This study aimed to evaluate the prognostic value of baseline macrophage inflammatory protein (MIP)-1/IL12p40 ratio for antiviral treatment outcome in HCV genotype 4 patients.
METHODS:
Sera of 450 treatment-naïve chronic HCV patients and 50 healthy individuals were collected. Liver transaminases, total bilirubin and albumin were biochemically tested, viral RNA was quantified, and circulating MIP-1 and IL-12p40 were estimated using human anti-MIP-1 and IL-12p40 antibodies in Sandwich ELISA.
RESULTS
: No difference was observed in the baseline chemokines levels between responders and relapsers, but the later had a significantly higher MIP-1/IL-12p40 ratio ( 0.0001). Multivariate regression analysis of baseline characteristics showed that gender, age, viral load, albumin level and chemokine ratios can significantly predict treatment outcome ( 0.0114, 0.0095, 0.042, 0.0004 and 0.0001; respectively). Accordingly, a predictive threshold of baseline chemokine ratio was calculated and it showed an AUC of 0.6917 ( 0.0108; 95% CI: 0.5566 to 0.8268). The calculated threshold for predicting virologic response was 8.245, with positive and negative predictive values of 92.98% and 100%; respectively. The chemokine ratios had significant correlations with liver transaminases in treated groups whether pre or post-treatment.
CONCLUSION:
Baseline MIP-1/IL-12p40 ratio represents a non-invasive prognostic biomarker that would provide shorter treatment duration and minimizes the emergence of drug-resistant variants in HCV genotype 4-patients.
In the recent years, several direct acting antiviral drugs (DAAs) have been developed for HCV treatment, avoiding the problems of low efficacy and side effects associated with the interferon (IFN)- and ribavirin therapy and showing high cure rate especially in combination [1]. Egypt used to have the highest worldwide prevalence of viral hepatitis, with estimated rates around 4.5% to 6.7% [2]. In line with the Sustainable Development Goals adopted by the United Nations General Assembly in 2015 that included combating viral hepatitis [3], the Egyptian government led a massive screening campaign in May 2018 targeting to identify and treat all HCV-infected population with an ambitious goal to eradicate HCV by 2023 instead of 2030. According to screening results, there was 4.61% an overall HCV seroprevelance among 50 million individuals screened [4].
Failure of the FDA-approved direct-acting antiviral (DAAs) combinations is generally rare in HCV clinical or retrospective studies, with rates lower than 7% depending on baseline characteristics of study cohorts [5]. However, in real life treatment failure rate might be higher due to lower compliance particularly in hard-to-treat populations. Several predictors of the direct acting antiviral treatment outcome have been identified, including viral genotype, compensated/decompensated liver state, baseline viral load, presence of resistant-associated substitution (RASs) in viral genome; whether baseline natural substitutions or induced by previous treatments, besides the host genetic background [6]. Host immune responses also play a pivotal role in the viral clearance during therapy [7]; however, the immune mediators associated with favorable treatment outcome are not yet well characterized.
Progressive liver inflammation manifested in fibrosis, cirrhosis and ultimately carcinoma are typically concomitant with viral hepatitis C that has the ability to establish a persistent chronic infection through multiple immune evasion strategies [8]. Chemotactic proteins including cytokines and chemokines play a key role mediating the whole inflammation onset by recruiting inflammatory leukocytes and macrophages into tissues, thus shaping the immune response and influence the outcome of viral infection [9]. One of the immune-evasive viral mechanisms is modulating the expression of chemokines and accordingly disrupting the chemotaxis leading to subverting the immune response and impaired viral clearance [10].
Many studies have reported inflammatory CXC and CC chemokines to be upregulated in liver and peripheral blood cells during chronic HCV infection [11], and further acknowledged them as biomarkers for patients with liver-related diseases including fibrosis, cirrhosis, and HCC associated with viral hepatitis [12, 13]. Furthermore, serum levels of chemokines CCL4; CCL5, CCL10 and interleukins 6; 10, and 12p40 have been previously investigated for prognostic capacity and reported as strong predictive markers of HCV treatment outcome with pegylated interferon and ribavirin [14, 15]. In this study, we aimed to evaluate the potential of baseline circulating inflammatory chemokines CCL4 (MIP-1) and IL-12p40 to predict sustained virological response in chronic HCV genotype 4-Egyptian patients undergoing treatment with direct acting antiviral combinations.
Materials and methods
Ethical committee approval
This retrospective study involving human participants was approved by the Medical Ethical Committee of the National Research Centre (Approval NO: 20131) in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Patients’ sera
This study followed STARD 2015 reporting guidelines. Sera from 50 healthy individuals without any history of liver diseases and 450 chronic HCV patients were retrospectively acquired from the Medical Center of Excellence-National Research Centre, Egypt that was entitled for screening/treatment of HCV-patients during the national campaign led by the Egyptian Ministry of Health and Population in the period of 2018–2019. The diagnosis of chronic HCV was based on physical examination, biochemical testing of liver function and the presence of HCV-antibodies in sera using recombinant HCV antigen based test (Axium, USA). Positive patients were confirmed for their infection by RT-PCR and only patients who had the replicative viral genome in their sera were included in the study. Inclusion criteria included positive HCV antibodies/RNA and only sera with viral load 127,137 IU/mL were included. Exclusion criteria included non-viral hepatitis; cirrhosis/carcinoma; co-infection with HBV/HIV, uncontrolled diabetes, current/previous treatment with immune-suppressants, and previous treatment with interferon-/ribavirin combination. The treatment protocol included a daily dose of 400 mg Sofosbuvir (SOF) and 60 mg Daclatasvir (DCV) for uninterrupted twelve weeks. The end point was sustained virologic response (SVR) defined as the absence of serum HCV-RNA three months minimum of treatment cessation [14].
Biochemical and hematological assessments
Serum levels of liver transaminases, albumin and total bilirubin were estimated Bio-diagnostic kits (Biogamma, Stanbio, Germany) according to user manual. Blood count of red and white blood cells, platelets and hemoglobin were estimated by complete blood count (CBC) analysis (Eurocount Plus, Medsource Ozone Biomedicals, India).
Quantification of viral RNA in patients’ sera
Viral RNA was extracted using QIAamp Viral RNA Kit (QIAGEN GmbH, Hilden, Germany) according to user manual. Purified RNA from each sample was used as template for PCR amplification using Verso SYBR Green One-Step qRT-PCR Kit Plus ROX (ThermoFisher Scientific, USA). Reaction mixture included 5 l RNA template; 70 nM final concentration of 5’-UTR genotype 4 specific primers F: 5’-TTCACGCAGAAAGCGTCT-3’ and R: 3’-GGTGCACGGTCTACGAG-5’; 1.25 l of RT enhancer; 12.5 l of 2X One-Step qPCR SYBR Mix; 0.25 l of Verso enzyme mix, and the volume was completed to 25 l with nuclease-free water. For amplification, the cycling conditions included a single round cDNA synthesis at 55C for 15 min followed by polymerase activation cycle at 95C for 15 min and 40 cycles of denaturation at 95C for 15 sec; annealing at 55C for 30 sec and extension at 72C for 30 sec. After PCR amplification, a melting curve analysis was performed by one cycle denaturation at 95C for 3 s; one cycle starting temp at 60C for 30 sec and finally melting for 80 cycles at 60C for 10 sec with 0.5C increment/cycle. Fluorescence data were continuously collected during this heating to monitor the dissociation of the strands, and the derivative melting curves were obtained with the Rotor-Gene Q Series software 2.0.3 (QIAGEN GmbH, Hilden, Germany) [16].
Genotyping
HCV-infected sera were subjected to genotyping using Versant HCV Genotype Assay (Lipa; Bayer, Germany). Briefly, HCV RNA was extracted as aforementioned, followed by cDNA synthesis using biotinylated random primers specific for the 5’UTR of G4-HCV [17]. The generated biotinylated amplicons were hybridized to immobilized oligonucleotides probes specific for the 5’ UTR of different HCV genotypes that are bound to nitrocellulose strips by a poly (T) tail. After hybridization, unhybridized DNA was washed out from the strips that were then treated with alkaline phosphatase labeled streptavidin (conjugate) which bounds then to the biotinylated hybrid. The chromogenic substrate (BCIP/NBT) that allows the formation of a purple/brown precipitate upon degradation by alkaline phosphatase of the conjugate was used for visualization of the banding pattern on the strip.
Estimation of circulating chemokines
Serum levels of MIP-1 and IL-12p40 were estimated using MIP-1 (CCL4) Human Instant ELISA Kit (Invetrogen – ThermoFisher Scientific; USA, Cat # BMS2030INST) and IL-12 p40 Human ELISA Kit (Invetrogen – ThermoFisher Scientific; USA, Cat # KAC1561); respectively according to the manufacturer instructions.
Statistical analysis
Data were statistically analyzed using GraphPad InStat 3.0 and GraphPad Prism version 8.0.2 (GraphPad, San Diego, CA).
Demographic and clinical characteristics of the study cohort
Parameters
Healthy control
Chronic HCV-patients
-value
Total number
50
450
Gender
Male; (%)
25 (50%)
217 (48.23%)
0.05
Female; (%)
25 (50%)
233 (51.77%)
Age (Yrs)
40.13 7.11
44.02 10.28
0.05
45; (%)
24 (48%)
195 (43.33%)
45; (%)
26 (52%)
255 (56.66%)
HCV antibodies
Negative
Positive
Log viral load (IU/mL)
6.411 0.2333
8 10; (%)
–
61 (13.56%)
8 10; (%)
389 (86.44%)
Subtype
4a/m/o (; %)
–
396(88%)/31 (6.9%)/23 (5.11%)
Treatment
–
SOF/DCV
ALT (U/L)
21.5 4.4
45.12 20.16
0.0001
AST (U/L)
20.1 6.04
42.85 12.08
0.002
Total bilirubin (mg/dL)
0.65 0.311
0.73 0.45
0.05
Albumin (g/dL)
4.835 0.285
4.577 0.491
0.05
RBC’s ( 10/mm)
4.495 0.31
4.703 0.58
0.05
Hemoglobin (g/dL)
12.9 1.435
13.27 1.615
0.05
Platelets ( 10/mm)
262.4 61.82
254.7 83.83
0.05
WBC’s ( 10/mm)
6.97 3.025
6.21 1.968
0.05
Circulating chemokines (pg/mL)
MIP-1
50.12 23.7
655.2 606.3
0.0001
IL-12p40
225.52 101.48
106.7 112.5
0.0245
Numerical data are expressed as mean SD. Two-tailed values 0.05 are considered significant. Viral load 8 10 (IU/mL) is selected to be considered as low [14]. (SOF) Sofosbuvir/(DCV) Daclatasvir.
Results
Baseline demographic and clinical characteristics of the study cohort
The baseline characteristics of the study cohort are summarized in Table 1. Sera of total 500 individuals categorized as 450 chronic HCV-patients (217 male and 233 female) and 50 healthy (25 males/females) were included in this study. The mean age of healthy and infected individuals was 40.13 7.11and 44.02 10.28 years; respectively. Due to the wide age range, the study cohort was stratified into two subgroups as below and above 45 years. Based on quantitative PCR results, viral loads were also stratified into low ( 800,000 IU/mL) that was detected in 61 patients, and high load (800,000 to 10 IU/mL) detected in 389 patients. Genotyping results showed the prevalence of subtype 4a as the most common among patients (88%), with lower frequencies of G4m (6.9%) and G4o (5.11%). Serum levels of ALT and AST were significantly higher in infected patients comparing to healthy individuals ( 0.0001 and 0.002; respectively), while no significant difference in total bilirubin and albumin levels was observed. Hematological parameters in infected patients including hemoglobin, RBCs, WBCs and platelet count were statistically insignificant comparing to healthy group. Circulating levels of MIP-1 and IL-12p40 were significantly different in patients comparing to healthy control, where patients had higher levels of MIP-1 ( 0.0001) and lower levels of IL-12p40 ( 0.0245).
Correlation between MIP-1 and IL-12p40 in chronic HCV-patients before and after treatment
SVR
Relapsers
Pre-treatment
Post-treatment
Pre-treatment
Post- treatment
Pearson coefficient (r)
0.9841
0.9915
0.8235
0.9302
-value
0.0001
0.0001
0.007
0.0001
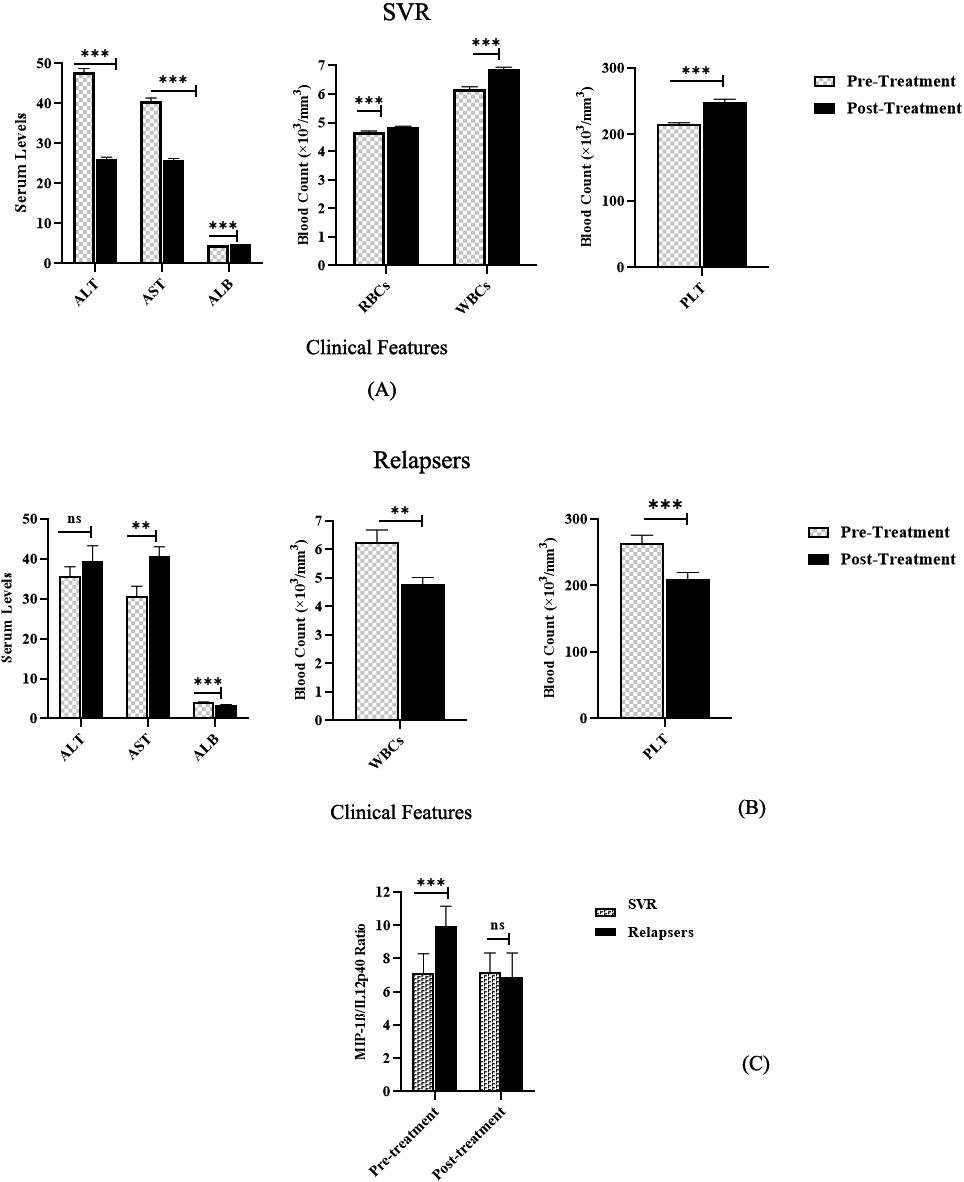
Differential efficacy of treatment in chronic HCV-patients. Responder patients had lower ALT and AST ( 0.0001 and 0.0007; respectively) and higher albumin levels ( 0.0001) and higher counts of RBCs, WBCs and platelets ( 0.0001) (1.A). Relapser patients had significantly higher AST ( 0.0478) and lower albumin levels ( 0.0001), and also lower counts of WBC ( 0.0025) and platelets ( 0.0055) after treatment failure (1.B). The calculated MIP-1/IL-12p40 ratio was significantly higher in relapsers comparing to SVR patients ( 0.0002), but no difference was found after treatment (1.C).
Multiple logistic regression analysis of baseline features predicting treatment outcome
Variable
Coefficient
SE
95% CI
t-ratio
-value
Constant
2.405
0.3209
1.760 to 3.051
7.495
0.0001
SVR ( 421)
Relapsers ( 29)
Gender
Male
200 (47.5%)
22 (73.33%)
0.1371
0.05725
0.2523 to 0.02197
2.395
0.0205
Female
221 (52.49%)
7 (26.67%)
Age (Years)
42.46 8.93
45 9.89
0.1418
0.05251
0.03621 to 0.2475
2.701
0.008
45; (%)
185 (43.94%)
10 (34.48%)
45; (%)
236 (56.05%)
19 (65.51%)
Subtype
0.03601
0.0382
0.1129 to 0.04086
0.943
0.3505
4a
288 (68.4%)
29 (100%)
4m
44 (10.45%)
–
4o
89 (21.14%)
–
Log viral load (IU/Ml)
6.52 0.49
6.854 0.175
0.08502
0.04072
0.1669 to 0.003115
2.088
0.04
ALT (U/mL)
40.33 16.7
36 8.185
0.000786
0.001129
0.003059 to 0.001486
0.6963
0.4896
AST (U/mL)
35.25 14.44
27.33 1.15
0.003272
0.002679
0.002117 to 0.008661
1.221
0.2277
Total bilirubin (mg/dL)
0.7228 0.2653
0.7 0.3
0.0834
0.07229
0.06203 to 0.2288
1.154
0.2543
Albumin (g/dL)
4.889 0.3104
4.121 0.3299
0.2127
0.05546
0.1011 to 0.3243
3.835
0.0004
Platelets ( 10/mm)
248.4 97.03
264.2 61.48
8.047E-05
0.0001879
0.0004595 to 0.0002985
0.4283
0.6706
WBC’s ( 10/mm)
6.167 1.857
6.286 2.186
0.009427
0.009919
0.02943 to 0.01058
0.9504
0.3471
RBC’s ( 10/mm)
4.848 0.53
4.544 0.5827
0.04096
0.04341
0.04659 to 0.1285
0.9436
0.3505
Hemoglobin (g/dL)
13.64 1.312
12.58 1.84
0.02161
0.0177
0.05730 to 0.01407
1.221
0.2284
MIP-1 (pg/mL)
457 405.3
393.9 88.14
0.0003432
0.0002082
7.560E-05 to 0.000762
1.648
0.1057
IL-12p40 (pg/mL)
69.36 74.54
35.97 3.28
0.002125
0.001199
0.004537 to 0.0002869
1.772
0.0826
MIP-1/IL-12p40 ratio
6.554 1.047
9.922 1.622
0.1665
0.01969
0.2061 to 0.1269
8.454
0.0001
Comparison of SVR patients’ clinical features with healthy control. Despite the viral clearance, responder patients had a significantly higher ( 0.0001) levels of ALT, AST, MIP-1 and lower levels of albumin ( 0.0001), IL-12p40 ( 0.0008), RBCs ( 0.016) and platelets count ( 0.0001) comparing to healthy individuals.
Efficacy of sofosbuvir-based treatment regimen in chronic HCV-patients
Out of 450 chronic HCV-patients, 421 (93.56%) have achieved sustained virologic response (SVR) after the completion of 12-weeks treatment protocol, while 29 patients (6.44%) were relapsers as confirmed by detection of viral RNA three months after the treatment cessation. Comparing to baseline levels, patients who achieved SVR had significantly lower ( 0.0001) serum ALT and AST, and higher levels of serum albumin ( 0.0001), with no significant difference observed in total bilirubin levels. Blood count of RBCs, WBCs and platelets was significantly higher ( 0.0001) after treatment success, but no difference was detected in hemoglobin levels (Fig. 1A). ALT, total bilirubin as well as viral RNA loads were elevated in relapsers despite the absence of statistical difference, while levels of AST and serum albumin were significantly higher ( 0.008 and 0.0001; respectively). No significant changes were observed in hemoglobin levels or RBCs count in relapser patients, but a significant reduction in WBCs and platelets’ count ( 0.0025 and 0.0055; respectively) was observed after treatment failure (Fig. 1B). Levels of circulating MIP-1 and IL-12p40 were significantly decreased in relapser patients ( 0.016, 0.0003; respectively), while a slight elevation of their mean levels was observed in SVR group without a significant difference, either when compared with pre-treatment levels or with relapsers. However, both chemokines were found to be strongly correlated in both groups, whether pre- or post-treatment (Table 2), which encouraged us to explore the possibility of calculated MIP-1/IL-12p40 ratios to clinically discriminate treated groups. Accordingly, this ratio was calculated and analyzed for variation between SVR and relapser individuals, and a significant difference of the baseline ratio has been observed, with relapser patients having a significantly higher mean ratio comparing to SVR group ( 0.0002), but no significant difference was found after treatment (Fig. 1C).
To assess the hepatic and immunological restorative effect of the treatment protocol, the clinical features of SVR group was compared to healthy control. Results showed that SVR patients had a significantly higher ( 0.0001) mean levels of ALT, AST, MIP-1 and lower levels of albumin ( 0.0001), IL-12p40 ( 0.0008) and RBCs ( 0.016) and platelets count ( 0.0001) comparing to healthy individuals (Fig. 2) despite the viral clearance, but no difference in total bilirubin, hemoglobin or WBCs count was detected.
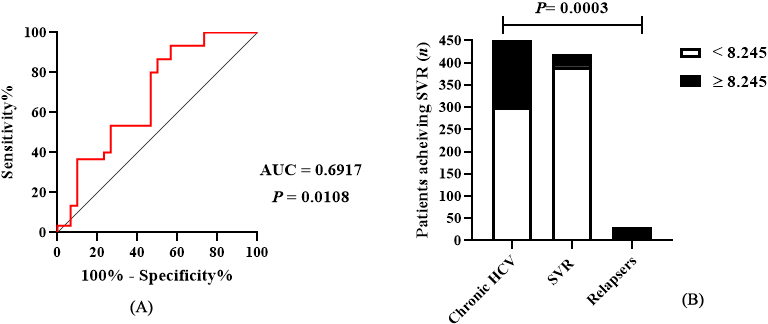
Determination of the predictive threshold of baseline MIP-1/IL-12p40 ratio. AUC value was 0.6917 ( 0.0108) (3.A), the calculated ratio for SVR prediction was 8.245 with 93.33% sensitivity and 43.33% specificity. The calculated ratio also showed a significant linear trend with strong association with treatment outcome; whether SVR or failure ( 0.0003) (3.B).
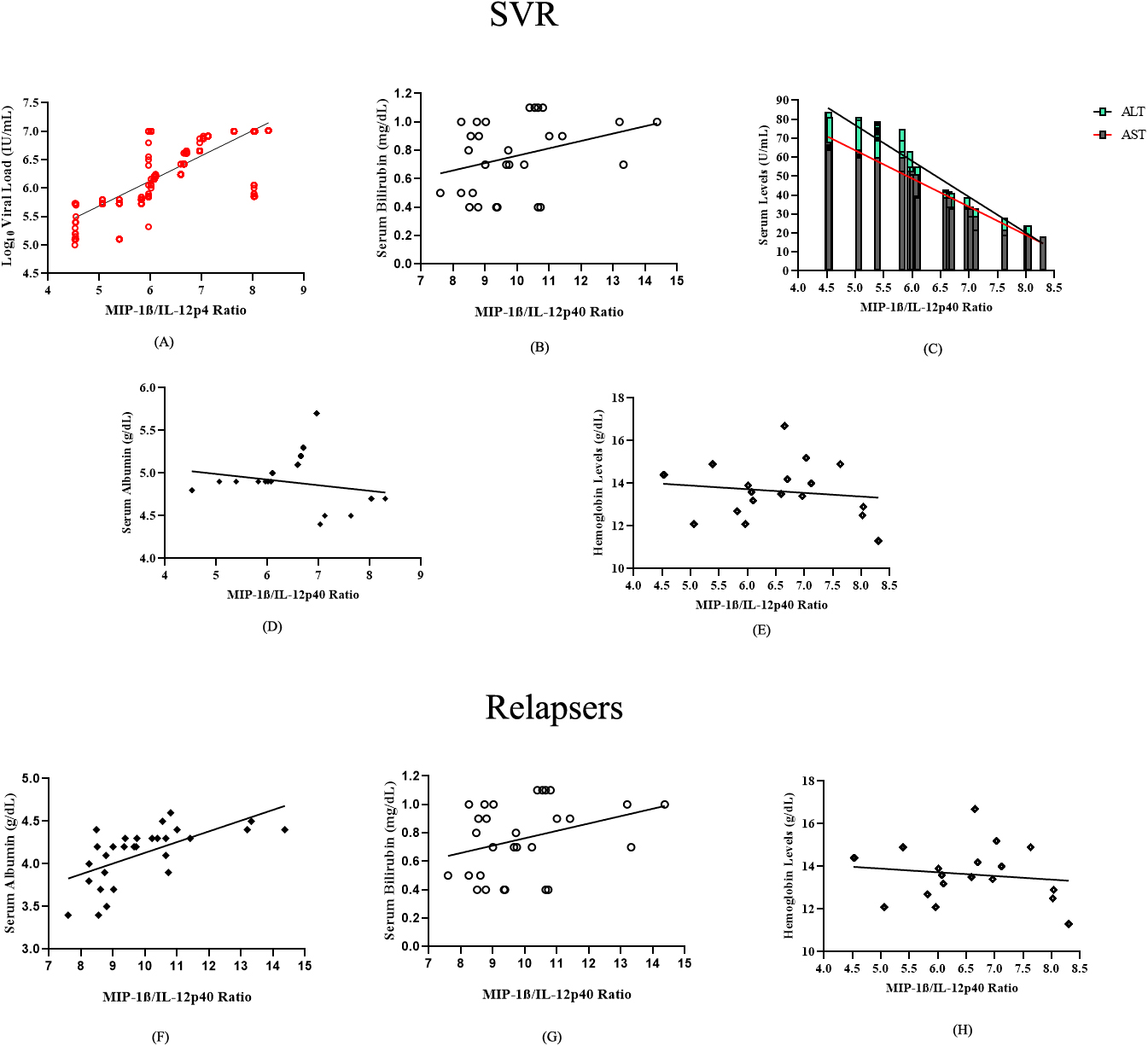
Pre-treatment correlations between chemokine ratios with clinical features. Baseline ratios were positively correlated with viral load ( 0.8128, 0.0001) (A) and WBCs count ( 0.4233, 0.0001) (B), while inversely correlated with ALT and AST (C); albumin (D) and hemoglobin levels (E) in SVR patients (0.9779, 0.0001; 0.9691, 0.0001; 0.2245, 0.0001, and 0.1378, 0.0046; respectively. In relapser patients, ratio positively correlated with albumin ( 0.6182, 0.0002) (F), total bilirubin ( 0.3292, 0.0406) and (G), and WBCs count ( 0.3498, 0.0314) (H).
Post-treatment correlations between chemokine ratios with clinical features. Chemokine ratios were found to positively correlate with ALT ( 0.35, 0.0001) and AST ( 0.2031, 0.0001) (A); albumin ( 0.1255, 0.005) (B) and WBCs count ( 0.16, 0.0005) (C) while inversely correlated with total bilirubin (0.1215, 0.0063) (D) and RBCs count (0.2405, 0.0001) (E) in SVR patients. In relapsers, the ratio inversely correlated with viral load (0.8238, 0.0001) (F) but positively correlated with serum albumin ( 0.3737, 0.0229) (G).
Baseline features predicting treatment outcome
In order to determine the baseline features that might predict the treatment outcome, a multivariate logistic regression analysis of baseline demographic and clinical features was performed. The analysis results revealed that gender, age, viral load, albumin levels and MIP-1/IL-12p40 ratio can significantly predict treatment outcome ( 0.0114, 0.008, 0.04, 0.0004 and 0.0001; respectively), where male patients; age more than 45 years; high baseline viral load and chemokine ratios, and low levels of serum albumin are more likely associated with treatment failure. Meanwhile, viral subtype, baseline levels of ALT, AST, total bilirubin, WBCs, RBCs, hemoglobin and individual chemokines had no significant effect on the treatment outcome in all patients (Table 3).
Determination of the ideal threshold for treatment outcome prediction
A receiver operating characteristic (ROC) curve was calculated to define the ideal cut-off value of chemokine ratio that might predict the final treatment outcome. AUC for SVR prediction was 0.6917 ( 0.0108) with 95% CI: 0.5566 to 0.8268. The calculated threshold for predictive baseline MIP-1/IL-12p40 ratio was 8.245 with 93.33% sensitivity (95% CI: 78.68% to 98.82%) and 43.33% specificity (95% CI: 27.38% to 60.8%), where patients with ratios 8.245 were more likely to achieve SVR than those having ratios 8.245 (Fig. 3A). Chi-square test results showed high predictive capacity of the calculated threshold ( 0.0001), with positive and negative predictive values of 93.1% (95% CI: 0.9026 to 0.9515) and 93.33% (95% CI: 0.7868 to 0.9882); respectively, with 99.49% (95% CI: 0.9816 to 0.9991) and 49.12% (95% CI: 0.3662 to 0.6174) sensitivity and specificity; respectively. The calculated ratio also showed a significant linear trend with strong association with treatment outcome; whether SVR or failure (Chi-square, df 12.83, 1; 0.0003) (Fig. 3B).
Correlation of circulating chemokine ratios with pre/post-treatment clinical features
In patients who achieved SVR, the baseline chemokine ratio was found to be positively correlated with both viral load ( 0.8128, 0.0001) (Fig 4A) and WBCs count ( 0.4233, 0.0001) (Fig. 4B), while inversely correlated with ALT and AST (0.9779, 0.0001 and 0.9691, 0.0001; respectively) (Fig. 4C). A week but significant inverse correlation was also observed between the chemokine ratio and both albumin (0.2245, 0.0001) (Fig. 4D) and hemoglobin levels (0.1378, 0.0046) (Fig. 4E). In relapser patients, pre-treatment chemokine ratio was found to have positive correlations with albumin ( 0.6182, 0.0002) (Fig. 4F), total bilirubin ( 0.3292, 0.0406) (Fig. 4G), and WBC’s count ( 0.3498, 0.0314) (Fig. 4H), but no correlation was found with viral load or liver enzymes.
Post-treatment, the chemokine ratios were found to positively correlate with liver transaminases ( 0.35, 0.0001 for ALT and 0.2031, 0.0001 for AST) (Fig. 5A); albumin levels ( 0.1255, 0.005) (Fig. 5B) and WBCs count ( 0.16, 0.0005) (Fig. 5C) while inversely correlated with total bilirubin (0.1215, 0.0063) (Fig. 5D) and RBCs count (0.2405, 0.0001) in SVR patients (Fig. 5E). In relapsers, the ratio inversely correlated with viral load (0.8238, 0.0001) (Fig. 5F) but positively correlated with serum albumin ( 0.3737, 0.0229) (Fig. 5G).
Discussion
Genotype 4 HCV has long been considered a challenging target for therapeutic approaches, given the inherent resistance associated with high variability of the viral genome under host immune-stress [18]. Despite the overwhelming rates of SVR achieved in the direct acting antiviral era; nonresponsive and relapsed patients have been recently reported in clinical trials [19]. This might be a consequence of the fact that DAA therapeutic agents were initially tailored for genotype 1 HCV; the most prevalent genotype worldwide [20]. One of the main concerns associated with DAA failure is the possibility of losing the antiviral effect of previously used DAAs with certain resistance profile when employed for re-treatment of non-responsive patients; which ultimately prompts the emergence of multi-drug resistant viral variants [21]. The risk of developing these variants does not only affect the patients prone to disease progression, but also lies in the potential transmission of these variants to other individuals which might impact the overall treatment success. Accordingly, it is best to prevent the emergence of those variants by eradicating the virus at the first treatment round using potent combinations of antivirals with non-overlapping resistance profiles, which mandates efficient prognostic markers to guide the appropriate treatment protocol.
In this domain, several chemokines have been acknowledged as predictors for interferon-based treatment outcome [14, 15, 22]; however, their role in prediction of SVR in patients on DAAs therapy has not been clearly investigated, particularly that HCV genotypes other than genotype 4 were focused in these reports. In our study, we aimed to assess the predictive value of circulating MIP-1 and IL-12p40 for the final outcome of Sofosbuvir/Daclatasvir protocol primarily adopted by the national committee for control of viral hepatitis to treat non-cirrhotic HCV-G4 patients, and address the factors associated with treatment failure. For this, sera from 50 healthy individual and 450 chronic HCV patients were retrospectively collected and assessed for liver functions tests, viral load and genotype, besides hematological parameters and circulating chemokines’ levels at the baseline and after the completion of treatment protocol.
The treatment protocol showed high efficacy where 421 patients out of 450 (93.56%) achieved SVR while only 29 patients (6.44%) were relapsers, which comes in accordance with several studies reporting the high success rates of sofosbuvir-based treatment among easy-to-treat genotype 4 HCV-patients [23, 24, 25]. Liver functions and hematological parameters were notably improved in responder patients as demonstrated by significant reduction in ALT and AST levels ( 0.0001 and 0.0007; respectively) and higher levels of serum albumin ( 0.0001), and also higher blood count of RBCs, WBCs and platelets ( 0.0001). In relapser patients, serum levels of AST and albumin were significantly higher ( 0.008 and 0.0001; respectively) after treatment failure, and similarly levels of ALT, total bilirubin as well as viral RNA loads despite the absence of statistical difference. Also, a significant reduction in WBCs and platelets’ counts ( 0.0025 and 0.0055; respectively) was observed in relapser patients, but no significant changes were observed in hemoglobin levels or RBCs counts. A significant reduction of circulating MIP-1 and IL-12p40 levels was also observed in patients who failed to achieve the virologic response ( 0.0238, 0.0428; respectively). This might be expected in instances of treatment failure typically associated with viral resistance, considering that both MIP-1 and IL-12p40 are essential for lymphocytes differentiation and priming T-helper 1 mediated response that promotes viral clearance [26].
On the other side, the post-treatment levels of liver transaminases, albumin, RBCs and platelets count as well as both chemokines did not normalize upon viral clearance and remained significantly different than normal baselines. This finding might contradict with previous studies reporting the DAAs’ restorative effect on liver functions and innate immune dysregulation generated by chronic HCV infection [27], yet supported with other studies reporting that DAA-mediated viral clearance does not completely restitute the disrupted inflammatory milieu [28]. Against this background, the post-treatment chemokine levels; particularly the pro-fibrogenic like MIP-1 [29], should be followed up in chronic HCV genotype 4 patients who achieve SVR. Of note, baseline levels of individual chemokines showed no significant difference between the treated groups; however, a strong positive correlation has been observed between pre- and post-treatment levels of MIP-1 and IL-12p40 in both groups. This observation guided us to calculate MIP-1/IL-12p40 ratio and compare the mean ratios in both groups, and a significant difference was actually found with relapser patients having a higher ratio comparing to responders ( 0.0001).
To determine the factors associated with treatment failure, the baseline demographic and clinical features were subjected to multivariate regression analysis. Results showed that the main predictors of failure included age ( 0.0095), viral load ( 0.042) and albumin level ( 0.0004), where age more than 45 years, high baseline viral load and low levels of serum albumin are more likely associated with treatment failure which agrees with the consensus findings of several studies addressing the host factors associated with DAAs response [30, 31]. Also, gender was another predictor that significantly impacts the treatment outcome ( 0.0205), where female patients had a more tendency to achieve SVR comparing to males. This finding has met conflicting results regarding this topic, where several previous studies agreed that gender has no effect on the treatment outcome [32, 33]; however, and despite the different viral genotype and genetic background of our study cohort, another study that reported higher rates of SVR among female patients; particularly in the reproductive age ( 50 years), has agreed with our findings [34]. Interestingly, the most significant predictor of the treatment outcome was the baseline chemokine ratio ( 0.0001); the lower the ratio the higher potential for the patient to respond, which complies with previous studies reporting that high levels of baseline inflammatory chemokines can be associated with DAA-induced viral clearance, and often decrease after SVR [35]. Based on this finding, a predictive threshold of pre-treatment chemokine ratio was calculated by receiver operating characteristic (ROC) curve that showed an AUC for SVR prediction of 0.6917 ( 0.0108; 95% confidence interval 0.5566 to 0.8268). The calculated threshold for predictive MIP-1/IL-12p40 ratio was 8.245 (93.33% sensitivity, 43.33% specificity), with positive and negative predictive values of 93.1% and 93.33%; respectively, and 99.49%, 49.12% sensitivity and specificity; respectively. The predictive ratio also showed a significant linear trend with strong association with treatment outcome; whether SVR or failure (Chi-square, df 12.83, 1; 0.0003).
The association between chemokines and the hepatic transaminases as a golden standard of inflammation has been a controversial topic, where some studies reported a correlation between serum/intrahepatic chemokines with liver function tests [36], while in others chemokine expression profile didn’t correlate with necroinflammation scores [37]. In our study, we investigated this hypothesis by analyzing the correlation between chemokine ratios with pre- and post-treatment clinical features. In SVR patients, the baseline ratio was found to be positively correlated with both viral load ( 0.8128, 0.0001) and WBCs count ( 0.4233, 0.0001), while inversely correlated with ALT; AST and albumin (0.9779, 0.0001; 0.9691, 0.0001; 0.2245, 0.0001; respectively). Post-treatment, the ratios positively correlated with liver transaminases ( 0.35, 0.0001 for ALT and 0.2031, 0.0001 for AST); albumin levels ( 0.1255, 0.005) and WBCs count ( 0.16, 0.0005) while inversely correlated with total bilirubin (0.1215, 0.0063). In relapsers, baseline ratio was found to have positive correlations with total bilirubin ( 0.3292, 0.0406), albumin ( 0.6182, 0.0002) and WBC’s count ( 0.3498, 0.0314), but no correlation was found with viral load or liver enzymes. After treatment failure, the ratios inversely correlated with viral load (0.8238, 0.0001) but positively correlated with serum albumin ( 0.3737, 0.0229). These findings imply that chronic HCV-patients with potent Th1 responses necessary to support virus-specific cytotoxicity have a greater chance for virologic response, and that upregulated expression of pro-inflammatory chemokines might be induced in response to viral replication rather than liver inflammation as measured by transaminases’ levels [38, 39], while in non-responsive patients the liver damage is directly associated with pro-inflammatory responses as suggested by their positive correlation with total bilirubin and albumin, and also suggests a direct viral impact on IL-12p40 levels [40].
Conclusion
The baseline ratio of circulating MIP-1/IL-12p40 has a prognostic potential that can predict sustained virological response or treatment failure in chronic HCV genotype 4-patients enrolled for Sofosbuvir/Daclatasvir treatment protocol. The proposed test represents a non-invasive biomarker that can provide shorter treatment duration and minimize the risk of drug-resistant variants emergence.
Funding
This work was not supported by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors, and most of the work was supported by personal fund.
Footnotes
Acknowledgments
The authors acknowledge the Medical Center of Excellence – National Research Centre (NRC) for providing the HCV patients’ sera used in our study, and the National Research Centre (NRC) of Egypt for providing all facilities and logistics required for the study.
Conflict of interest
The authors declare no conflict of interest concerning this work.
References
1.
WHO Global Hepatitis Report (2019), March. https://www.who.int/hepatitis/news-events/egypt-hepatitis-c-testing/en/.
2.
GomaaA.AllamN.ElsharkwayA.El KassasM. and WakedI., Hepatitis C infection in Egypt: Prevalence, impact and management strategies, Hepat Med9 (2017), 17–25. doi: 10.2147/HMER.S113681.
3.
United Nations. Resolution adopted by the General Assembly on 25 September 2015. 70/1. Transforming our world: the 2030 agenda for sustainable development (2015). http://www.naturalcapital.vn/wp-content/uploads/2017/02/UNDP-Viet-Nam.pdf.
4.
WakedI.EsmatG.ElsharkawyA.El-SerafyM.Abdel-RazekW.GhalabR. et al., Screening and treatment program to eliminate hepatitis C in Egypt, N Engl J Med382(12) (2020), 1166–1174. doi: 10.1056/nejmsr1912628.
5.
ButiM.Riveiro-BarcielaM. and EstebanR., Management of direct-acting antiviral agent failures, J Hepatol63(6) (2015), 1511–1522. doi: 10.1016/j.jhep.2015.08.010.
6.
YanZ. and WangY., Viral and host factors associated with outcomes of hepatitis C virus infection, Mol. Med. Rep15(5) (2017), 2909–2924. doi: 10.3892/mmr.2017.6351.
7.
ZhangY.GuoD.ZhaoY.ChenX.MaL.JinY. et al., The effect of cytokine profiles on the viral response to re-treatment in antiviral-experienced patients with chronic hepatitis C virus infection, Antiviral Res92 (2011), 247–254. doi: 10.1016/j.antiviral.2011.08.009.
8.
GokhaleN.S.VazquezC. and HornerS.M., Hepatitis C virus, strategies to evade antiviral responses, Fut. Virol9(12) (2014), 1061–1075. doi: 10.2217/fvl.14.89.
9.
ZeremskiM.PetrovicL.M. and TalalA.H., The role of chemokines as inflammatory mediators in chronic hepatitis C virus infection, J Viral Hepat14 (2007), 675–687. doi: 10.1111/j.1365-2893.2006.00838.x.
10.
FaheyS.DempseyE. and LongA., The role of chemokines in acute and chronic hepatitis C infection, Cell Mol Immunol11 (2014), 25–40. doi: 10.1038/cmi.2013.37.
11.
XueH.LinF.TanH.ZhuZ.Q.ZhangZ.Y. and ZhaoL., Overrepresentation of IL-10-expressing B cells suppresses cytotoxic CD4+ T cell activity in HBV-induced hepatocellular carcinoma, PLoS One11(5) (2016), e0154815. doi: 10.1371/journal.pone.0154815.
12.
JangJ.W.OhB.S.KwonJ.H.YouC.R.ChungK.W. et al., Serum interleukin-6 and C-reactive protein as a prognostic indicator in hepatocellular carcinoma, Cytokine60(3) (2012), 686–693. doi: 10.1016/j.cyto.2012.07.017.
13.
HuL.ZhuY.ZhangJ.ChenW.LiZ. et al., Potential circulating biomarkers of circulating chemokines CCL5, MIP-1β and HA as for early detection of cirrhosis related to chronic HBV (hepatitis B virus) infection, BMC Infect Dis19(1) (2019), 523. doi: 10.1186/s12879-019-4130-0.
14.
ZhangS.ZhaoY.YanH.WuH.WeiL. et al., Pretreatment serum macrophage inflammatory protein (MIP)-1 levels predict sustained virological responses to re-treatment in patients with chronic hepatitis C virus infection, Int J Infect Dis33 (2015), 15–21. doi: 10.1016/j.ijid.2014.08.021.
15.
UmemuraT.JoshitaS.YonedaS.KatsuyamaY.IchijoT. et al., Serum interleukin (IL)-10 and IL-12 levels and IL28B gene polymorphisms: Pretreatment prediction of treatment failure in chronic hepatitis C, Antivir Ther16(7) (2011), 1073–1080. doi: 10.3851/imp1869.
16.
ZaghloulH.El MorsiA.A.SowehaH.E.ElsayedA.SeifS. et al., A simple real-time polymerase chain reaction assay using SYBR green for hepatitis C virus genotyping, Arch Virol162 (2017), 57–61. doi: 10.1007/s00705-016-3059-5.
17.
YoungK.K.ArcherJ.J.YokosukaO.OmataM. and ResnickR.M., Detection of hepatitis C virus RNA by a combined reverse transcription PCR assay: Comparison with nested amplification and antibody testing, J Clin Microbial33(3) (1995), 654–657. doi: 10.1128/JCM.33.3.654-657.1995.
18.
SchnellG.TripathiR.BeyerJ.ReischT.KrishnanP. et al., Hepatitis C virus genotype 4 resistance and subtype demographic characterization of patients treated with Ombitasvir plus Paritaprevir/Ritonavir, Antimicrob Agents Chemother59 (2015), 6807–6815. doi: 10.1128/2FAAC.01229-15.
19.
MakhloufN.A.FaroukM.NafehH.M. et al., NS34A resistance-associated substitutions in chronic hepatitis C in Upper Egypt and regression of liver fibrosis after direct-acting antiviral therapy, Egypt Liver Journal11 (2021), 13. doi: 10.1186/s43066-021-00080-0.
20.
VermehrenJ.ParkJ.S.JacobsonI.M. and ZeuzemS., Challenges and perspectives of direct antivirals for the treatment of hepatitis C virus infection, J Hepatol69(5) (2018), 1178–1187. doi: 10.1016/j.jhep.2018.07.02.
21.
Abdel-HamidM.El-DalyM.MolnegrenV.El-KafrawyS.Abdel-LatifS. et al., Genetic diversity in hepatitis C virus in Egypt and possible association with hepatocellular carcinoma, J Gen Virol88(Pt 5) (2007), 1526–1531. doi: 10.1099/vir.0.82626-0.
22.
BerenguerJ.Fernandez-RodríguezA.Jimenez-SousaM.A.CosínJ.ZarateP. et al., High plasma CXCL10 levels are associated with HCV-genotype 1, and higher insulin resistance, fibrosis, and HIV viral load in HIV/HCV co-infected patients, Cytokine57 (2012), 25–29. doi: 10.1016/j.cyto.2011.10.020.
23.
AbdelatyL.N.ElnaggarA.A.SaidA.A. and HusseinR.R.S., Ledipasvir/sofosbuvir versus daclatasvir/sofosbuvir for the treatment of chronic hepatitis C genotype 4 patients, Current Drug Safety15 (2020), 53. doi: 10.2174/1574886314666191001151314.
24.
NouhM.A.Ahmed AliA.A. and El-GazzarahA.R., Study the efficacy of sofosbuvir/daclatasvir in treatment of hepatitis C virus in Egypt, Menoufia Med J33 (2020), 62–68. doi: https://www.mmj.eg.net/text.asp?2020/33/1/62/281322.
25.
CharatcharoenwitthayaP.WongpaitoonV.KomolmitP.SukeepaisarnjaroenW.TangkijvanichP. et al., Real-world effectiveness and safety of sofosbuvir and nonstructural protein 5A inhibitors for chronic hepatitis C genotype 1, 2, 3, 4, or 6: A multicentre cohort study, BMC Gastroenterol20(1) (2020), 47. doi: 10.1186/s12876-020-01196-0.
26.
HullegieS.J.ArendsJ.E.A.GroothuisminkZ.M.A.PasS.D.RijndersB.J.A. et al., Decreased pro-inflammatory immune responses during recurrent acute HCV infections in HIV co-infected patients, J Gen Virol98(6) (2017), 1294–1298. doi: 10.1099/jgv.0.000768.
27.
BurchillM.A.RobyJ.A.CrochetN.Wind-RotoloM.StoneA.E. et al., Rapid reversal of innate immune dysregulation in blood of patients and livers of humanized mice with HCV following DAA therapy, PLoS One12(10) (2017), e0186213. doi: 10.1371/journal.pone.0186213.
28.
HengstJ.FalkC.S.SchlaphoffV.DeterdingK.MannsM.P. et al., Direct-acting antiviral-induced hepatitis C virus clearance does not completely restore the altered cytokine and chemokine milieu in patients with chronic hepatitis C, J Infect Dis214(12) (2016), 1965–1974. doi: 10.1093/infdis/jiw457.
29.
HeydtmannM. and AdamsD.H., Chemokines in the immune-pathogenesis of hepatitis C infection, Hepatology (Baltimore, Md.)49(2) (2009), 676–688. doi: 10.1002/hep.22763.
30.
YanZ. and YanZ., Viral and host factors associated with outcomes of hepatitis C virus infection (review), Molecular Medicine Reports15 (2017), 2909–2924. doi: 10.3892/mmr.2017.6351.
31.
AzizH.AzizM. and GillM.L., Analysis of host and viral-related factors associated to direct acting antiviral response in hepatitis C virus patients, Viral Immunol31(3) (2018), 256–263. doi: 10.1089/vim.2017.0124.
32.
GayamV.KhalidM.MandalA.K.HussainM.R.MukhtarO. et al., Direct-acting antivirals in chronic hepatitis C genotype 4 infection in community care setting, Gastroenterol. Res11(2) (2018), 130–137. doi: 10.14740/gr999w.
33.
YangY.WuF.P.WangW.J.ShiJ.J.LiY.P. et al., Real life efficacy and safety of direct-acting antiviral therapy for treatment of patients infected with hepatitis C virus genotypes 1, 2 and 3 in northwest China, World J Gastroenterol25(44) (2019), 6551–6560. doi: 10.3748/wjg.v25.i44.6551.
34.
BelciP.ColloA.MartoranaM.EvangelistaA.GiuntiS. et al., Can gender predict virological response to standard antiviral therapy for chronic hepatitis C? A retrospective study, Hepatoma Res2 (2016), 122–130. doi: 10.20517/2394-5079.2015.53.
35.
MenezesE.G.Coelho-Dos-ReisJ.G.CardosoL.M.Lopes-RibeiroA.Jonathan-GonçalvesJ. et al., Strategies for serum chemokine/cytokine assessment as biomarkers of therapeutic response in HCV patients as a prototype to monitor immunotherapy of infectious diseases, Antiviral Res141 (2017), 19–28. doi: 10.1016/j.antiviral.2017.02.001.
36.
YamauchiK.AkbarS.M.HoriikeN.MichitakaK. and OnjiM., Increased serum levels of macrophage inflammatory protein-3alpha in chronic viral hepatitis: Prognostic importance of macrophage inflammatory protein-3alpha during interferon therapy in chronic hepatitis C, J Viral Hepat9(3) (2002), 213–220. doi: 10.1046/j.1365-2893.2002.00354.x.
37.
NischalkeH.D.NattermannJ.FischerH.P.SauerbruchT.SpenglerU. and DumoulinF.L., Semiquantitative analysis of intrahepatic CC-chemokine mRNas in chronic hepatitis C, Mediators Inflamm 1, 3(5-6) (2004), 357–359. doi: 10.1155/2FS0962935104000523.
38.
AhlenstielG.WoitasR.P.RockstrohJ. and SpenglerU., CC-chemokine receptor 5 (CCR5) in hepatitis C at the crossroads of the antiviral immune response? J Antimicrob Chemother53(6) (2004), 895–898. doi: 10.1093/jac/dkh239.
39.
HajarizadehB.LamouryF.M.FeldJ.J.AminJ.KeoshkerianE. et al., Alanine aminotransferase, HCV RNA levels and pro-inflammatory and pro-fibrogenic cytokines/chemokines during acute hepatitis C virus infection, Virol J 24, 13 (2016), 32. doi: 10.1186/2Fs12985-016-0482-x.
40.
Eisen-VanderveldeA.L.WaggonerS.N.YaoZ.Q.CaleE.M.HahnC.S. and HahnY.S., Hepatitis C virus core selectively suppresses interleukin-12 synthesis in human macrophages by interfering with AP-1 activation, J Biol Chem279(42) (2004), 43479–43486. doi: 10.1074/jbc.m407640200.