
Abstract
BACKGROUND:
Type 2 diabetes as the most prevalent metabolic disorder, is one of the major causes of morbidity and mortality worldwide. Recent studies suggest that body microbiota may play a role in developing metabolic disorders including type 2 diabetes. The objective of the present study was to investigate the blood microbiota composition in Iranian pre-diabetic and type 2 diabetic patients compared to healthy individuals.
METHODS:
Blood samples were taken after 12-h fasting from 90 participants, 30 healthy individuals, 30 type 2 diabetes patients and 30 pre-diabetic participants. The buffy coat layer separated by centrifugation at 800 and DNA was extracted using a column-based method. Composition and load of blood microbiota was evaluated by real-time PCR method using genus specific 16S rRNA primers.
RESULTS:
The load of Akkermansia, and Faecalibacterium was higher in normal volunteers compared to pre-diabetic and type 2 diabetes group (
The load of Bifidobacterium was higher in normal volunteers compared to type 2 diabetes patients (
In contrast, the load of Lactobacillus and Escherichia coli was higher in pre-diabetics and type 2 diabetes patients compared to normal volunteers (
The load of Bacteroides fragilis was not statistically different between studied groups but it was higher in males compared to female group (
CONCLUSION:
There is difference between microbiota composition in white blood cells of pre-diabetic and type 2 diabetes patients compared to healthy people. Determination of blood microbiota pattern may have a role in diagnosis and preventive of type 2 diabetes in a certain population. For more clarification about correlation between blood microbiota and type 2 diabetes, larger studies with more participants in different ethnical populations is suggested.
Introduction
Type 2 diabetes is a metabolic disorder with multiple predisposing factors, including age, sex, smoking, alcohol, genetics, obesity and hypertension [1, 2]. In addition to these classic risk factors, growing body of evidences indicate that other less known factors like chemicals affecting endocrine system and human microbiota may have a role in pathogenesis of type 2 diabetes [3, 4]. The prevalence of Type 2 diabetes is increasing worldwide and nowadays it considered as an epidemic situation [5]. Based on these facts, there is a need to increase our knowledge about different underlying mechanisms of type 2diabetes in order to be able to provide better prevention and treatment strategies.
The role of microbiota in human health and disease is a young science and is not fully understood.
Based on current data, human microbiota has an important role in energy and metabolism equilibrium and microbial dysbiosis may be a risk factor for the development of obesity, hypertension and type 2 diabetes [6, 7, 8]. The human Microbiota composition is affected by different factors like age, gender, diet, antibiotic consumption, ethnicity, genetic background, and life style. In other word we may mention that these different predisposing factors may be involved in intestinal microbiota imbalance and possibly cause metabolic disorders [9, 10].
According to our classic knowledge, human Blood is considered as a sterile environment. But in recent years numerous evidences have demonstrated that enteric bacterial and their products (e.g., lipopolysaccharides [LPS]) could cross the intestinal barrier due to impaired or increased permeability and enter to peripheral circulation [11, 12]. In recent years, number of interesting studies indicate the possible association between gut microbiota and type 2 diabetes [13, 14, 15, 16]. Also, small number of studies investigated the role blood microbiota in diabetic patients [17, 18].
Despite these findings there is a lack of information about the role of blood microbiota in type 2 diabetes pathogenesis and more evidence is still needed to establish this link.
The aim of the present study was to assess and compare the blood microbiota composition in three groups of type 2 diabetic patients, pre-diabetic patients and healthy individuals. We investigated the presence of genus specific 16S rRNA in peripheral blood leukocyte from Iranian studied groups using real time PCR method.
Materials and methods
Study design and population
In this case-control study, 90 individuals referred to university hospitals in Tehran, Iran in 2018 were included. The sample size was predetermined based on normal approximation using the Z statistic and the standard effect size, derived from published studies. The sample was divided into three groups. Group 1) 30 type 2 diabetes patients with A1c Hemoglobin over than 6.4%; group 2) 30 pre-diabetic patients identified with high fasting glucose (100
Participant’s age was between 40 to 60 years. The exclusion criteria were alcohol consumption, smoking, current infectious diseases, cancer, receiving antibiotics and corticosteroids within the last month, and suffering from chronic diseases (including liver cirrhosis, inflammatory bowel diseases, and chronic kidney diseases).
Written informed consents were obtained from participants. After 12 h of fasting, blood samples containing EDTA were taken from subjects. The blood samples were collected in sterile laboratory dishes containing ice and shipped to the Mycobacteriology & Pulmonary Research Department, Pasteur Institute of Iran, Tehran, Iran [13].
DNA extraction and determination of bacterial load by real-time PCR
Buffy coat layer was separated from whole blood samples. Briefly, the samples were centrifuged at 3300 g for 12 minutes and the weaving layer was gently separated and transferred to another tube. DNA from Buffy coat layer (100 microliter) was extracted using QIAamp
16S rRNA specific primers used in this study
16S rRNA specific primers used in this study
In order to quantify and determine various bacterial populations, quantitative real-time PCR was utilized. The bacterial 16SrRNA genes used in the current study were targeted by genus-specific sequences of primers. Nucleotide BLAST in NCBI was used to assess the specificity of the primers, sequences of which are presented in Table 1 [13, 14, 19, 20, 21, 22, 23, 24, 25]. PCR reactions were carried out in duplicate using Roche LightCycler
The Kolmogorov-Smirnov test was used to check the normality of data distribution. For normally distributed data, one-way analysis of variance and LSD post hoc tests were applied. For non-normally distributed data, non-parametric tests Kruskal-Wallis and Man-Whitney U Test were used. Mann-Whitney Test of SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) was used to compare the bacterial abundance in men versus women. The level of significance was set at 0.05 and less.
Results
Sex, weight, and BMI were not significantly different between studied groups (
The load of Akkermansia was higher in normal volunteers compared to pre-diabetic and type 2 diabetic patients (
Bacterial load in buffy coat samples in pre-diabetic, type 2 diabetic patients and healthy controls. Values are presented as mean 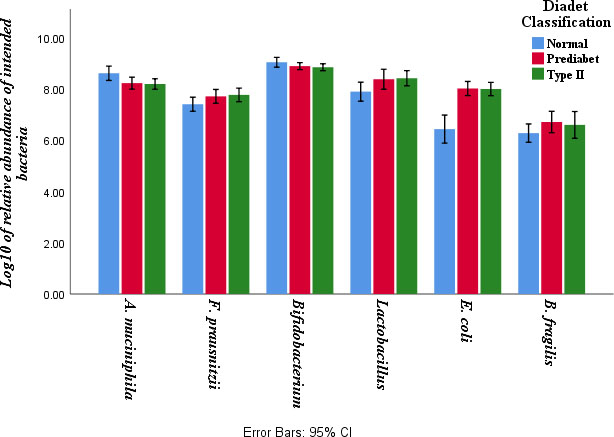
Bacterial load in buffy coat samples in male and females. Values are presented as mean 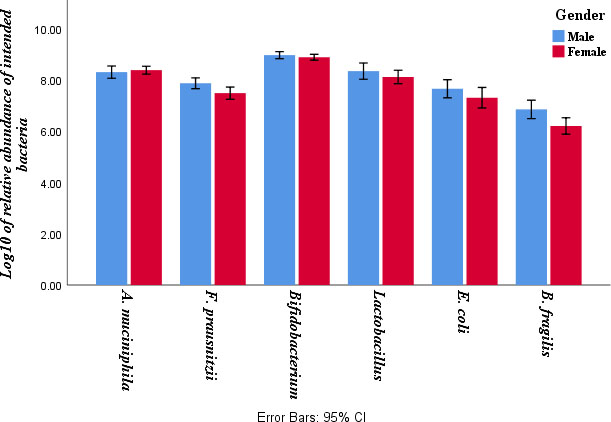
The load of Faecalibacterium was higher in normal volunteers compared to pre-diabetic and type 2 diabetic patients (
The load of Bifidobacterium was higher in normal volunteers compared to type 2 diabetic patients (
The load of Lactobacillus was higher in pre-diabetics and type 2 diabetic patients compared to normal volunteers (
The load of E. coli was higher in pre-diabetics and type 2 diabetic patients compared to normal volunteers (
The load of Bacteroides was not statistically different between studied groups (
The study further explored the difference between genders in terms of bacterial abundance. In overall, the load of Bacteroides was higher in male subjects compared to female subjects (
Human blood sterility was one of the main rules in medical sciences for decades. Historically, the presence of any microbial agents in blood was considered as a sign of infection. However, in recent years growing body of evidences suggest that we need to reconsider blood sterility and accept a normal microbiota [12, 26, 27, 28]. Although the source of blood microbiota is not completely understood, transferring bacteria from enriched environments like intestine is one of the logical possible ways. This transfer can be divided into two categories: 1 – Passive transfer trough loosening of physiological barriers and 2 – Active transfer through ingestion into leukocytes and migration through blood [26]. Previous studies confirmed the translocation of microbes and microbial components after breaking phycological barriers like oral inflammation, catheter insertion, drug injection using syringe, and even after surgeries [29, 30, 31]. The similarity between bacterial load in fecal and blood samples of studied groups in our current and previous study suggest that at least a part of source of blood microbiota in healthy volunteers and diabetic patients may be the gut [13].
Previous studies showed that tissue bacteria and their pro-inflammatory effects may be associated with diabetes [16]. Also, low-grade inflammation plays a role in the development of insulin resistance [32]. There may also be a link between stool and blood bacteria, which this needs further assessments.
In the present study, we evaluated the microbiome profile of leukocytes isolated from pre-diabetics, type 2 diabetics and healthy controls. Our results showed that the frequency of Akkermansia and Bifidobacterium was higher in healthy volunteers compared to type 2 diabetic patients. Also, the frequency of Faecalibacterium was significantly higher in healthy group than diabetic and pre-diabetic groups. In concordance with our results, Bhattacharyya and colleagues found that the peripheral blood from healthy donors contains bacterial DNA mostly from the Proteobacteria phylum, Actinobacteria phylum, Firmicutes, and Bacteroidetes phyla [12].
In our previous study we evaluated the change in gut microbiota in Iranian patients with type 2 diabetes. Briefly we found that the frequency of Akkermansia and Bifidobacterium in was higher healthy compared to type 2 diabetic patients. In contrast, the load of Lactobacillus, E. coli, and Bacteroides fragilis in type 2 diabetes groups and the load of E. coli and Bacteroides fragilis in pre-diabetes group were significantly higher than healthy group. Also, the frequency of Faecalibacterium in the healthy group was significantly greater than the other two groups [13]. Similar to mentioned studies, we confirmed that the load of E. coli was higher in pre-diabetic and diabetic groups compared than healthy volunteers. In this respect, the role of lipopolysaccharides, a major component of proteobacteria, in the onset of diabetes should take in to consideration.
In contrast to our findings about intestinal microbiota, Ejtahed et al reported that there was no significant difference between Akkermansia load in stool samples of healthy subjects and diabetic patient. They also showed that Prevotella, Escherichia, and Lactobacillus were more prevalent in faecal samples of type 1 and type 2 diabetic patients, and Bifidobacterium, Faecalibacterium, Roseburia and Bacteroides were more abundant in healthy controls [15].
In a recent study Qiu et al. found that the genus Bacteroides in the blood was negatively associated with risk of type 2 diabetes, whereas there was a positive association between the genus Sediminibacterium and type 2 diabetes [17].
Our study further explored the sexual dimorphism in blood bacterial prevalence. In general, load of Bacteroides was higher in male subjects compared to female subjects. But the load of other types of bacteria did not differ significantly between male and female. The microgenderome defines the interaction between sex hormones and microbiota and it involves bidirectional interactions between the hormones, microbiota, and disease susceptibility. In a previous cross-sectional study Mueller et al. showed that Bacteroidesa and Prevotella groups are more frequent in males than females [33]. Another study conducted by ma et al mentioned that the prevalence of five major phyla including Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, and Proteobacteria: were different between males and females [34].
Similar to mentioned studies, we confirmed that the load of E. coli was higher in pre-diabetic and diabetic groups compared than healthy volunteers. In this respect, the role of lipopolysaccharides, a major component of proteobacteria, in the onset of chronic disease like diabetes should take in to consideration. Interestingly a recent study showed an association between endotoxemia and carotid atherosclerosis [35]. Recent literature has linked gut microbiota composition with chronic diseases such as diabetes [23, 36]. A decrease in at least one of these five phylogenetically distant genera including Bacteroides, Bifidobacterium, Faecali-bacterium, and Akkermansia was found in almost half of type 2 diabetic patients and it is possible to consider them as a novel biomarker [37, 38, 39, 40].
Conclusions
The healthy blood microbiome exists and cannot be simply ignored. Reduction the load of blood bacteria like Akkermansia, Faecalibacterium, and Bifidobacterium, may be a predisposing factor for type 2 diabetes. The change in blood microbiota is probably before overt type 2 diabetes and may be started in pre-diabetes period. In addition to reduction of specific bacteria, overloading of Lactobacillus and E. coli in blood may also be a risk factor for type 2 diabetes.
Footnotes
Acknowledgments
This work was supported by the National Institute for Medical Research Development (NIMAD) (Grant number: 940604). The authors would like to thank the colleagues at Mycobacteriology and Pulmonary Research Department and Microbiology Research Center at Pasteur Institute of Iran, Tehran, Iran.
Compliance with ethical standards
Conflict of interests: The authors declare that they have no conflict of interest.
Informed consent prior to sampling: a written informed consent obtained from all participants.