Morbidity and mortality associated with HIV infection is immune-mediated, and an understanding of HIV immunology will be beneficial in the management of HIV infection
OBJECTIVE:
The objective of this research was to measure the levels of TNF-, IL-6 and IFN- in asymptomatic HIV patients and non-HIV subjects, as well as their relationship with CD4 count.
METHOD:
Blood samples were collected from 173 subjects, consisting of 125 asymptomatic HIV patients (44 HAART-naïve and 81 on HAART) and 48 non-HIV subjects. The IFN-, IL-6, and TNF- levels in the blood were determined using enzyme-linked immunosorbent assays, and the CD4 count of all participants was determined using flow cytometry.
RESULTS:
Regardless of treatment status, the IFN- levels of non-HIV subjects were significantly higher than those of HIV patients ( 0.001). The opposite was true for IL-6, as the levels of IL-6 in non-HIV subjects were significantly lower than those in HAART-naïve HIV patients ( 0.001) and those on HAART ( 0.01). TNF- levels did not differ between HIV patients and their non-HIV counterparts. Generally, the levels of these cytokines was not affected ( 0.05) by immunosuppression (measured by CD4 count 200 cells/L) and there was no significant correlation between CD4 count and these cytokines ( 0.05).
CONCLUSION:
In conclusion, asymptomatic HIV infection decreased IFN-, increased IL-6, and had no effect on TNF- levels, regardless of treatment status. Immunosuppression had no impact on these cytokine levels, and there was no relationship between them and CD4 counts.
Infection with the human immunodeficiency virus (HIV) is one of the most serious public health issues. It was reported to have affected an estimated 37.6 million people worldwide in 2020, with 34 million of them being adults [1]. A prevalence of 1.4% among people aged 15–49 years was reported in 2018 in Nigeria with higher prevalence among females [2]. There are 3.5 million HIV-positive people in Nigeria, with 250,000 new cases and 180,000 AIDS-related deaths (UNAIDS Gap Report, 2016). Although modern combined antiretroviral therapies (also known as highly active antiretroviral therapy [HAART]) result in lower morbidity and mortality and a visible improvement of clinical and laboratory parameters in HIV-infected patients, it is known that their long-term use contributes to appearance of the many events unrelated to AIDS [4]. These morbidities (events) are usually immune-mediated and good understanding of the immunology of HIV infection and effect of HAART on this immunology will be useful in the long-term management of these patients. HIV infection is associated with inflammation [5]. Understanding the impact of immune status on inflammatory markers in HIV infection may indicate disease progression. The levels of circulating cytokine in an individual are indicative of the nature of the immune response. In addition to being essential immune system controllers, CD4 T helper (Th) cells also have a significant impact on the development of inflammatory diseases [6]. One of the crucial factors in directing CD4 T helper cells towards the appropriate response are cytokines produced by cells of the innate immune system [6]. It is important to know the levels of circulating pro-inflammatory and anti-inflammatory cytokines in HIV infected. Conflicting reports exists on the effect of HIV and/or HAART on HIV immunology and disease progression [7, 8, 9, 10]. Many studies use patients that cut across the entire clinical spectrum (WHO clinical stage I–IV) as well as not having non-HIV controls [9, 8, 10]. These introduced a lot of factors that affect the interpretation of results. Using HIV patients (irrespective of treatment status) within a particular clinical stage will remove the complexities and improve interpretation and understanding. Against this background, this study aims to determine the levels of interferon gamma, interleukin 6 and tissue necrosis factor alpha among asymptomatic HIV patients and non-HIV subjects. The effect of immunosuppression (measured by CD4 count) on these cytokines as well as relationship between these cytokines and CD4 count will also be assessed.
Materials and methods
Study population
A total of 173 subjects consisting of 125 asymptomatic HIV positive patients and 48 apparently healthy HIV seronegative individuals, were randomly recruited for this study. The HIV patients consisted of 81 patients on HAART and 44 HAART-naive patients. All HIV patients were asymptomatic out-patients attending HIV clinics in the University of Benin Teaching Hospital, Benin City, Nigeria, without signs and symptoms of any infection or diseases, and were not on any medication other than HAART (for those on HAART), while their HIV seronegative counterparts were from the surrounding community. The regimens for HAART are divided into first line, alternate first line and second line drugs. The first line and alternate first line HAART regimens are zidovudine, lamivudine and nevirapine, or combivir (consisting zidovudine, lamivudine) and liponavir/ritonavir), or combivir and efavirenz, or combivir and abacavir, or abacavir, lamivudine and nevirapine. The second line HAART regimen entails any of the following combinations: abacavir, lamivudine and liponavir/ritonavir, or zidovudine, lamivudine and liponavir/ritonavir, or stavudine, lamivudine and liponavir/ritonavir, or abacavir, lamivudine and aluvir or efavirenz, lamivudine and tenofovir, or efavirenz and ritonavir, or efavirenz, lamivudine, disoproxil fumarate. Information on duration of HAART use was also obtained. Informed consent was obtained from all participants prior to specimen collection. The Ethical Committee of Edo State Ministry of Health, Benin City, Nigeria, approved the protocol for this study.
Specimen collection and processing
Ten millilitres of blood was collected from each subject and 5 mL each was dispensed into ethylene diamine tetra-acetic acid (EDTA) container and plain container. This was mixed and labelled. The whole blood was used for CD4 estimation while the serum obtained from the clotted specimen was used for the estimation of interferon gamma (IFN-), interleukin 6 (IL-6) and tissue necrosis factor alpha (TNF-).
CD4 lymphocyte counts was evaluated using flow cytometry (Partec, Gmbh, Germany) following the manufacturer’s instruction as previously described [11]. Briefly, 20 l CD4 phycoerythrin (monoclonal) antibodies was placed into a Partec test tube and 20 l of well-mixed whole EDTA blood was added. The contents were mixed gently and incubated in the dark for 15 minutes at room temperature. This mixture was agitated during incubation every 5 minutes. Eight hundred microlitres of CD4 buffer was added to the mixture of antibody and sample and mixed gently. The counting of the cells was done by the flow cytometer.
The level of IFN- was determined using enzyme linked immunosorbent assay (ELISA) technique using the Human IFN- Picokine™ ELISA kit (Boster Biological Technology Co. Ltd, CA, USA) following the manufacturer’s instruction. Briefly, 0.1 ml of each study subject’s serum was placed inside a precoated well plate (precoated with anti-human IFN- antibody) (labelled standard). Aliquots of 0.1 ml per well of standard solutions (1000 pg/ml, 500 pg/ml, 250 pg/ml, 125 pg.ml, 62.5 pg.ml, 31.2 pg.ml and 15.6 pg/ml) of human IFN- were placed in separate wells. Into another well labelled control, 0.1 ml of sample diluent was added. This was followed by incubation at 37C for 90 mins. The contents of the wells were discarded and the plate was blotted onto paper towels. Into the wells was added 0. 1ml of biotinylated anti-human IFN- antibody and the plate was incubated at 37C for 60 mins. The wells were washed 3 times with phosphate buffered saline. This was done by adding 0.3 ml of phosphate buffer into wells and left for 2 mins. The content was discarded. This was repeated two more times and the plate was blotted onto paper towel. To all the wells was added 0.1 ml of Avidin-Biotin-Peroxidase complex solution followed by incubation at 37C for 30 mins. The wells were washed 5 times with phosphate buffered saline. Ninety microlitre of TMB substrate (colour developing agent) was added to all the wells and this was incubated in the dark for 25 mins. This was followed by the addition of 0.1 ml TMB stop solution. The absorbance (optical density) was read within 30 mins of adding the stop solution at 450 nm. The absorbance of each well was derived by subtracting the absorbance of the control well from that of each well. A graph of absorbance of the standard wells against their respective concentrations was plotted. The concentration of test IFN- was extrapolated from the standard graph.
The levels of IL-6 and TNF- were determined using enzyme linked immunosorbent assay (ELISA) technique using Human Interleukin-6 (IL-6) Picokine™ ELISA kit and Human Tissue Necrosis Factor alpha (TNF-) Picokine™ ELISA kit respectively (both from Boster Biological Technology Co. Ltd, CA, USA). The procedure for determination of the concentration of IL-6 and TNF- is the same as that for IFN- except that the wells were precoated with anti-human IL-6 antibody and anti-human TNF- antibody respectively. The manufacturer’s instruction was followed.
Statistical analysis
The data obtained were analyzed with student t-test, ANOVA and Pearson’s product moment correlation using the statistical software INSTAT (Graph Pad Inc., La Jolla, CA, USA).
Results
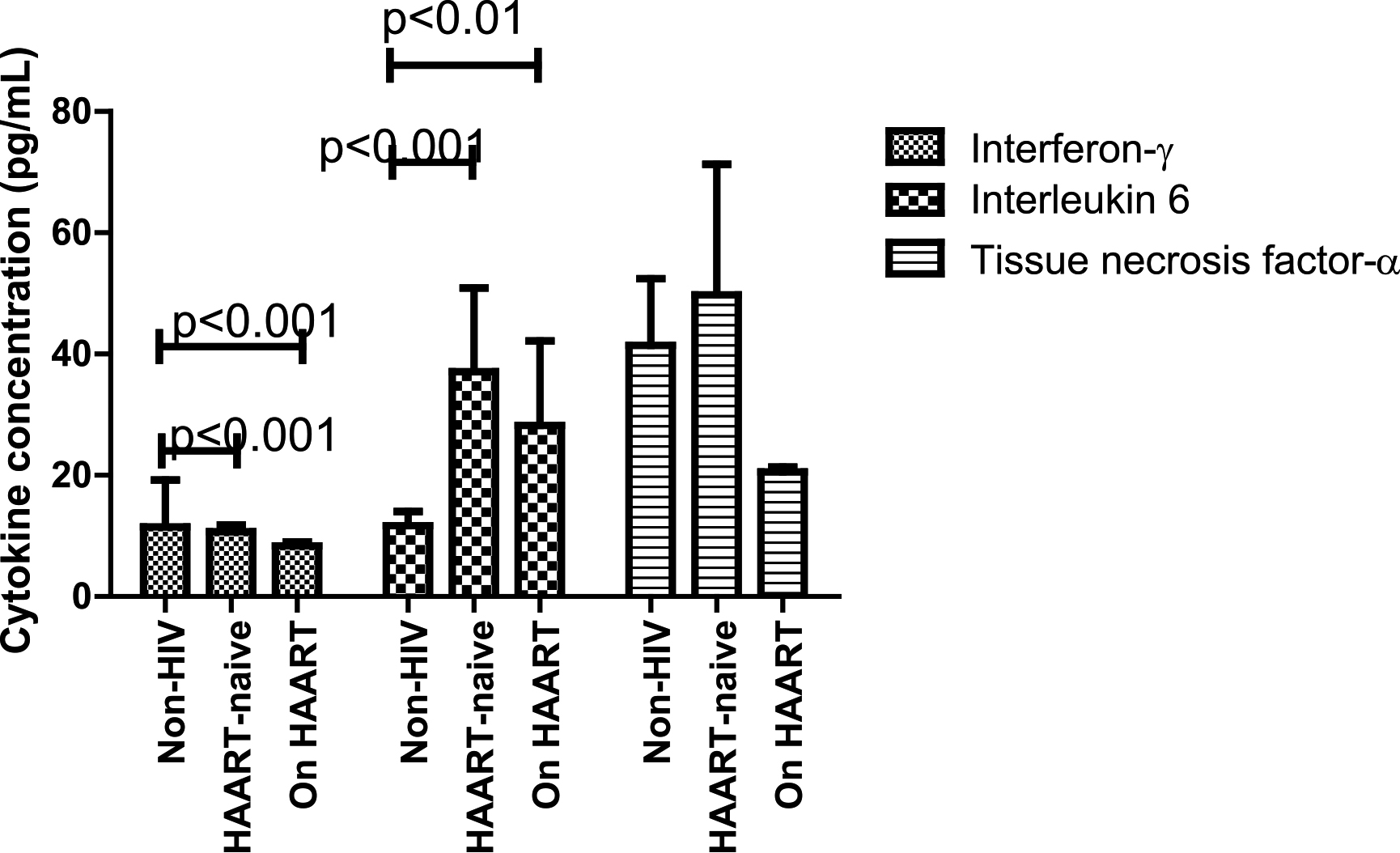
The IFN- levels of non-HIV subjects were significantly higher than those of HIV patients irrespective of treatment status ( 0.001). The reverse was the case with IL-6 as the levels of IL-6 of non-HIV subjects were significantly lower than those of HAART-naïve HIV patients ( 0.001) as well as those of HIV patients on HAART ( 0.01). TNF- levels did not differ significantly ( 0.4388) among all categories of participants (Fig. 1).
Serum levels of some cytokines in the study subjects.
Irrespective of HIV treatment status, the levels of the studied cytokines did not differ ( 0.05) among HIV patients with CD4 count 200 cells/L) and those with count 200 cells/L) with the exception of TNF- levels which was significantly higher ( 0.0040) among HAART-naïve HIV patients with CD4 count 200 cells/L (Table 1).
Effect of CD4 count on the levels of the cytokines
Parameters
CD4 count (cells/L)
value
200
200
HAART-naïve
18
26
Interferon (pg/mL)
10.19 1.91
11.02 1.41
0.7225
Interleukin 6 (pg/mL)
39.19 15.01
94.38 25.68
0.0713
Tissue necrosis factor (pg/mL)
27.39 4.30
175.45 46.57
0.0040
On HAART
6
75
Interferon (pg/mL)
10.50 1.65
8.82 0.73
0.5251
Interleukin 6 (pg/mL)
15.53 6.24
29.96 15.07
0.3794
Tissue necrosis factor (pg/mL)
19.80 2.70
22.10 1.02
0.5355
Figures are in mean standard error of the mean (SEM); number tested.
CD4 count was not significantly ( 0.05) correlated with the studied cytokines (Table 2). There was a significant negative correlation ((0.1192; 0.05) between duration of HAART use and CD4 count: type of HAART regimen did not affect the levels of IFN-, IL-6 and TNF- (data not shown).
Correlation between CD4 count and the studied cytokines
Parameters
CD4 count (cells/L)
HAART-naïve ( 44)
On HAART ( 81)
Interferon (pg/mL)
0.0908 ( 0.05)
0.1360 ( 0.05)
Interleukin 6 (pg/mL)
0.0252 ( 0.05)
0.1192 ( 0.05)
Tissue necrosis factor (pg/mL)
0.0519 ( 0.05)
0.0513 ( 0.05)
Discussion
In this study, the levels of IFN- were lower in HIV infected patients compared with non-HIV subjects. This agrees with previous reports [10, 12] but disagree with others [7, 8]. High cytokine levels correspond with symptoms of infection [13, 14]. Indeed higher levels of IFN- have been reported among HIV patients with symptoms compared to their asymptomatic counterparts [7]. The levels of IFN- during acute HIV infection in adults steadily increase and peak approximately 20–24 days post-infection [13]. In this study, the time between HIV infection and specimen collection was not determined. One may surmise that the HAART-naïve HIV patients in this study may be more than 30 days post infection and that chronic infection may have commenced. Conflicting reports on the effect of HAART on the levels of IFN- are available in the literatures. Decreasing levels of IFN- following HAART was reported by some authors [15, 16] while others reported increasing levels [8]. Other authors found minimal effect of HAART on plasma cytokines/chemokines [17]. In this study, HAART resulted in an insignificant decrease in IFN- levels compared with HAART-naïve HIV patients.
In this study, HIV patients (irrespective of treatment status) had higher levels of IL-6 compared with non-HIV subjects. This agrees with previous reports [10, 18, 19]. High levels of IL-6, which demonstrates activated or enhanced inflammation, have been associated with anaemia, cancer, cardiovascular disease and death [20, 21, 22, 23]. This may indicate that the HIV patients used in this study may be at risk of adverse clinical outcomes. Comparing IL-6 levels of HAART-naïve HIV patients and their counterparts on HAART revealed no significant difference and did not agree with previous reports [9, 10]. The difference observed in this study compared to those of Akase et al. [9] and Osuji et al. [10] may be due to the study geographical location, design and type of HIV patients used. The studies by: Akase et al. [9] was in Zaria (North West Nigeria), Osuji et al. [10] was in Nnewi (South East Nigeria) while this study was conducted in Benin City (South South Nigeria). Osuji et al. [10] study was a prospective study while this study was a cross sectional study. The HIV patients used in this study were asymptomatic (WHO clinical stage 1) while HIV patients used in Akase et al. [9] study covered the entire WHO clinical staging, that is, WHO clinical stage 1 to WHO clinical stage 4. The presence of symptoms increases plasma levels of cytokines [13]. Indeed, Akase et al. [9] found increasing levels of IL-6 with increasing WHO clinical staging. These may explain the difference in findings in this study.
Analysis of variance revealed that there was no significant difference ( 0.4388) in the serum levels of TNF- among non-HIV subjects, HAART-naïve HIV patients and HIV patients on HAART. This finding agrees with previous report [24]. Mugwe et al. [19] reported levels of TNF- among HAART-naïve HIV patients that were comparable to those of HIV patients on HAART but significantly higher than levels of non-HIV subjects. Osuji et al. [10] reported significant reduction in TNF- level following the use of HAART for up to one year. Majority of studies have demonstrated reduced TNF- levels following initiation of HAART [10, 25, 26]. This was observed in this study albeit, the difference failed to reach statistical significance. In both HIV and non-HIV subjects, the presence of symptoms of disease resulted in higher levels of TNF- [7]. This study used asymptomatic subjects, and this may explain the lack of significant difference in TNF- level among the 3 categories of participants used in this study.
It is generally accepted that CD4 lymphocyte count 200 cells/L predisposes HIV patients to opportunistic infections [27] as CD4 lymphocyte count is used as a measure of immunity and HIV disease progression [28]. In this study, irrespective of HIV treatment status, the level of the tested cytokines did not differ significantly ( 0.05) between HIV patients with CD4 count 200 cells/L and those with CD4 count 200 cells/L. IFN- levels are not associated with HIV disease progression [16]. Several theories exist as to why IFN- response does not correlate with disease progression and largely center on the poly-functional and pro-inflammatory effects of IFN- [29]. It has been suggested that cytokine expression and immunologic profiles in HIV-positive patients are more pro-inflammatory than immunoregulatory when compared to uninfected but exposed controls [30]. It is also likely that HIV infection results in modification of antigen presentation in macrophages and dendritic cell lines, resulting in anergy of HIV specific CD4 and CD8 T cells [31]. Another theory suggests that diminished response to IFN- in target populations may alter immunomodulation of Th1/Th2 response through the production of synergistic or inhibitory cytokines [29].
The finding that IL-6 values did not differ between HIV patients with CD4 count 200 cells/L and those with CD4 count 200 cells/L irrespective of their treatment status is at variance with reports that associate higher IL-6 levels with low CD4 count [7, 30]. Shive et al. [33] reported that high IL-6 results in CD4 depletion by inducing CD4 turnover without replenishing of CD4. HAART improves immunity by decreasing viral load and increasing CD4 count. However, HAART does not completely restore the immune system destroyed by HIV [16]. Indeed approximately 7.4% of the HIV patients on HAART in this study have CD4 count 200 cells/L. This may explain the finding in this study. The finding that TNF- levels did not differ significantly ( 0.05) between HIV patients with CD4 count 200 cells/L and those with CD4 count 200 cells/L of HIV patients on HAART agrees with a previous report [34].
Watanabe et al. [15] and Twizerimana et al. [35] did not find significant correlations between IFN- and CD4 count. Similarly, no correlation was found between IL-6 and CD4 count in previous reports [19, 36, 37]. These are in agreement with the finding in this study. Akase et al. [9] reported a significant inverse correlation between CD4 count and IL-6. Akase et al. [9] used HIV patients that were both symptomatic and asymptomatic (WHO clinical stage 1–4) while WHO clinical stage 1 (asymptomatic) HIV patients were used in this study, and this may explain the difference in findings. Mugwe et al. [19] reported insignificant negative correlation between TNF- and CD4 count among HIV patients irrespective of treatment status. This agrees with the finding in this study, albeit a positive correlation was observed.
In conclusion, asymptomatic HIV infection, irrespective of treatment status, resulted in lower levels of IFN-, higher levels of IL-6 and had no effect on TNF- level. The levels of these cytokines were not affected by immunosuppression and were not correlated with CD4 count.
Footnotes
Acknowledgments
The authors are immensely grateful to all the study participants for volunteering to participate in this study. All financial expenses incurred in this research was borne by authors.
Conflict of interest
The authors declare that they have no conflict of interest.
Author’s contributions
All authors were involved in conceptualization and design of the study. GAA, NLI, ROA and RO carried out sample collection and analysis. GAA, INI, NLI and RO analyzed and interpreted the data and drafted the manuscript. GAA, INI, ROA and RO contributed to reviewing and finalizing the manuscript. All Authors approved the final version of the manuscript. INI supervised the study.
References
1.
UNAIDS Global HIV & AIDS Statistics–2020 Fact Sheet. [(accessed on 17 October 2021)]. Available online: https://www.unaids.org/en/resources/fact-sheet.
2.
Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS). Nigeria HIV/AIDS Indicator and Impact Survey 2018. Available at: https://www.naiis.ng/resource/factsheet/NAIIS%20PA%20NATIONAL%20FACTSHEET%20FINAL.pdf. [Access- ed on 19 of April 2019].
3.
UNAIDS. Prevention Gap Report. Available at: https://www.unaids.org/sites/default/files/media_asset/2016-prevention-gap-report_en.pdf. 2016 Accessed on the 19 of October 2019.
4.
TascaK.L. et al., Immunovirological parameters and cytokines in HIV infection, Revista da Sociedade Brasileira de Medicina Tropical45 (2012), 663–669.
5.
KeatingaS.M. et al., The effect of HIV infection and HAART on inflammatory biomarkers in a population-based cohort of US women, AIDS25 (2011), 1823–1832.
6.
TudelaE.V.SinghM.K.LagmanM.LyJ.Nishita PatelN.OchoaC. and VenketaramanV., Cytokine levels in plasma samples of individuals with HIV infection, Austin Journal of Clinical Immunology1 (2014), 1003.
7.
NorrisP.J. et al., Elevations in IL-10, TNF-α, and IFN-γ from the earliest point of HIV type 1 Infection, AIDS Research and Human Retroviruses22 (2006), 757–762.
8.
MousaviS.A.A. et al., Plasma levels of IFN-γ, IL-4, IL-6 and IL-17 in HIV-positive patients with oral candidiasis, Jundishapur Journal of Microbiology9 (2016), e32021, doi: 105812/jjm.32021..
9.
AkaseI.E. et al., Immune dysfunction in HIV: a possible role for pro- and anti-inflammatory cytokines in HIV staging, Journal of Immunology Research.2017. Available at: doi: 10.1155/2017/4128398.
10.
OsujiF.N. et al., The effects of highly active antiretroviral therapy of the serum levels of pro-inflammatory and anti-inflammatory cytokines in HIV infected subjects, Journal of Biomedical Science25 (2018), 88. Available at: doi: 10.1186/s12929-018-0490-9.
11.
AkinboF.O. et al., Plasmodium falciparum and intestinal parasitic co-infection in HIV-infected patients in Benin City, Edo State, Nigeria, Journal of Infections in Developing Countries6 (2012), 430–435.
12.
ImamiN. et al., Assessment of type 1 and type 2 cytokines in HIV type 1-infected individuals: impact of highly active antiretroviral therapy, AIDS Research and Human Retroviruses15 (1999), 1499–1508.
13.
StaceyA.R. et al., Induction of a striking systemic cytokine cascade prior to peak viremia in acute human immunodeficiency virus type 1 infection, in contrast to more modest and delayed responses in acute hepatitis B and C virus infections, Journal of Virology83 (2009), 3719–3733.
14.
FreemanM.L., et al. Cytokines and T-cell homeostasis in HIV infection, Journal of Infectious Diseases214 (2016), 51–57.
15.
WatanabeD. et al., Sustained high levels of serum interferon-gamma during HIV-1 infection: a specific trend different from other cytokines, Viral Immunology23 (2010), 619–625.
16.
RoffS.R. et al., The significance of interferon-γ in HIV-1 pathogenesis, therapy, and prophylaxis, Frontiers in Immunology4 (2014), 498. doi: 10.3389/fimmu.2013.00498.
17.
GayC. et al., Cross-sectional detection of acute HIV Infection: timing of transmission, inflammation and antiretroviral therapy, PLoS ONE6 (2011), e19617. doi: 10.1371/journal.pone.0019617.
18.
NeuhausJ. et al., Markers of inflammation, coagulation and renal function are elevated in adults with HIV infection, Journal of Infectious Diseases201 (2010), 1788–1795.
19.
MugweJ.N. et al., Relationship between plasma cytokine levels and CD4 T cell counts during acute HIV infection among HIV/AIDS patients attending Nakuru Provincial General Hospital, Kenya, European Journal of Research in Medical Sciences4 (2016), 44–51.
20.
KullerL.H. et al., Inflammatory and coagulation biomarkers and mortality in patients with HIV infection, PLoS Medicine5 (2008), e203.
21.
DuprezD.A. et al., Inflammation, coagulation and cardiovascular disease in HIV-infected individuals, PLoS One7 (2012), e44454.
22.
BorgesA.H. et al., Predicting risk of cancer during HIV infection: the role of inflammatory and coagulation biomarkers, AIDS27 (2013), 1433–1441.
23.
BorgesA.H. et al., Markers of inflammation and activation of coagulation are associated with anaemia in antiretroviral treated HIV disease, AIDS28 (2014), 1791–1796.
24.
GoriE. et al., Inflammation-modulating cytokine profile and lipid interaction in HIV-related risk factors for cardiovascular diseases, Therapeutics and Clinical Risk Management12 (2016), 1659–1666.
25.
HaissmanJ.M. et al., Plasma cytokine levels in Tanzanian HIV-1-infected adults and the effect of antiretroviral treatment, Journal of Acquired Immune Deficiency Syndrome52 (2009), 493–497.
26.
SachdevaR.K. et al., Effect of nonnucleoside reverse transcriptase inhibitors on cytokine, chemokine, and immunoglobulin profiles in serum and genital secretions of HIV-infected women, Journal of Interferon and Cytokine Research30 (2010), 299–310.
27.
OguntibejuO.O. et al., Effect of liquid nutritional supplement on viral load and haematological parameters in HIV-positive/AIDS patients, British Journal of Biomedical Science63 (2006), 134–139.
28.
GoselleO.N. et al., Malaria infection in HIV/AIDS patients and its correlation with packed cell volume (PCV), Journal of Vector Borne Diseases46 (2009), 205–211.
29.
LiebermanJ., Tracking the killers: how should we measure CD8 T cells in HIV infection? AIDS18 (2004), 1489–1493.
30.
NaranbhaiV. et al., Innate immune activation enhances HIV acquisition in women, diminishing the effectiveness of tenofovir microbicide gel, Journal of Infectious Diseases206 (2012), 993–1001.
31.
LiebermanJ. et al., Dressed to kill? A review of why antiviral CD8 T lymphocytes fail to prevent progressive immunodeficiency in HIV-1infection, Blood98 (2001), 1667–1677.
32.
ArmahK.A. et al., HIV status, burden of comorbid disease, and biomarkers of inflammation, altered coagulation, and monocyte activation, Clinical Infectious Diseases55 (2012), 126–136.
33.
ShiveC.L. et al., Inflammatory cytokines drive CD4+ T cell cycling and impaired responsiveness to interleukin 7: implications for immune failure in HIV disease, Journal of Infectious Diseases210 (2014), 619–629.
34.
BenjaminR. et al., Discordance in CD4+T-cell levels and viral loads with co-occurrence of elevated peripheral TNF-α and IL-4 in newly diagnosed HIV-TB co-infected cases, PLoS ONE8 (2013), e70250. doi: 10.1371/journal.pone.0070250.
35.
TwizerimanaA.P. et al., Immunological profiles in HIV positive patients following HAART initiation in Kigali, Rwanda, East African Medical Journal91 (2014), 261–266.
36.
BorgesA.H. et al., Factors associated with plasma IL-6 levels during HIV infection, Journal of Infectious Diseases212 (2015), 585–595.
37.
NhhomaP. et al., Raised interleukin 6 levels: a risk factor for cardiovascular associated complications in HIV positive Zambians before initiation of antiretroviral therapy, Medical Journal of Zambia44 (2017), 69–74.