
Abstract
BACKGROUND:
One of the most severe side effects of solid-organ transplantation is posttransplant lymphoproliferative disease (PTLD). People with human immunodeficiency virus infection (HIV), an immunosuppressive disease comparable to HIV, have a higher chance of developing lymphoma when their peripheral blood contains elevated levels of the immunoglobulins kappa and lambda free light chains (FLCs).
METHODS:
This systematic review’s objective was to monitor associated B lymphoma cells in PTLD patients. In order to find relevant studies published between 1/1/2000 and 1/9/2022, two independent researchers conducted searches (MT, AJ). A literature search of English language publications was conducted using MEDLINE through PubMed, EMBASETM through Ovid, the Cochrane Library, and Trip. In addition to Magiran and SID, we searched KoreaMed and LILACS for literature published in other languages. sFLC or PTLD, transplant, or Electrophoresis are terms used in the search strategy.
RESULTS:
A total of 174 studies were selected. After analyzing their correspondence with the required criteria, a final review of five studies was conducted. The manuscript presents current findings on the potential benefits of the clinical applicability of sFLCs in PTLD. While the preliminary results appear promising, the only consistent result is that early-onset PTLD is predicted within the first two years after transplant, a biomarker that could be used to diagnose the condition.
CONCLUSIONS:
Therefore, PTLD has been predicted by using the sFLCs. There have been contradictory results to date. Future research could include assessing the quantity of sFLCs and their quality in transplant recipients. In addition to PTLD and complications after transplantation, sFLCs may provide insight into other diseases. To confirm the validity of sFLCs, more studies are needed.
Background
Post-transplant lymphoproliferative disorder (PTLD) is a severe complication of solid organ and hematopoietic stem cell transplantation (HSCT) that arises due to the impaired immune system of transplant recipients [1]. PTLD is a diverse group of lymphoid and plasmacytic neoplasms that vary in histological and clinical features. The incidence of PTLD varies depending on the type of transplantation and the recipient’s age, with a reported incidence ranging from 1% to 20% [2, 3]. PTLD is a challenging disease to manage due to its varied presentation and potential for rapid progression. Early diagnosis and management of PTLD are crucial for successful treatment, but this can be challenging due to the wide range of clinical presentations and the lack of specific diagnostic markers [4, 5]. Currently, PTLD diagnosis relies on a combination of clinical features, imaging studies, histopathology, and molecular analyses. PTLD may present as a localized or systemic disease, with symptoms ranging from fever and malaise to organ failure [6]. The diagnosis of PTLD is primarily based on histological analysis of tissue biopsies, which can be challenging to obtain due to the risks associated with invasive procedures in immunocompromised patients. However, several serum biomarkers have shown potential as diagnostic tools for PTLD, including soluble CD30 (sCD30), immunoglobulin-free light chains (sFLCs), and Epstein-Barr virus (EBV) DNA [6, 7]. These biomarkers may aid in the early diagnosis and monitoring of PTLD, especially in cases where biopsy is not feasible.
The management of PTLD depends on several factors, including the type and severity of the disease, the patient’s immune status, and the presence of underlying comorbidities. The primary treatment modality for PTLD is the reduction of immunosuppressive therapy, which can lead to disease regression in up to 60% of cases. However, in some cases, immunosuppression reduction may not be sufficient, and other treatments, such as chemotherapy, radiotherapy, or adoptive cellular therapy, may be required [1, 2, 3]. The optimal management of PTLD remains a matter of debate, and current guidelines recommend a multidisciplinary approach. Despite advances in diagnosis and treatment, PTLD remains a significant cause of morbidity and mortality in transplant recipients, highlighting the need for continued research and development of practical diagnostic and therapeutic approaches. Recently, there has been increasing interest in the use of serum biomarkers, including soluble factors such as sFLCs, as a potential tool for PTLD diagnosis and monitoring [7, 8].
Most patients with PTLD, especially those with early onset of the disease, have detectable EBV DNA in their peripheral blood (also called EBV DNAemia, which indicates circulating virus, free viral DNA, and/or EBV-infected lymphocytes) [6]. The low positive predictive value and lack of specificity of the presence of EBV DNAemia make diagnosing it challenging. Since some individuals with EBV-associated disorders have no detectable DNA in their blood, it is not always appropriate to monitor EBV DNA levels in the blood [7]. Only up to 50% of patients with PTLD show a response to therapy, making the prognosis for this condition similarly unpredictable. Additionally, it might be challenging to gauge a patient’s reaction to treatment, especially if the tumor is difficult to measure or access [8]. The development of PTLD may also be influenced by cytomegalovirus (CMV) infection, possibly through immune system modulation. A wide range of clinical presentations can lead to a delayed diagnosis [9]. A need, therefore, exists for noninvasive markers that can be used for early diagnosis of PTLD that are rapid, readily available, and standardized. Various serum markers can now be used to forecast the development of PTLD. One such biomarker is a serum-free light chain (sFLC). sFLCs are small proteins that are produced by B cells and plasma cells. They are composed of either kappa (
The FLCs, however, have the potential to play a protective role. They prevent myocarditis caused by viruses [13]. A direct antiviral effect and anti-inflammatory effect are supposed to be responsible for this protection, according to Matsumori et al., whereas based to Hutchinson et al., IL-10 may be responsible for this protection through its binding to sphingomyelin on cell membranes, which inhibits viral fusion. According to researchers at Mayo Clinic, polyclonal increases in FLCs have been linked to poorer overall survival. According to another study, patients with FLCs
As part of diagnosing and assessing disease activity, sFLCs are also used to monitor various types of diseases, especially diseases affecting plasma cells [16]. Recent studies suggest that increased levels of kappa and lambda immunoglobulin free light chains (FLCs) in peripheral blood are related to an increased risk of NHL development in HIV-infected individuals, a condition similar to that experienced by transplant recipients [17, 18]. Various assays are currently available to assess serum FLCs (sFLCs). These tests cannot be substituted for one another, and renal function should be considered while analyzing test findings [19]. Plasma cell dyscrasias are often identified and tracked using the levels of kappa and lambda sFLCs. However, in patients with various illnesses, including those who have undergone transplantation, the therapeutic value of sFLCs is being studied [20, 21]. An aberrant monoclonal B-cell population may be present if the kappa: lambda FLC ratio is skewed; in contrast, high lambda and kappa FLC levels indicate polyclonal B-cell activation [22, 23]. A transplant patient’s circulating immunoglobulins can originate from activated B lymphocytes or lymphocytes transformed by EBV [24, 25].
Studies have shown that elevated sFLC levels are associated with an increased risk of developing PTLD and may also be a valuable tool for monitoring the disease. For example, in a study of 104 renal transplant patients, those with elevated sFLC levels were found to have a higher incidence of PTLD compared to those with normal levels (8.8% vs 1.9%). Furthermore, in patients who developed PTLD, sFLC levels were found to be significantly higher at the time of diagnosis compared to pre-transplant levels [17, 18]. The effectiveness of sFLCs in predicting PTLD has produced mixed findings. However, it appears that sFLCs may be helpful in early-onset PTLD prediction. There have been some studies that examine the potential role of sFLCs in PTLD. The results of these studies, however, are controversial. We deemed it necessary to clarify these discrepancies. This article discusses how serum FLC levels may serve as biomarkers in patients with PTLD for diagnosis, prognosis, and treatment response.
Summary of included studies
Summary of included studies
A systematic search of the literature was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [26]. The following search technique was used between Jan 2000 to Sept 2022 to find the eligible studies. Two separate researchers (MT, AJ) searched for the pertinent papers published between Jan 2000 to Sept 2022. The Cochrane Library, Ovid, and Trip databases searched for English-language publications in MEDLINE, EMBASETM, and MEDLINE via PubMed. Our search for material written in different languages included national databases (Magiran, SID), KoreaMed, and LILACS. For literature saturation (MT), the list of included references or relevant reviews was examined. The Health Sciences Librarian website was used to develop unique search techniques focused on systematic review searches using MESH terms and open phrases in compliance with the PRESS criteria. Results from searches in other databases were contrasted with those from the MEDLINE approach after it had been finalized (MT, AJ). Similarly, PROSPERO was looked up to locate recent or active systematic reviews. The terms free light chain OR sFLC OR PTLD OR transplant OR Electrophoresis were utilized in the search approach. The database of earlier study materials and systematic reviews was also explored to find the published research (MT, AJ). A search for unpublished data and abstracts (MT) was also conducted on all papers that met the inclusion criteria.
Eligibility criteria
The addition of Cross-sectional, case-control, cohort, case reports, and review publications with the Availability of full text were the articles that met the criteria for the systematic review. Non-random sample size, lack of relevance to the issue, duplicate studies, and inadequate data were among the exclusion criteria. Two researchers carried out each of the stages mentioned above separately to prevent bias in the study. Finally, the consistency of the third researcher’s findings was checked.
Study selection and data extraction
All pertinent publications were initially gathered, and a list of abstracts was created to help special investigations. The complete text of the publications was given to the researchers after the specifics, such as the name of the journal and the author, had been concealed. Two researchers independently examined each publication; if the article was rejected, the reason was stated. In the event of a dispute between the two researchers, a third researcher evaluated the paper.
Quality of included studies
It includes the following nine parameters: sample size, mean age, kappa rate, lambda rate, Abnormal FLC rate, Transplanted organ, PTLD pathology, Timing of FLC measurements, and outcome. We evaluated their quality in terms of sample size, a critical predictor of study quality, and the laboratory parameters assessed in the research (Table 2).
A general overview of the study (first author, country, and year of publication) and study details (sampling method, data collection method, the proportion of females versus males, number of participants, mean age, and the general population) were extracted (Table 1).
The quality of the articles that is calculated using a checklist which includes nine criteria
The quality of the articles that is calculated using a checklist which includes nine criteria
PRISMA flow diagram.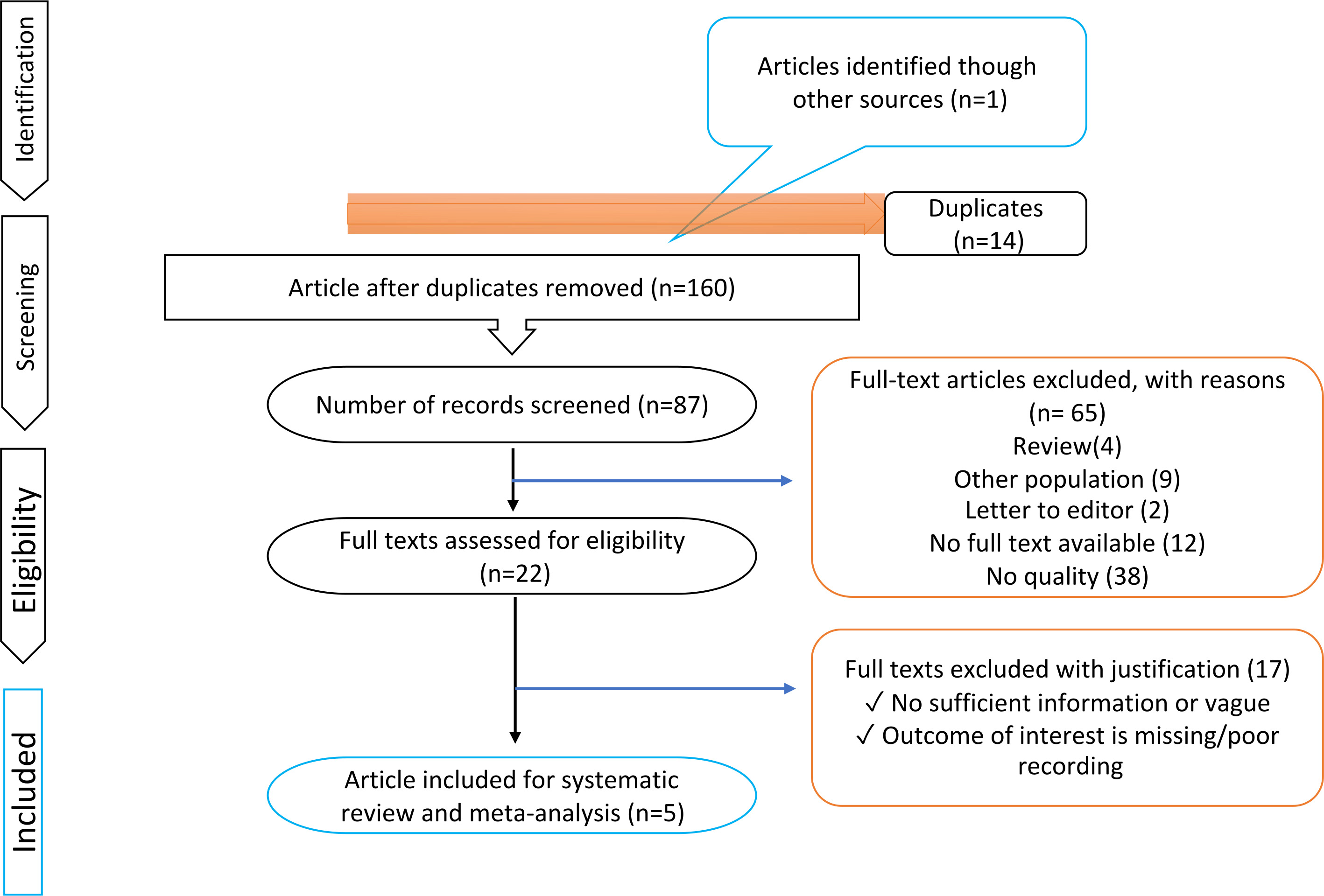
Study selection
One hundred seventy-four studies were found in the initial stages of our extensive search. Sixty-five studies were omitted after titles and abstracts were examined. Seventeen papers were eliminated after a thorough analysis of the text and consideration of the inclusion/exclusion criteria, and ultimately, five studies were chosen as appropriate for systematic review (Fig. 1). In order to assess light-chain immunoglobulins in serum, a serum-free light-chain test, also known as the SFLC assay, was created in 2002. The specificity of this assay lies in its ability to detect an epitope on a free monoclonal light chain. The methods used to analyze sFLC levels in the included studies involved the use of automated immunoassays. In immunonephelometry, SFLC tests are performed on automated laboratory instruments using a commercially available reagent set of polyclonal antibodies (FreeliteTM Assay, The Binding Site Ltd., Birmingham, United Kingdom). Studies report sFLC levels adjusted for renal function, suggesting the use of a similar method. None of the references mention any standardized techniques or equipment used beyond the immunoassay methodology. This was among the first immunological tests for immunoglobulins (light chains). It measures the light chains
The SFLC assay can detect levels as low as one mg/L of free monoclonal light chains compared with other methods. Contrary to this, serum protein electrophoresis (SPEP) and serum or urine immunofixation electrophoresis (IFE) is limited to measuring levels of 1,000 mg/L and 150 to 500 mg/L, respectively. The specificity offered by analyzing the
However, this approach also has drawbacks, such as:
For AL amyloidosis, 24-hour urine collection is required because monoclonal proteins can only be found in urine. As an adjunct to serum IFE, but not as a stand-alone assay Several false negatives and positives have been identified
There is a difference in how therapy response and remission are evaluated (using the SFLC test or the
Assessing the concentration of free light chains can be used to define early relapse, strict complete response, or partial response, predict treatment failure earlier, and detect light chain escape.
It is possible to identify PTLDs or other disease-status indicators through SFLC in addition to reducing repeated biopsies and examinations; however, the evidence for this is mixed. Additionally, given that B-cells are the source of the majority of PTLDs, markers for aberrant B-cells may assist in identifying patients at a high risk of suffering this negative result [29]. Immunosuppressive medication is linked to a higher risk of developing PTLD in organ transplant patients. This condition is primarily B-cell-derived, and almost 80% of cases have Epstein-Barr virus (EBV) positivity. B-cell failure brought on by the EBV virus might increase sFLCs.
The sFLCs in PTLD and non-PTLD patients
In 2012, Engels and colleagues found higher FLC levels in cases than controls (median 1.53 versus 1.07 times ULN (optimum range of normal) for kappa, 1.03 versus 0.68 times ULN for lambda). Measurements were obtained at two-time points (prediagnostic and diagnostic specimens): 46–63% of controls and 69–72% of cases had elevated kappa FLCs, while 25–28% of controls and 52–59% of cases had elevated lambda FLCs. Cases showed an aberrant FLC ratio of 14–31% compared to the controls’ abnormal FLC ratio of 11–12%. There was an anomalous FLC ratio in only two subjects (both of whom had PTLD), without an elevation in either kappa or lambda. Whenever prediagnostic samples are utilized, FLC elevations with polyclonal patterns had a stronger association with subsequent PTLD (OR 4.2) than FLC elevations with monoclonal patterns (OR 3.0), howbeit there was no discernible difference between the increase of polyclonal and monoclonal cells (
According to another study by Engels and colleagues in 2013, An evaluation of sFLCs was suggested as a marker to assist in identifying those who are at high risk for developing PTLD in other research that involved 36 juvenile transplant recipients (half of whom had received a liver transplant and 12 had the disease). Hematopoietic stem cell transplant (HSCT) recipients, all of the HSCT donors, and six liver recipients had EBV seropositivity at the time of the transplant. In 20.8 percent and 28% of plasma specimens,
Similar to the previous study, greater EBV loads were associated with significantly higher levels of sFLCs. A polyclonal sFLCs elevation was often seen at least four times more frequently than a monoclonal sFLCs elevation (26 percent of the specimen,
Regarding renal function, Borrows and associates looked at the value of sFLCs measures in PTLD and non-PTLD patients. Cystatin C was used in the study by Borrows and colleagues to evaluate renal function in this setting. Renal impairment is a prominent confounder in studies of FLC Levels because the kidneys quickly eliminate blood FLC. This was a significant omission from earlier research. During sample collection, CRP levels from patient records were collected to control for FLC production brought on by inflammatory processes. There was no significant correlation between CRP levels and any of the FLC or HLC measures investigated, and two of the three individuals with CRP levels of more than 10 mg/dL had cFLC values that were near the median for cFLC levels (66.9 mg/dL, 83.5 mg/L, and 193.0 mg/dL). Renal function was modified to consider renal function when FLC levels were standardized to serum cystatin C (both values provided as mg/L and consequently dimensionless). As a result, patients with PTLD had considerably higher combined FLC levels (cFLCadj) than did controls (35.74 [range 2.88–693.37] vs 24.80 [range 8.85–100.91]). Adjusted FLCs levels cannot be utilized to evaluate therapy response alone. In the future, it may be utilized for disease surveillance. Low adjusted sFLC levels in PTLD patients with CR may or may not be prognostic at this time [28].
In this study, potential confounding factors such as age, sex, underlying disease, donor-recipient relationship, graft source, conditioning regimen, and use of immunosuppressive medications were considered in the analysis. It is important to note that the studies included were conducted in different populations and may have used different methods to control for potential confounding factors. Therefore, it is essential to carefully evaluate each study and its methods before drawing any conclusions.
In the study by Borrows et al. [27], potential confounding factors such as age, gender, time since transplantation, and medications were considered in the analysis. The study adjusted for creatinine clearance, as sFLC levels can be affected by renal function, and excluded patients with active infection, inflammation, or hematological malignancy. Additionally, the study included patients with various types of solid organ transplants, including kidney, liver, heart, and lung, and adjusted for the type of transplant in the analysis. Overall, the study aimed to minimize the influence of confounding factors and to evaluate the potential utility of sFLC levels as a biomarker for PTLD [28].
In the study by Engels et al. [10, 18, 26], potential confounding factors such as medication use, Epstein-Barr virus (EBV) serostatus, and other medical conditions were considered in the analysis. The authors adjusted for age, sex, race, time since transplantation, and history of acute rejection or hepatitis C virus infection. Additionally, they assessed the impact of immunosuppressive medication regimens on the risk of PTLD. The study found that donor-specific antibodies, high levels of immunoglobulin-free light chains, and high levels of B-cell activating factor were all associated with an increased risk of late-onset PTLD in liver transplant recipients, even after adjusting for these potential confounding factors [10, 11, 27].
We have performed a deep analysis of the current literature to assess whether sFLC may be helpful as a noninvasive biomarker in PTLD patients. In particular, plasma cell disorders are treated using the sFLCs for diagnosis, evaluation of disease activity, and therapy monitoring. Several disorders are now being researched to see if sFLCs are beneficial. A total of seven articles were identified regarding the usefulness of sFLC in PTLD patients, one of which was a case report study [30]. Although various innovative uses of the SFLC test have been suggested in recent narrative reviews to help with the diagnosis, monitoring, and prognostic evaluation of PTLD, such uses have not been extensively studied.
After solid organ transplantation, it has been demonstrated that an assay for FLC that is sensitive, repeatable, and easily accessible correlates with the emergence of PTLD.
There are three (perhaps complementary and not necessarily exclusive) theories to account for the association between high FLCs and PTLD. First, polyclonal B cell activation may be a critical factor in lymphoproliferative illness, as activated (albeit not clonal) B cells produce polyclonal FLC. Second, the clonally growing lymphoma cells themselves release monoclonal FLCs. Third, FLC increases show EBV proliferation and (implicitly) lymphoma linked to the virus.
In 2012, Engels and colleagues demonstrated an association between high sFLC levels, high EBV viral loads, and a greater risk of developing PTLD. They found that B-cell failure brought on by the EBV virus might increase sFLCs. It is noteworthy that PTLD cases from a single transplant center were represented in this study, in which controls without PTLD were matched carefully to PTLD cases, and prediagnostic samples were available from PTLD cases. In stratified analyses, the study was nonetheless limited by the small specimen size. FLC elevations and EBV DNAemia were not associated with PTLD independently because EBV DNAemia data were often missing [27].
The Fernando research demonstrated that sFLC is not a reliable predictor of the development of PTLD because there was not a single patient with PTLD with an sFLC ratio outside of the usual or renal range. This study included a small number of cases due to the rarity of PTLD. In order to achieve a reliable conclusion, they used a nested case-control design with oversampling of controls [17].
In a 2014 study, Deborah Kuhn and associates concluded that high FLC concentrations and aberrant gammopathy were related to PTLD. Because of this, solid organ transplant recipients should be screened for PTLD using the FLC test and SPE. Both methods may not be appropriate for tracking PTLD in the post-transplant population since neither was linked to the date of PTLD diagnosis [30].
In another study by Engels and colleagues in 2013, FLC abnormalities were detected in 20–28% of plasma specimens. The most frequent problem was polyclonal FLC excess, where the lambda and kappa FLCs were proportionally amplified to restore a standard kappa/lambda FLC ratio. Also, higher EBV loads were associated with enormously increased levels of three biomarkers (kappa and lambda FLCs, sCD30). Higher EBV loads are linked to measurable elevations in circulating B-cell activation markers because EBV-infected B-cells proliferate more often. It would be of considerable interest to identify a subset of receivers who are most at risk of developing PTLD, particularly before PTLD becomes clinically apparent [10]. Previous studies have linked high levels of immunoglobulin-free light chains (FLCs), which are antibodies produced after B cell activation, with high levels of EBV viral load and PTLD development following solid organ transplantation. It is possible that B cells from early-stage malignancies created FLCs since some FLCs are recovered close to the time of PTLD diagnosis. Furthermore, half of the cases of PTLD arise within the first year following transplantation, indicating that FLC levels significantly impact PTLD incidence within that period.
Notably, a prior study [26] showed that elevations in FLC were significant predictors of PTLD development within a half-year. Though some instances did not have specimens available prior to diagnosis, no PTLD case with previous monoclonal FLC increases was noted in the current investigation (the earliest was the time of PTLD diagnosis). This study’s strength was the inclusion of solid organ and HSCT recipients, those with and without PTLD, and various EBV loads [10, 27]. In order to enable longitudinal comparisons, the markers were also evaluated in several samples obtained from transplant patients before PTLD diagnosis. The fact that the study’s participants were chosen from earlier clinical research was a drawback. They might not thus be representative of other transplant recipients. There is no information on how these markers could relate to different recipient populations (for example, adults and recipients of other solid organs). Additionally, the limited sample size precluded thorough studies of transplant recipient subgroups (e.g., liver and HSCT recipients separately).
High levels of immunoglobulin-free light chains (FLCs), which are antibodies generated after B cell activation, have been associated in earlier studies by Engels with high levels of EBV viral load and the development of PTLD following solid organ donation. Since some FLCs will be recovered close to the time of PTLD diagnosis, it is possible that B cells from early-stage malignancies created the FLCs. It appears that FLC levels significantly impact PTLD incidence within the first year following transplantation since approximately half of the cases arose within that period.
Contrary to this, the present study had only six PTLD cases diagnosed within the first year of transplantation and none within the first two years. Furthermore, compared with the current study (median, 2.4 years), the prior study (median, 0.3 years) revealed shorter intervals between FLC measurement and PTLD diagnosis. As a result, FLC elevations in the earlier study, which were found at the time of diagnosis, might have primarily been immunoglobulin fragments produced by the PTLD cells themselves just before the tumor became clinically evident and may not have been an indication of the underlying immune abnormalities that caused PTLD to develop in the early stages of the disease process. This study’s ability to include a variety of immunoreactivity markers for the donor organ was a plus. This study’s limitations include the overall low number of PTLD patients.
Additionally, several recipients’ measures were missing due to assay issues, forcing them to abandon the case-control matching (particularly for FLCs). Furthermore, many of the transplants were for late-onset PTLD since they were done in an earlier period. While transplant practices have changed over time for immunosuppressive regimens and rejection monitoring, it is uncertain if these would have impacted the relationships found [11]. According to Borrows’ study, FLC levels were strikingly similar to those found in Engels’ studies, suggesting generalizability to other populations. Further, Borrows’ study was consistent with that study’s finding that polyclonal and monoclonal FLC elevations (separately and together) were related to PTLD diagnosis. Despite Fernando’s previous study not finding this effect, its smaller size limited its robustness. It is crucial to remember that although FLC levels are a general indicator of inflammation, most of their patients with PTLD after solid organ donation lacked clinically significant CRP rises.
The kidney function was evaluated by measuring cystatin C in this context. Previously, FLC levels have been studied without considering renal impairment, one of the most critical confounders of FLC studies. In order to account for this confounder, they changed the basic FLC levels to consider that glomerular filtration removes polyclonal FLCs from the circulation has been advised that this modification be made in renal cohorts since cystatin C and FLC levels show the best connection as a renal excretory marker. Furthermore, the ROC curve studies point to possible predictive usefulness that has not been previously investigated in this context; PTLD may be “ruled in” with 91 percent specificity when FLC levels are changed. Although the ‘cutoff’ value presented here has limited sensitivity, it is of limited utility in ruling out diseases.
Additionally, such data should not be over-interpreted since they are derived from a single cohort and have a margin for error. Although it appears logical to alter FLC levels by renal function, future prospective studies in transplant cohorts should ascertain whether this technique has any evident advantages and whether the ’diagnostic’ cutoff values they have discovered are reliable and generalizable. Additionally, the relationship between FLC levels and the clinical course was investigated. When monitoring tumor restaging, FLCadj levels were lower in patients who sustained complete remission than in those who experienced partial remission or disease progression. FLC measurements may play a role in disease surveillance based on these results [28]. The first two hypotheses mentioned at the beginning are supported by the findings of the Borrows et al. study, which also discovered links between polyclonal and monoclonal FLC increases and PTLD. The Borrows study cannot support or disprove the third hypothesis since the dataset did not contain any information on EBV viremia.
Limitations and future research
The limitations of the review include the potential for publication bias, as only published studies were included, and the small sample sizes of some of the included studies. The limitations of each study included in the review were also taken into account during the data synthesis and analysis. The process of confirming the validity of diagnostic criteria for PTLD varied among the studies included in this review. However, many studies used the diagnostic criteria established by the World Health Organization (WHO) for PTLD, which includes histological analysis of tissue biopsy samples and the evaluation of clinical features such as lymphadenopathy, fever, and weight loss. In some studies, additional laboratory tests such as EBV viral load measurements and imaging tests such as CT scans were also used to aid in the diagnosis of PTLD. Additionally, some studies required confirmation of PTLD diagnosis by a pathology review board or multiple pathologists to ensure the accuracy of the diagnosis.
However, in general, some studies have suggested that sFLC levels may differ between different subtypes of PTLD. For example, a study published in the journal Transplantation Direct in 2018 found that higher levels of sFLCs and donor-specific antibodies were associated with an increased risk of late-onset PTLD in liver transplant recipients [11]. Another study published in the Annals of Hematology in 2019 suggested that sFLC levels adjusted for renal function may be a potential biomarker for post-transplant lymphoproliferative disorders, though this study did not differentiate between PTLD subtypes. It is important to note that further research is needed to fully understand the relationship between sFLC levels and PTLD subtypes [28].
There have been several previous studies on the use of sFLCs as a biomarker for PTLD. The results of this systematic review are generally consistent with those of previous studies, which have also shown that sFLCs are a promising biomarker for PTLD. However, the studies included in this systematic review provide more comprehensive and robust evidence for the use of sFLCs as a biomarker for PTLD, as they are based on larger sample sizes and have more consistent findings. Additionally, this systematic review highlights the need for further research to optimize the use of sFLCs as a biomarker for PTLD, including the development of standardized measurement methods and the identification of optimal cutoff values for different patient populations.
There is limited data on the long-term prognosis of PTLD patients with elevated sFLC levels. The studies included in the systematic review mainly focused on the association between sFLC levels and the risk of developing PTLD rather than the prognosis of those already diagnosed with PTLD. However, one study included in the review by Borrows et al. [27] did report that higher sFLC levels at the time of PTLD diagnosis were associated with poorer overall survival among renal transplant recipients with PTLD [28]. Further studies are needed to investigate the long-term prognosis of PTLD patients with elevated sFLC levels.
There were no studies specifically evaluating the cost-effectiveness of using sFLCs as a diagnostic tool for PTLD. However, cost-effectiveness analyses would typically consider factors such as the cost of the test, the accuracy of the test, and the potential benefits (e.g., earlier detection, improved outcomes) of using the test compared to current diagnostic methods. Based on the current evidence, it appears that sFLCs may have some potential as a biomarker for PTLD, mainly when used in combination with other diagnostic tools. However, further research is needed to better understand the clinical utility and cost-effectiveness of sFLCs for PTLD diagnosis.
Also, there were limited data on the use of sFLCs in monitoring response to treatment for PTLD. One study published in the journal Blood in 2010 evaluated the utility of sFLCs in monitoring response to rituximab therapy in patients with PTLD after solid organ transplantation. The study found that a decrease in sFLC levels after treatment was associated with a better response to therapy and improved overall survival. However, larger studies are needed to confirm these findings and to evaluate the potential use of sFLCs as a tool for monitoring response to treatment for PTLD.
The use of different sFLCs assays and the lack of data from extensive prospective studies indicating the efficacy of sFLCs measurements in solid organ transplant patients are the two most critical current limits on the clinical relevance of sFLCs in transplantation. However, non-controlled confounding factors have the potential to significantly affect results from case-control studies with a small number of patients. Therefore, it is essential to conduct prospective clinical studies to validate our results and ascertain the extra usefulness of FLC levels in treating PTLD. It is important to note that, based on available evidence, sFLCs may be particularly helpful in the first two years following transplantation. They can be used alone to predict early-onset PTLD and, possibly in conjunction with immunoglobulins screening, to predict infection. The ability to evaluate the number of sFLCs in patients following transplantation and their quality may become essential in the future. Perhaps sFLCs can aid in diagnosing conditions other than PTLD or transplant-related consequences. To prove that interest in sFLCs is warranted, more research is required.
In terms of future research, larger studies with a control group are needed to confirm the relationship between sFLC levels and PTLD. It would also be helpful to determine whether sFLC levels can be used as a predictive biomarker for the development of PTLD. Additionally, further research is needed to evaluate other potential biomarkers and develop a comprehensive approach to monitoring and predicting PTLD in transplant patients. Finally, it would be valuable to investigate whether sFLC levels can be used to monitor response to treatment and predict outcomes in PTLD patients.
Conclusion
This systematic review was conducted to assess the available evidence on the topic of interest. The search strategy was comprehensive, and the eligibility criteria were clearly defined. The quality of the included studies was assessed, and the findings were synthesized and analyzed using a narrative approach. In summary, this systematic review provides current evidence on the potential clinical applicability of sFLCs in predicting early-onset PTLD in solid organ transplant recipients. Our findings highlight the importance of interpreting sFLC results in the context of renal function and emphasize the need for caution when attempting to use sFLC assays interchangeably. The review also emphasizes that plasma cell dyscrasia can be diagnosed and monitored by measuring the sFLC percent and FLC ratio.
However, the small sample size of the final five studies included in this review limits the generalizability and validity of the results. While the preliminary results of our review are promising, it is clear that more research is needed to confirm the validity of sFLCs in predicting PTLD and other transplant-related complications. Nonetheless, the biomarker potential of sFLCs in identifying early-onset PTLD within the first two years after transplant holds significant implications for clinical practice. This finding has significant implications for clinical practice, as early diagnosis and treatment of PTLD can improve patient outcomes and survival rates.
It is important to note that the contradictory findings in the current literature suggest the need for further investigation into the quality, as well as the quantity, of sFLCs in transplant recipients. Future studies may also explore the potential use of sFLCs in predicting other post-transplant complications or diseases. Overall, the findings of this review underscore the potential of sFLCs in improving patient care and highlight the need for continued research in this area.
Abbreviations
PTLD: posttransplant lymphoproliferative disorder EBV: Epstein-Barr virus FLC: Free light chain CMV: cytomegalovirus NHL: non-Hodgkin lymphoma SPEP: serum protein electrophoresis IFE: immunofixation electrophoresis
Author contributions
Concept and design: IS, NH.
Data gathering: MH I.
Data analysis: MA.
Drafting the manuscript: AJ, SH R.
Critically revising the manuscript: IS, AJ, MT.
Supervision: IS, AJ.
Footnotes
Conflict of interest
The authors declare no any conflict of interest regarding the publication of this article. The authors gave their consent for publication in this journal.