
Abstract
INTRODUCTION:
Metastatic or recurrent colorectal cancer (MRCRC) has a poor prognosis. The aim of the present meta-analysis was to assess the prevalence of different subtypes of KRAS mutation and BRAF mutation in metastatic CRC patients, and evaluate the relationship between the tumor sidedness and prevalence of KRAS and BRAF mutation.
METHODS:
We searched MEDLINE/PubMed, the Cochrane Library, and ClinicalTrials.gov from January 2010 to July 2020. The data were extracted independently according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The statistical analysis was done using STATA and Meta-Disk 1.4 applications.
RESULTS:
Overall, 6699 colorectal cancer patients were included. KRAS and BRAF mutation was reported in 28% and 6% of patients, respectively. The overall prevalence of right primary and left primary metastatic CRC patients with mutated KRAS was 40% and 60%. However, the prevalence BRAF mutated right primary and left primary metastatic CRC patients was 37% and 63%. The overall HR was 2.38 for patients with metastatic CRC who had a mutated type of KRAS. Our study showed a mean overall survival of 35.4 month for KRAS mutant and a 10.12 month survival for BRAF mutant patients with metastatic colorectal cancer patients.
CONCLUSION:
The prevalence of KRAS and BRAF mutations varied significantly according to the location of the tumor. BRAF mutations are more commonly found in metastatic colorectal cancers on the right side. Liver was the most common site of metastases in patients with mutant KRAS and the mortality of patients with mutant KRAS was 2.3 times higher than the patients with wild types. These results help to better describe the population of mCRC patients and can have implications for improving and organizing anti-EGFR therapies. Further research is needed to assess differences in survival through mutation status and primary tumor location.
Introduction
Colorectal cancer (CRC) is the most common bowel cancer and one of the leading causes of cancer death worldwide [1]. Metastatic or recurrent colorectal cancer (MRCRC) has a poor prognosis. Many recent studies have shown that MRCRC with the KRAS (MT) mutant type is resistant to anti-epidermal growth factor receptors (EGFRs) such as cetuximab or panitumumab. These drugs previously used alone or in combination with cytotoxic agents in MRCRC patients with wild type (WT) genotype have shown their effect on codons 12 and 13 of the KRAS gene [3, 4, 5, 6]. Evaluation of the mutational status of the KRAS gene in primary or metastatic tumor tissues is recommended for all MRCRC patients receiving anti-EGFR chemotherapy. KRAS mutations are seen in about 40% of all CRC cases. The KRAS activating mutation stimulates the EGFR-independent RAS/MAPK signaling pathway, followed by abnormal cell growth, proliferation, and survival. However, real differences in clinical behaviors between tumors with WT and MT KRAS, except for resistance to anti-EGFR agents, remain controversial. Some reports suggested that MT KRAS tumors have a poorer prognosis than WT KRAS tumors. However, such a relationship between KRAS mutations and CRC prognosis has not been confirmed in other reports [9, 10, 11, 12, 13]. BRAF gene testing allows the identification of a subset of patients with metastatic colorectal cancer (mCRC) (i.e., those with the V600E mutation) who enjoy the relatively low benefits of standard treatments and have a very poor prognosis. BRAF-V600E-mutant mCRCs have certain clinical and pathological features: They are more common in women than men, are often on the right, have mucinous and microsatellite-instability histology (MSI-high), and spread to lymph nodes and peritoneum [17, 18, 19]. When liver metastases are severely reduced, BRAF V600E mutant tumors often recur early due to extrahepatic lesions [20, 21]. Given these considerations and the evidence in international clinical recommendations [22, 23], BRAF testing has entered clinical practice worldwide. Sanger has long been a reliable technique for detecting BRAF mutations and is still widely used in many laboratories. The part of the BRAF gene that is amplified and then sequenced also contains codons 594 and 596 mapped close to codon 600 and mutated in less than 1% of CRCs [24]. The aim of the present meta-analysis was to assess the prevalence of different subtypes of KRAS mutation and BRAF mutation in metastatic CRC patients, and evaluate the relationship between the tumor sidedness and prevalence of KRAS and BRAF mutation.
Materials and methods
This analysis aimed to evaluate the effect of KRAS/BRAF mutation status in patients with metastatic cancer (CRC) who entered retrospective and prospective studies. The initial finding showed the prevalence of these mutations in CRC patients, the second finding suggested the prevalence of KRAS mutation subtypes, and the third finding pointed to the difference in the prevalence of these mutations in right- and left-side cancers.
Dataset and research strategy
We searched MEDLINE/PubMed, the Cochrane Library, and ClinicalTrials.gov from January 2010 to July 2020. The search criteria were limited to human studies published in English. PubMed medical terms for search on PubMed were “BRAF” or “KRAS”, “Colon” or “Colorectal” or “Rectal” or “Rectum”, “Metastasis” or “Metastatic” or “metastases” or (metastasectomy), “liver”, and “lung”.
Selection criteria
To be included for review in this study, the articles had to meet the following criteria: To be performed on metastatic CRC patients who underwent complete metastasis removal surgery; have reported the results of KRAS or BRAF mutation genetic analysis from CRC sampling; the results indicating the prevalence of various mutant KRAS gene subtypes; and specifying the position of KRAS and BRAF mutations relative to the tumor site (right versus left). The selected articles included the studies published since 2010 to review the best results from recent surgical techniques. Duplicate articles or those performed on the same patient cohorts were not included in the study.
Data extraction
The data were extracted independently according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Two authors (FP and MS) selected studies according to the inclusion criteria. After this first choice, another author (MK) was consulted if necessary, to reach a joint decision. A predefined protocol was used to retrieve data from each study, including the first author name, year of publication, journal of publication, study period, sample size, research design, demographic characteristics, and KRAS/BRAF mutation status.
PRISMA flow diagram.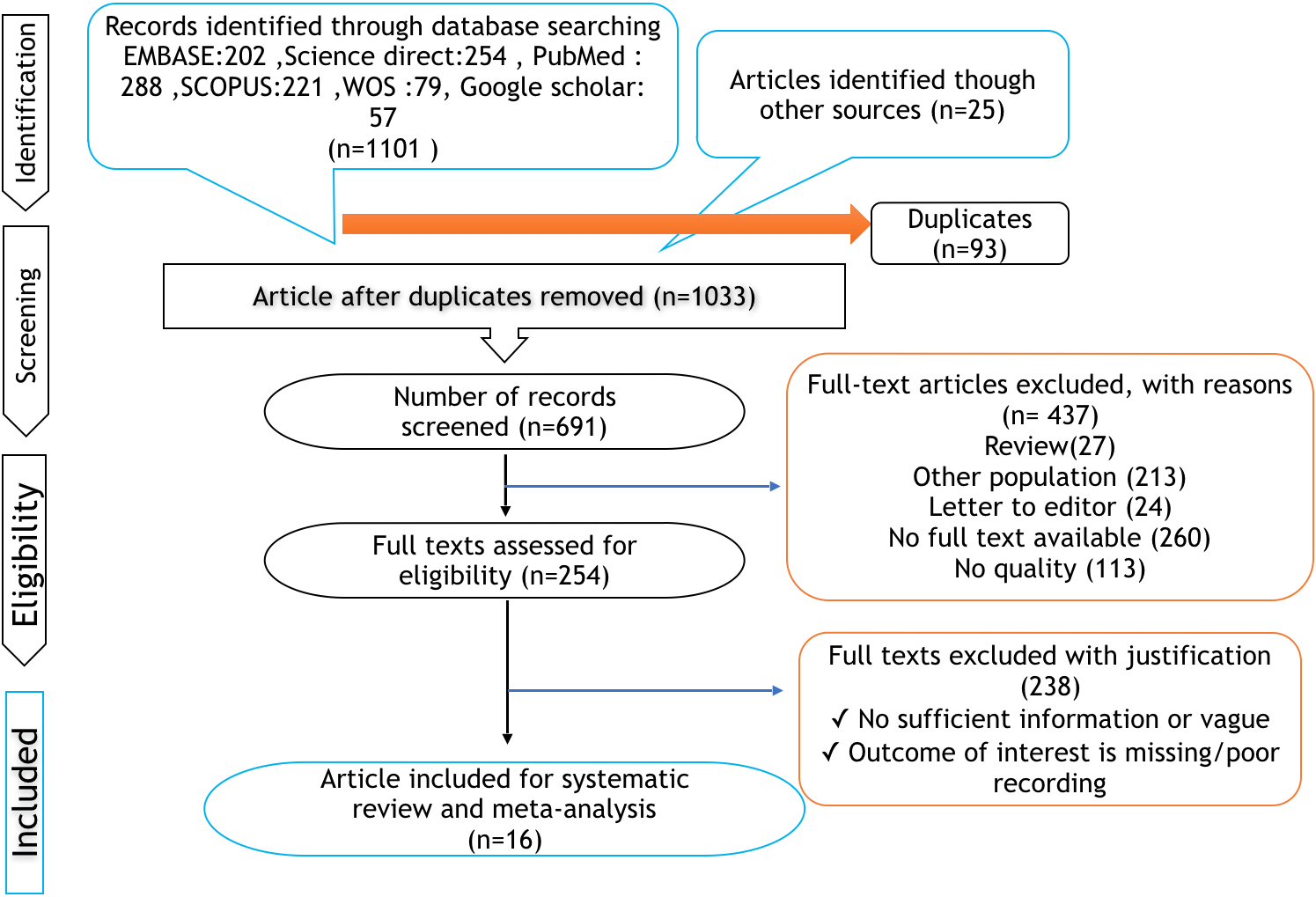
Frequency of BRAF (a), KRAS (b) mutations and its 95% interval for the studied cases according to the publication year based on the model of the random effects model. The midpoint of each section of the line estimates the % value and the length of the lines showing the 95% confidence interval in each study. The oval sign shows overall of frequency of BRAF and KRAS mutations.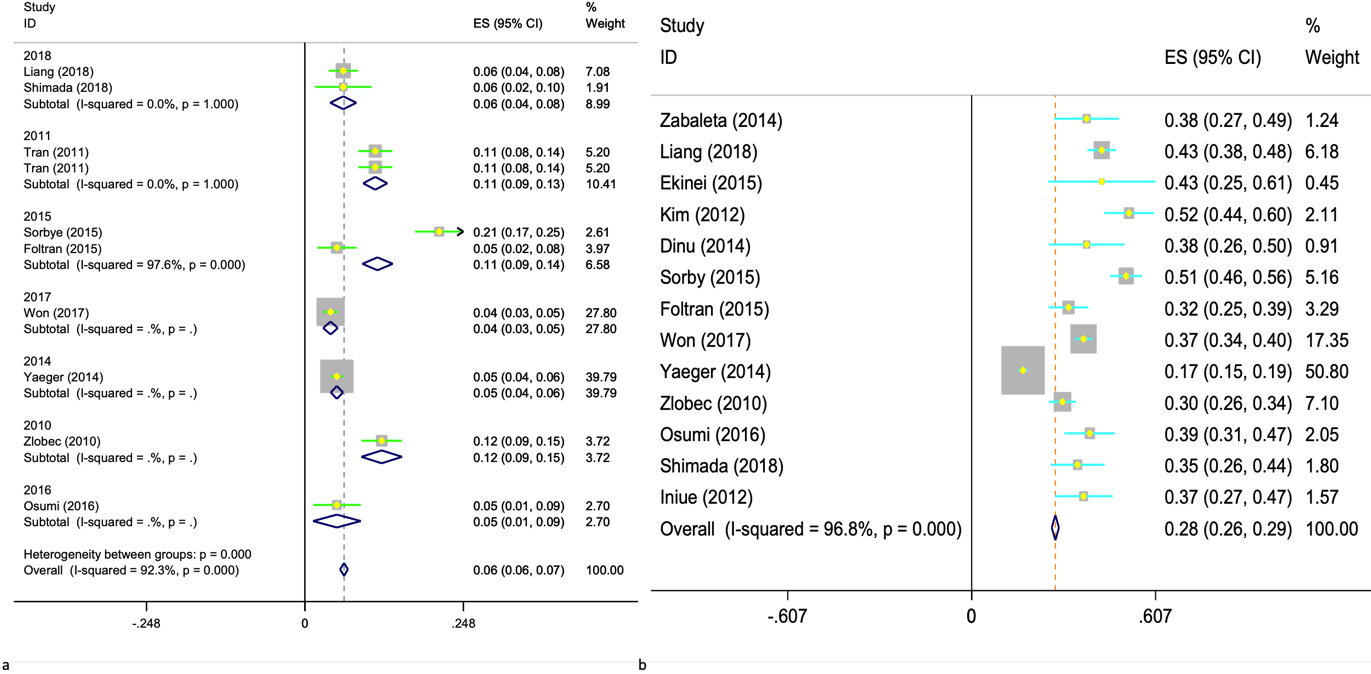
This meta-analysis was performed using the inverse-variance weighting method, in which the specific weight of each study in the dataset is calculated reciprocally with the standard square error. Heterogeneity among studies was examined using Cochran Q and I
Results
Literature search result
The electronic search provided a total of 1033 results. After screening, 30 were eliminated because they were not in English language and/or not in human; 437 were excluded because they were reviews, editorial letters, or case reports. Further, we excluded 238 articles because they included lung metastases or Liver metastases, pathways other than KRAS and BRAF, or were not focused on the effect of KRAS and BRAF mutations after metastasectomy as the main topic. At the end of the review process, 16 studies were identified as meeting the inclusion criteria of this review. These articles constitute the study population (Fig. 1). Study charac-
Demographic characteristics for the included studies
Demographic characteristics for the included studies
teristics are shown in Table 1. The Cochrane database of systematic review was then cross-checked to ensure that no similar systematic reviews had been undertaken.
Overall, 6699 colorectal cancer patients were included. KRAS mutation was reported in 28% (95% CI: 26, 29) and 6% (95% CI: 6, 7) of patients were reported to be BRAF mutated. Out of 16 included studies 5 reported prospective data and the rest of the studies were retrospective. The prevalence of KRAS mutation among metastatic CRC patients based on retrospective and prospective studies was 24.5% (95% CI: 23.9, 25.9) and 40% (95% CI: 37.3, 42.6), respectively and the corresponding rates for BRAF mutation were 4.7% (95% CI: 4, 5.4), 10.8% (95% CI: 9.5, 12) respectively. The mean follow up time ranged from 17 months to 58 month (Table 1, Fig. 2).
Meta-analysis of the prevalence of KRAS mutant right and left primary CRC
The overall prevalence of right primary metastatic CRC patients with mutated KRAS was 40% (95% CI: 35, 44) and the corresponding rate for left primary CRC was 60% (95% CI: 55, 65). However, the prevalence BRAF mutated right primary metastatic CRC patients was 37% (95% CI: 30, 43) while the corresponding rate for the left primary tumors was 63% (95% CI: 61, 66).
Meta-analysis of the prevalence of codon 12 and 13 KRAS mutations among CRC patients
Overally, KRAS mutation in codon 12 was reported in 30% (95% CI: 28, 32, I
Meta-analysis of sites of metastases in CRC patients with mutated KRAS
KRAS mutation was present in 53% (95% CI: 46, 60, I
Meta-regression finding based on the publication year and frequency of KRAS (a) and BRAF (b) mutations in metastatic colorectal cancer patients.
The overall HR was 2.38 (95% CI: 1.36, 4.61) for patients with metastatic CRC who had a mutated type of KRAS.
Meta-analysis of overall disease survival of CRC patients with mutated KRAS compared with patients with mutated BRAF
The overall survival of metastatic CRC patients with mutated KRAS and BRAF were 35.4 and 10.12 months, respectively.
Meta-analysis of the prevalence of KRAS and BRAF mutations among CRC patients coming from different countries
KRAS and BRAF mutations were present in 40% (95% CI: 37, 42), 6% (95% CI: 5.4, 7.1) of American patients and 37.1% (95% CI: 32, 42), 5.4% (95% CI: 2.6, 8.3) of Japanese patients with metastatic CRC metastasis, respectively.
Meta-regression finding based on the publication year and frequency of KRAS and BRAF mutations in metastatic CRC patients
The meta-regression findings showed an increasing process for prevalence of KRAS mutations in studies on metastatic CRC patients over time. However, the prevalence of BRAF mutation showed a decreasing pattern over time (Fig. 3).
Meta-regression finding based on the patient age and frequency of KRAS and BRAF mutations in metastatic CRC patients
The meta-regression findings showed that the prevalence of KRAS mutations increased in the older ages in studies on metastatic CRC patient’s. However, the prevalence of BRAF mutation showed a decreasing pattern by increasing the age of patients (Fig. 4).
Meta-regression finding based on the mean of age and frequency of KRAS (a) and BRAF (b) mutations in metastatic colorectal cancer patients.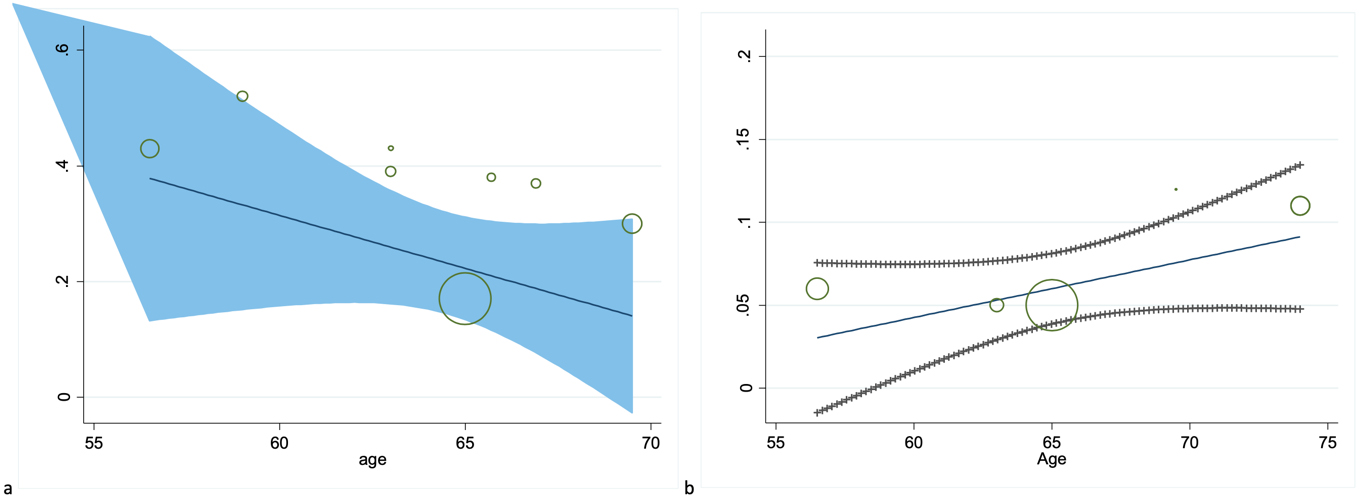
The meta-regression findings showed that the prevalence of KRAS mutations has a direct relationship with the male to female ratio while it is the opposite for BRAF mutation (Fig. 5).
Meta-regression finding based on the male to female ratio and frequency of KRAS (a) and BRAF (b) mutations in metastatic colorectal cancer patients.
Begg’s funnel plot for publication bias.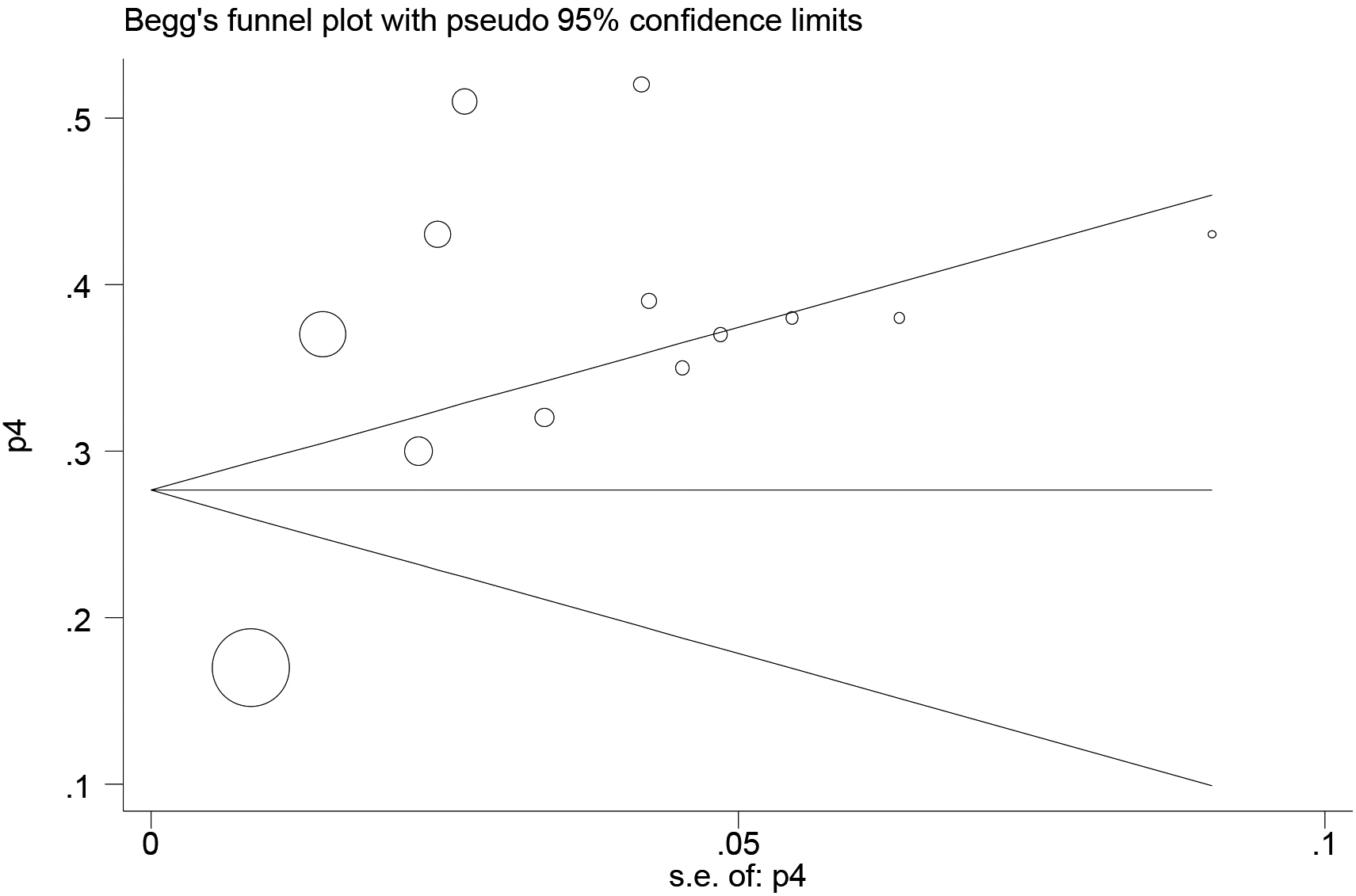
Funnel plot in Fig. 6 shows no indication of publication bias. It is shows in funnel plot symmetrically. Circles’ size shows the weight of studies (bigger circles shows more sample and smaller circles shows fewer sample).
Discussion
This systematic study and meta-analysis showed that the prevalence of mutations varied significantly according to the location of the tumor in mCRC patients, and also highlighted that the mortality of patients with mutant KRAS was 2.3 times higher than the patients with wild types. The prevalence of BRAF mutation in right colon cancer was significantly higher than left tumors. The overall prevalence of BRAF mutations in mCRC patients was 6% and the prevalence of right colon cancer with BRAF mutations was 62.6%, while the prevalence of left colon colorectal cancer with BRAF mutations was 37%. Our findings of a higher prevalence of BRAF mutations in right tumors were consistent with a recent meta-analysis that reported a significant association between right-sided colon cancer and BRAF V600E mutations (odds ratio: 4.85; 95%; CI: 3.59–6.56) [25]. Recent studies have highlighted differences in the epidemiological, clinical, and molecular characteristics of right- and left-sided CRC cancers, and they are generally considered separate diseases because right-sided tumors have a worse prognosis than left-sided tumors [26, 27]. However, in a mixed analysis of six studies, patients with right-sided tumors still had a worse prognosis than those with left-sided tumors, even compared to patients with the non-mutant mCRC subtype, indicating that the difference in the frequency of mutations by the tumor side is unlikely to be the only factor in calculating the prognostic difference between left- and right-sided tumors [27], while the National Cancer Network (NCCN) guidelines recommend anti-EGFR treatment only in non-mutated KRAS/NRAS/BRAF subtype and left mCRC and no specific treatment recommendations are provided for KRAS/NRAS/BRAF mutants or the right mCRC [28]. In their meta-analysis, Bylsma et al. showed that KRAS mutations are common in right-sided colon cancers, which, contrary to our results, implies that there is no significant difference between right- and left-sided CRCs [29]. It has been shown that metastases are present in 15% to 25% of patients at the time of diagnosis, while another 25% to 50% will involve the liver within 3 years [30, 31]. A therapeutic strategy and multidisciplinary approach to liver CRC (CRLM) metastases are essential for the further prognosis of CRC prognosis. Currently, liver resection is the only potential cure if it is technically possible. To date, the number of patients who have been candidates for liver resection has increased dramatically due to the combination of new surgical techniques with more effective treatments [32, 33]. RAS mutations may increase the chances of selecting suitable candidates for liver resection and potentially complement current clinical scores along with other prognostic features. There have been numerous reports of the prognostic significance of KRAS mutations in patients with metastatic CRC undergoing complete liver surgery. Some authors have suggested a possible negative prognostic role for RAS mutations in patients undergoing resection of colorectal cancer liver metastases [34]. The liver was found the most common site of primary metastasis in this meta-analysis. Our data showed that liver was the first metastasis site in more than half of the patients with KRAS mutants. Other metastasis sites in KRAS mutant patients were lung, brain, and peritoneum, respectively. It should be noted that mutations in the KRAS gene occur in the early stages of cancer development. Considering that the mortality of patients with mutant KRAS is 2.3 times more than the wild types. Therefore, identifying these mutations is very important for the prognosis of patients with CRC. Our study showed a mean overall survival of 35.4 month for KRAS mutant and a 10.12 month survival for BRAF mutant patients with metastatic colorectal cancer patients.
Early detection of cancer improves patients’ quality of life and survival and reduces complications and mortality. The collected data showed that KRAS mutations are mainly present in codons 12 and 13 (i.e., 95% of the total mutations: 80% in codon 12 and 15% in codon 13). Our results also showed the prevalence of 30% of mutations in codon 12 KRAS among all CRC patients based on 10 studies and 10% of KRAS mutations in codon 13 (35 and 36). In sum, mCRC patients with the possibility of having different tumors need different treatments in practice. Clinical information integrated with molecular data allows us to select better treatment options for patients and may help to classify clinical trials. Our analysis suggests that advanced CRC mutant profiles allow for a better understanding of tumor biology, and that patient classification can be performed both in clinical practice and in the design of clinical trials.
Strengths and limitations of the study
One of the strengths of this study was the selection of a wide range of studies published over the past decade on mCRC patients with tumors on both sides. Our dataset also covered the studies that explored mutation status. One of the limitations of the present study was related to different diagnostic methods reported in the initial studies that can significantly contribute to the heterogeneity of studies. Besides, significant changes in the characteristics of study subgroups including genetics, environment, diet, and lifestyle represent another limitation of our meta-analysis. However, we combined the results using a random-effect model to consider such heterogeneity.
Conclusion
The prevalence of KRAS and BRAF mutations varied significantly according to the location of the tumor. BRAF mutations are more commonly found in metastatic colorectal cancers on the right side. Liver was the most common site of metastases in patients with mutant KRAS and the mortality of patients with mutant KRAS was 2.3 times higher than the patients with wild types. Our study showed a mean overall survival of 35.4 month for KRAS mutant and a 10.12 month survival for BRAF mutant patients with metastatic colorectal cancer patients. These results help to better describe the population of mCRC patients and can have implications for improving and organizing anti-EGFR therapies. Further research is needed to assess differences in survival through mutation status and primary tumor location.