diagnosis of this malignancy. Here in this article, I have highlighted that in addition to focusing on other strategies for breast cancer treatment, the involvement of immune system in breast cancer is vital for the understanding of this malignancy. Further, the complete involvement of immune system in the relapse or recurrence of the breast tumor and have also highlighted the role of vaccines, PD-1 and CTLA-4 with the recent advances in the field. Moreover, in addition to the application of immunotherapy as a sole therapy, combinations of immunotherapy with various strategies like targeting it with MEK inhibitors, Vaccines, chemotherapy and PARP inhibitor has shown to have significant benefits is also discussed in this article.
Introduction
Breast cancer persists as the most lethal cancer among women in the United States, accounting for 30% of all new cancer diagnosed and almost 41,000 annual deaths [1]. Due to the early advances in breast cancer detection and therapies, a 38% decrease in the breast cancer death rate have been observed, but almost all patients developing this metastatic disease has been shown to succumb to it. All these statistics evoke the need for the development of innovative therapeutic approaches for the treatment of breast cancer and further to reduce the recurrence and death due to this malignancy. Accumulated evidences have reported the role of immune system in breast cancer, paving the way to target the same for standard therapy and long-term survival in patients with breast cancer [2]. Various clinical studies and data have illustrated the success of targeting immune checkpoint inhibitors for the diagnosis of multiple solid tumors [3, 4]. All these sobering data have illustrated the role and significance of immune-based strategies for breast cancer treatment and prevention [5, 6].
The diagram represents the escape of tumor cells from the immune system which further results in the growth and progression of cancer.
Breast cancer has been classified into four subtypes namely: Luminal A (ER+/PR+/HER2
Once this shift happens, the immune checkpoint molecules on tumor cells and immune cells are upregulated in response to early immune activation [11], the CD4 T cell response is tilted from T helper (Th) type 1 to T helper (Th) type 2 [12] and the various immune suppressive pathways are activated in multiple immune cells [13, 14]. Therefore, all these factors generate a complex network which leads to immune suppression in the tumor microenvironment of breast tumor. Thus, signifying the role of immune system in tumorigenesis, further adding to the importance of the modulation of its cellular components as a suitable target for breast cancer diagnosis [15, 16, 17, 18, 19].
Several successes have been achieved in various cancers like melanoma, acute lymphoblastic leukemia, lung cancer by targeting certain parts of the patient’s immune system, thereby stimulating or boosting the immune system via immunotherapy. Similarly, after numerous efforts fruitful results have been achieved in breast cancer with an objective response rate of approximately 12%–19% range with PD-L1 or PD-1 monoclonal antibodies (mAb) representing the most promising strategy showing high efficacy in patients with advanced triple negative breast cancer [20, 21, 22]. In addition, cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blockades appears minimally active [23] and combinations of PD-1 and CTLA-4 are being actively studied. Furthermore, Chimeric Antigen Receptor (CAR)-engineered T cells for breast cancer diagnosis are at the earliest stages of development [24, 25] Fig. 2. Moreover, despite the soaring number of clinical trials testing immunotherapy in breast cancer, no FDA approved drugs for immunotherapies are available for breast cancer, as there are for other cancer types [26, 27, 28].
Representing the trials of immune checkpoint inhibitor in combination with various therapeutic drugs with their key effects
Representing the trials of immune checkpoint inhibitor in combination with various therapeutic drugs with their key effects
Diagrammatic representation of the interaction between tumor and CAR T cell.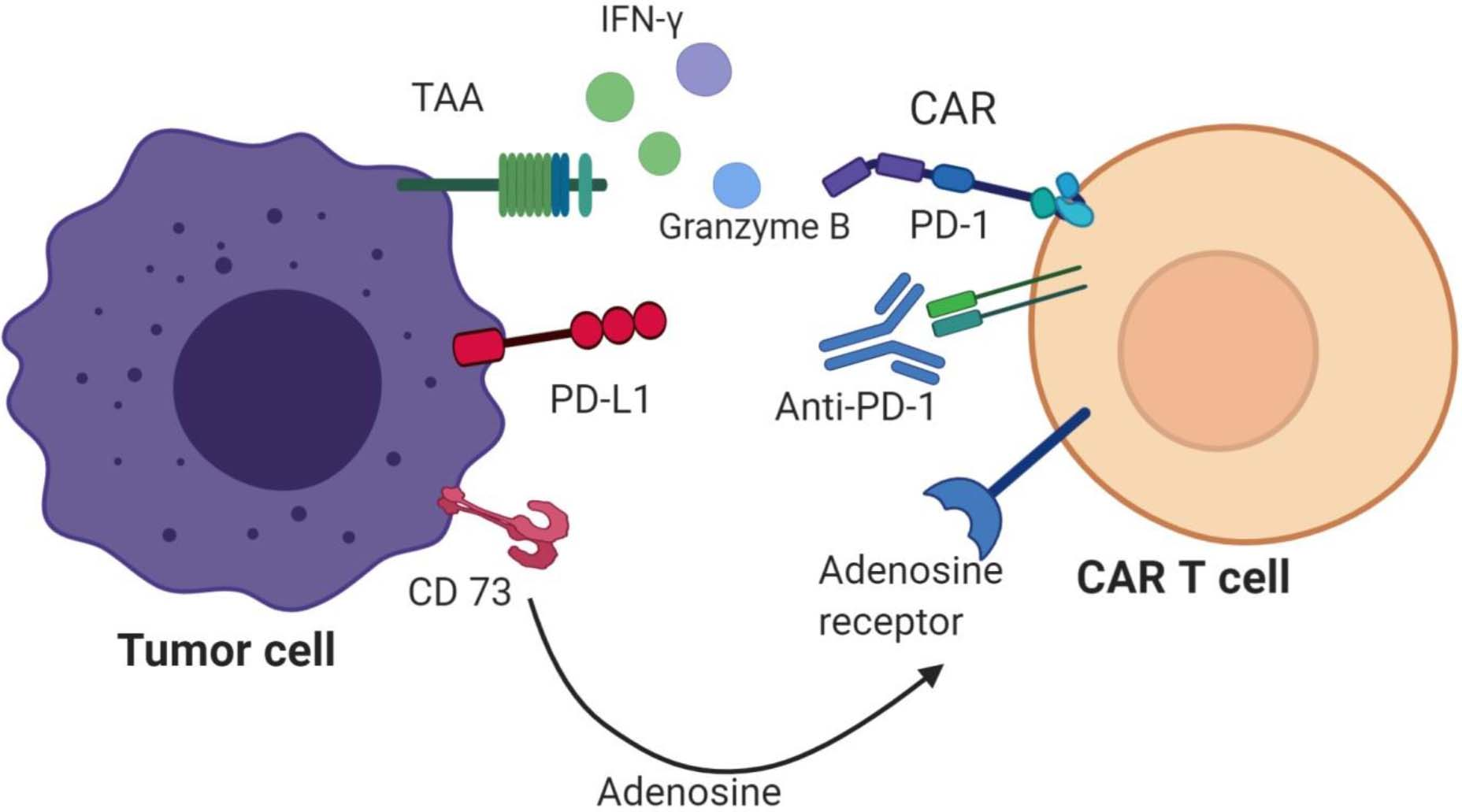
As already discussed above breast cancer is immunogenic with multiple putative tumor-associated antigens (TAAs) for instance Mucin 1 (MUC 1) and HER-2 proven to be as clinically beneficial targets for tumor-specific immune responses and development of new drug targets for cancer vaccine and bispecific antibody (bsAbs) [5, 29]. Accumulated evidences have proved that the immune cells in the tumor microenvironment can be used as a prognostic indicator of breast cancer that efficiently promote or inhibit tumor growth [30, 31]. The immune cells in the breast tumors mainly consist of T-lymphocytes and the natural killer cells, macrophages and antigen presenting cells (APCs) that are derived from B-lymphocytes [32, 33, 34]. The tumor antigens are recognized by the activated T-cells through the presentation by APCs based on the frequency of receptor-ligand interactions [35]. The breast cancer vaccines are the biological response modifiers, which contains an agent resembling the putative tumor associated antigen or any specific marker protein of tumor-causing micro-organisms, which strengthens the body’s immune system against tumor cells [5]. The development of vaccines for cancer is an active field of research, which boost the immune system in immune compromised cancer patients that utilizes an adjuvant (which may be either an immunological or pharmacological agent). This type was initiated earlier in the 1910s by Wlliam Coley who successfully used the bacterial products from Streptococcus and Serrratia for the treatment of round-cell sarcoma [6]. Breast cancer vaccines are known to induce or augment a tumor-specific response by which the immune system eliminates tumors through recognition by MHC class I and MHC class II. Nevertheless, breast cancer vaccines are mostly incorporated with shared tumor antigens to avoid autoimmunity, which are typically recognized as self by the immune system, therefore are less effective as a population of T-cells with lower avidity are generated due to the thymic selection as compared to a population of T-cells with high-avidity against tumor-specific immune response. For instance, a number of breast cancer vaccines that deliver shared tumor antigens evaluated in multiple trials have shown that despite they have proven to be safe and has been known to induce an antigen-specific immune response yet they have been shown to be correlated with no clinical benefit due to the low magnitude of T-cell response and vaccine-induced immunity. This inadequacy of shared tumor antigens is attributed to the used vaccine platforms and the advanced disease setting in which the vaccines were tested. An alternate approach to overcome this limitation is to develop the vaccines that are tumor specific mutation-specific antigens, which are having the potential to generate a high avidity T-cell response that possess the ability to significantly lyse the tumor cells presenting the neo-antigens [36]. In concordance with this, it has been seen that tumors with high mutational load are more likely to respond to immune checkpoint blockade [37, 38]. Therefore, for a more personalized approach efforts for profiling the mutational landscape are undergoing but the extent to which mutational load influences the breast tumor immunity are yet to be determined [39]. However, a major loop hole in both the personalized and generalized tumor vaccines thus far is attributed to the doings of immunecheckpoint pathways and various immune suppression mechanisms that keep in check the vaccine-induced T cells [5]. Moreover, a combination breast cancer vaccines with low-dose chemotherapy [25, 40] or full-dose chemotherapy (to trim down tumor burden and immune suppressive mechanisms in TME) have been tested in clinical trials [41]. In addition, a trial has tested a combination of peptide and cell-based vaccines, which transport trastuzumab alone to HER2 (to enhance immune memory, immune priming and effector CD8 T-cell activity) [42, 43] or low dose cyclophosphamide in order to abrogate Treg. activity [44]. Until now, the combination strategy for improving the efficacy of breast cancer vaccines have shown promising results [45]. For instance, combination of CTLA-4 or PD-1/PD-L1 with breast cancer vaccines have shown to inhibit the signaling cascades involved in the immunosuppression in the TME.
Therefore, approaches should be developed in such a way that it must boost as well as direct it towards a viable tumor target critically involved in tumorigenesis.
Recent clinical advances in breast cancer immunotherapy
The immune system can recognize a number of immunogenic targets that result from the genetic changes in tumorigenesis, the deregulated pathways that hinder the functions of adaptive immune response and the immune checkpoint inhibitors that significantly prevent autoimmunity and modulate immune response [46, 47, 48, 49, 50]. The immune checkpoint inhibitors are cell surface receptor molecules that inhibit the immune response in the TME by suppression of the activation of infiltrating T-cells. Evidences have proven the significant impact of certain inhibitory antibodies for the treatment of several cancers. For instance, bladder, breast, melanoma and non-small cell lung cancer (NSCLC) [51, 52, 53, 54]. Furthermore, several clinical trials for immune checkpoint therapies targeting PD-1, CTLA-4 or LAG-3 (lymphocyte activation gene-3) in breast cancer are still undergoing and the immune checkpoint antagonists specific for CTLA-4, PD-L1 and PD-1 have shown promising results in multiple cancers with overall beneficial survival [3, 4].
The diagram represents the interaction between cell receptors and the inhibitors in tumor progression.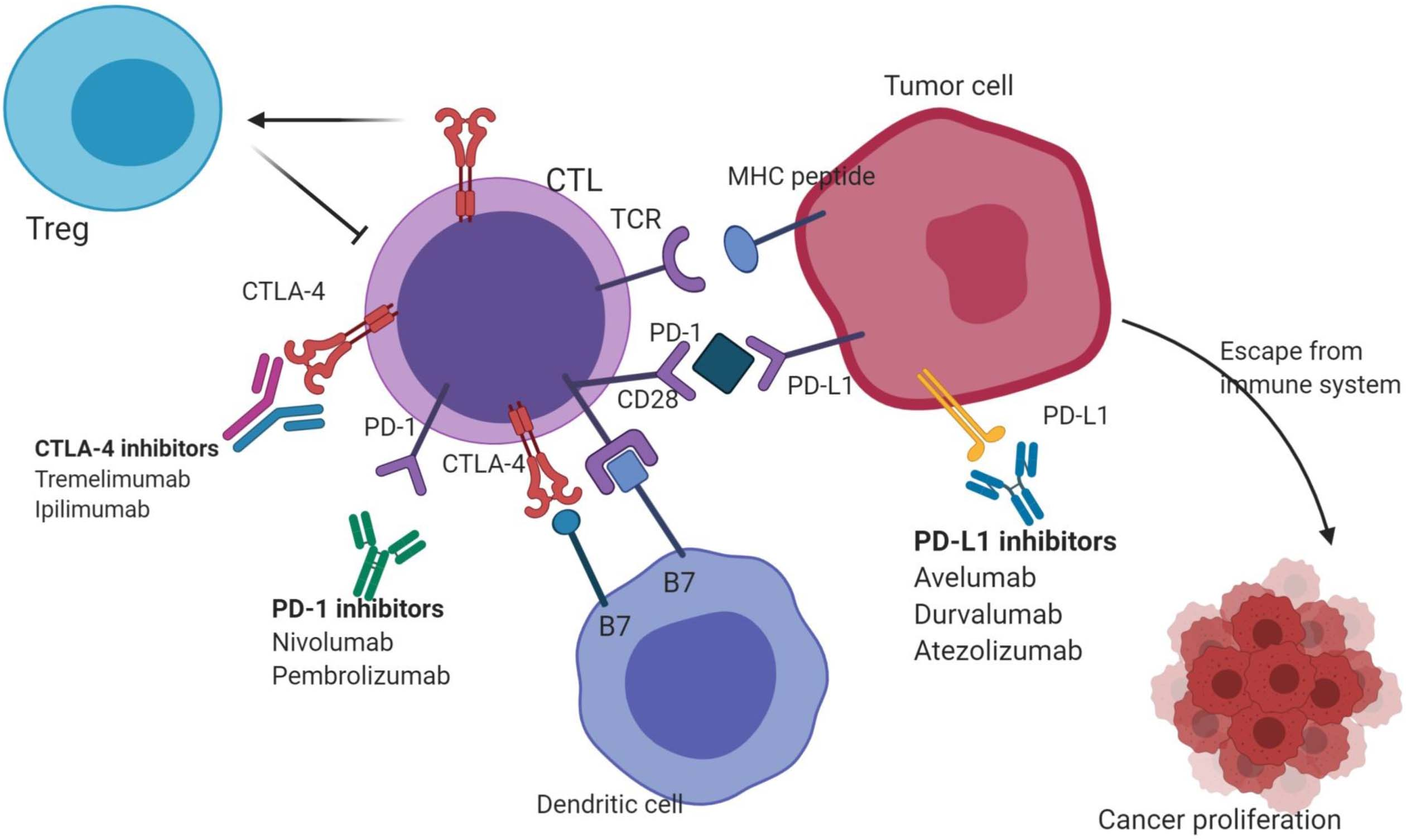
Cytotoxic T-lymphocyte antigen-4 (CTLA-4) the first immune checkpoint molecule, when inhibited shown to significantly induce anti-tumor immunity [55]. CTLA-4 acts as a homologue of CD28, which is known to bind to B7. The CTLA-4 outcompetes the binding of CD28 to B7 and prevents the T-cell activation. Therefore, after T-cell activation the upregulated CTLA-4 has been shown to interfere with the inhibition of T-cell activation and anti-tumor therapy [56].
Despite the adverse effects of CTLA-4 inhibitors related to immune system due to improved T-cell activation, it is associated with a significant objective response rate (OR). However, the mechanism may be attributed to the fact that CTLA-4 is expressed highly on regulatory T-cells, that helps in maintaining peripheral tolerance [35, 57, 58]. As for other cancers like melanoma several clinical trials for breast cancers are emerging. For instance, twenty-six hormone receptor positive patients were administered with exemestane
PD-1/PDL-1 blockade in breast cancer
The PD-1 signal pathway is considered to be an interesting therapeutic target. During the initial T-cell activation the PD-1 (Programmed Cell Death-1) is expressed highly, with the ligand partners being PD-L1 and PD-L2, for instance CD274 or B7-H1 and CD273 or B7-DC [59]. PD-1 is known to inhibit the immunological action at the reaction sites very unlikely of CTLA-4 that at the earlier step of T-cell activation inhibits the immune response [35]. PD-1 is widely expressed on a number of immune cells. PD-L1 is a potential marker in case of PD-1/PD-L1 targeted therapy, as it is widely expressed on a number of immune cells such as T-cells (CD8+ and CD4+), NK cells, B-cells and Treg. cells [60]. Interestingly, 20–30% of PD-L1 protein expression has been detected in breast cancer patients including TNBC [61, 63] and furthermore with PD-L1 mRNA expression has been detected in almost all subsets of this malignancy [62, 63]. A study relating to the clinical outcomes of PD-L1 in negative tumors has further signified the clinically beneficial role of PD-1/PD-L1 inhibitors in cancers associated with the PD-L1 expression [64]. As the PD-L1 expression is mostly limited to tumor and sites of active inflammation, it has been shown to lower the possibility of immune related disorders, which has been seen to occur in case of CTLA-4, mostly because of the down-modulation of an immune response in the effector phase [65] Fig. 3.
Nivolumab, the first anti-PD-1 antibody has shown an objective response rate of 31% and a median overall survival of 16.8 months in melanoma [66]. Therefore, has been approved for medicinal use in advanced melanoma and NSCLC. Moreover, various studies have now shown the efficacy of PD-1/PD-L1 inhibitors for the diagnosis of breast cancer [67, 68, 69]. Another anti-PD-1/PD-L1 antibody, pembrolizumab has demonstrated to be quite effective in various tumor types [3, 4]. In addition, a phase 1b study of pembrolizumab as a monotherapy in PD-L1+ TNBC has been evaluated [20, 70]. A study for evaluating the blockade of PD-1/PD-L1 in TNBC is under study. Moreover, a clinical trial for the combination of paclitaxel and pembrolizumab has estimated pCR rate of 46% versus 16% in HER-2
It is meaningful to find an effective treatment with significant therapeutic activity in the heavily recurrent/metastatic TNBC, as most of these patients had received and progressed on multiple lines of therapy for advanced disease.
Combining chemotherapy with immune-based therapy
A dual combinational strategy has the most promising therapeutic potential. The combined effect of chemotherapy and immunotherapy has proven to be influential for the diagnosis of TNBC. Based on the chemotherpy’s property to reduce the primary tumor mass plus the significant immune modulatory effects of immune based therapies on the body’s immune system. The combinatorial approach has proven to potentially promote the cytotoxic and immunological effects in a synergistic manner without any apparent additional toxicity [75]. However, depending on the drug, the timing and dose, the chemotherapy has shown to have a variable impact over the immune response in concomitance to immune-based therapy [76].
Moreover, in order to improve the overall clinical efficacy of chemo-immunotherapy, a strategy for sequential administration with different waves has proven to be beneficial in that the TME is remodeled by the first wave of immunomodulators such as kinase inhibitors for lower resistance and higher perfusion by targeting the factors associated with supportive stroma cells, reactive fibroblasts, angiogenesis and an altered ECM in the TME, followed by the second wave of chemotherapeutics shown to achieve improved tumor transmission [77]. Evidence from two small trials have revealed that two drugs namely- Nabpaclitaxel and eribulin modulate the immune system by enhancing the immune priming through antigen release and increasing the immunity through relieving immune-suppressive signals in the TME. In addition, a phase 1b study of mTNBC patients irrespective of the PD-L1 status has reported/tested the effect of atezolizumab with nab-paclitaxel [73]. In addition, a phase III study for randomized double-blind placebo-controlled for evaluating the combination of atezolizumab to nab-paclitaxel is underway as a first-line therapy for breast cancer (NCT02425891). Moreover, pembrolizumab with eribulin are being tested in an ongoing trial in patients with mTNBC of any PD-L1 status that are treated with less than or equal to two lines of chemotherapy [78]. Another KEYNOTE-355 phase III trial evaluating the combination of pembrolizumab with chemotherapy is ongoing (NCT02819518).
MEK inhibitors in combination with immunotherapy
MEK inhibitors cause the degeneration of tumors with active mutations in the Ras signaling pathway. These inhibitors have been shown to enhance the number of effector CD8+ T-cells by blocking the T-cell activation in tumor-bearing mice [79]. A combination of MEK inhibitors and PD-L1 antibody has reported in synergistic anti-tumor activity. The neoadjuvant chemotherapy treated breast cancer TNBC patients have revealed that TILs are associated with better prognosis and further the alterations in TNBC are associated with lower levels of TILs [68]. In breast cancer mouse models MEK inhibitors combined with PD-1 pathway inhibitors has revealed improvement in tumor control and tumor-specific immune response mostly by upregulating the cell surface expression of PD-L1 and MHC class I and II. Interestingly, the clinical trials for the same are ongoing.
PARP inhibition in combination with immunotherapy
PARP inhibitors are known to enhance the efficacy of conventional treatments by impairing the repair of damage caused by the agents such as radiotherapy and platinum agents. PARPi as single agents are known to induce cell death hence improve cancer therapy. However, when used in combination PARPi have shown to improve the efficacy of conventional treatments in a positive manner [80, 81, 82, 83, 84, 85]. In various animal models and breast cancer cell lines, PARP inhibitors have been reported to modulate the immune microenvironment through upregulation of PD-L1 expression [86]. In response to the antibodies that block the PD-L1 has revealed that in PARP inhibitors treated cells the sensitivity have been restored to the T-cell mediated killing. Moreover, the PARP and PD-L1 expression are shown to be inversely correlated with breast tumors. Specifically, in mouse models of breast cancers the combined treatment of PARP inhibitor and PD-L1 blockade has shown to enhance the delay of tumor outgrowth relative to their effects when applied alone. Nevertheless, studies in BRCA-deficient ovarian cancer models have shown a synergistic effect of PARP inhibitors in combination with CTLA-4 blockade [87]. In addition, the PARP inhibition or VEGF inhibition in combination with PD-L1 blockade in both ovarian and breast cancers have shown to be clinically beneficial [88].
These data support trials exploring the combination of PARP inhibitors and/or anti-angiogenic therapies on a backbone of PD-1/PD-L1 blockade in BRCA-mutated breast and ovarian cancer.
Vaccination strategies in combination with immune checkpoint blockade
Vaccines given to patients with advanced metastatic disease are known to show a modest clinical activity as a single agent or in combination with standard chemotherapy. This may be attributed to the dominant activity of immune checkpoint signaling specifically through the PD-1 pathway. Therefore, combining both the treatment options likely vaccines with immune checkpoint inhibitors may accelerate the T-cell priming and activation, while enhancing the tumor immunity response may have a greater chance of success than used alone in targeting tumors. As the basic problem associated with the vaccines is that the neo-antigens generated are recognized by the patient’s immune system as self. So, the correlation of clinical responses induced by the immune checkpoint blockade with the intrinsic immune responses specific for the neo-antigens has created in developing personalized vaccines on the basis of unique neo-antigens present in a patient’s tumor [36]. Platforms for neo-antigen based cancer vaccines include- nucleic acid based vaccines, genetically engineered viral or bacterial vaccines [5]. For the personalized vaccination strategy, a novel approach is to activate the innate immunity through the intratumoral delivery of agonists for instance through the stimulator of interferon genes (STING) pathway. The intra-tumoral delivery of STING agonist ADU-S100 induces IFN-
Conclusion and discussion
Immunotherapy is established to be the fifth treatment modality for cancer and has been an addition to the available treatment options such as chemotherapy, radiotherapy, surgery and molecularly targeted therapies. Inspite of the major advances of immunotherapy in other cancer types, immunotherapy in breast cancer is in the initial phase of its development and is just beginning to advance. Until Feb 1, 2019 no immunotherapy was approved by the FDA for breast cancer, although pembrolizumab could be used for instability high tumors for breast cancers. Despite a number of treatment options available for targeting the breast cancer, the relapse and recurrence of tumorigenesis has been posing a great challenge in the treatment of breast cancer. This recurrence and relapse has been attributed to the evasion of some tumor cells from the immune response and proliferate when the environment is feasible. Therefore, efforts have been made and further need to be strengthen to efficiently target the tumor cells and remove the chances of relapse. In addition, targeting immunotherapy with various other specific strategies like PARP inhibitors, MEK inhibitors etc. Moreover, several studies for combined immunotherapy have proven to be beneficial in several clinical trials discussed above with some more studies ongoing. Therefore, highlighting the need for further exploration of this immensly potential field.
Footnotes
Acknowledgments
The author would like to thank Deanship of Scientific Research at Majmaah University for supporting this work under project No. R-2021-123.
Conflict of interest
The author declares that he has no conflict of interest.
Funding
The study was financially supported by Deanship of Scientific Research at Majmaah University Kingdom of Saudi Arabia; vide Project Number: R-2021-123.