
Abstract
BACKGROUND:
Although the detection of immunoglobulin G (IgG) molecules has long been considered to be crucial for successful humoral immune defence against infections and harmful metabolites, it has become increasingly important in relation to SARS-CoV-2 research.
OBJECTIVE:
To compare longitudinal changes in IgG titres in post-infection and post-vaccination Iraqi participants, and to estimate the protective benefits of the two principal vaccines used in Iraq.
METHODS:
This quantitative study used samples from SARS-CoV-2 recovered patients (
RESULTS:
IgG antibody levels peaked in the first month and tapered off in the following three months in both convalescent and vaccinated groups. The latter showed a significant decrease in IgG titres than in the convalescent group. Samples from the group given the mRNA vaccination that targeted spike (S) proteins might have a cross-reactivity between nucleocapsid (N) and spike (S) proteins.
CONCLUSIONS:
Participants who had recovered from or who were vaccinated against SARS-CoV-2 exhibited a protective, persistent and durable humoral immune response for at least a month. This was more potent in the SARS-CoV-2 convalescent group compared to the vaccinated cohort. The IgG titres decayed faster after vaccination with Sinopharm than following the Pfizer-BioNTech vaccine.
Introduction
The recent global coronavirus pandemic resulted in more than 600 million SARS-CoV-2 infections and 6 million deaths worldwide. Although the proportion of vaccinated individuals has increased significantly, the virus has mutated in such a way as to cause infection rates to continue to rise. A pertinent question, therefore, is how efficient and durable vaccination is in protecting against infection with SARS-CoV-2.
Immune response is a critical aspect of controlling SARS-CoV-2 infection. As a result of the innate and adaptive (acquired) immune responses [1], immunological dysregulation can drastically alter the clinical outcomes of patients infected by SARS-CoV-2 [2]. Adaptive immune responses involve B cells, which provide humoral responses in order to generate antibodies, including immunoglobulin (Ig) M, IgG and IgA, as well as lower titres of IgD and IgE. Four to eight days following symptom onset, these antibodies act against the spike (S) protein [3] by binding to the (S) and other membrane proteins, and neutralise the virus naturally [4].
In addition to natural immunity, vaccines are able to elicit degrees of artificial immunity through the innate and adaptive immune responses, which lead to the activation of lymphocytes and the secretion of antibodies within the body, respectively. In order to address the global coronavirus pandemic in an effective and substantial manner, an impressive number of SARS-CoV-2 vaccines were developed using various technologies and with differing levels of success. The vaccine innovations against SARS-CoV-2 include live attenuated viral vectors, inactivated vaccines, subunit vaccines, and recombinant and DNA vaccines [5]. Currently, 334 vaccines have been developed, of which 194 and 140 are still in the preclinical and clinical trial stages, respectively [6]. Worldwide, the most popular coronavirus vaccines encompass Pfizer-BioNTech, Moderna (mRNA-1273), Oxford/AstraZeneca, Johnson and Johnson, Sinopharm, Sinovac and Covaxin [7]. In Iraq, the location which forms the focus of this study, the most common vaccines used are Pfizer-BioNTech, Oxford/AstraZeneca and Sinopharm.
Both previously infected patients and vaccinated individuals possess antibodies that reduce the risk of SARS-CoV-2 infection. However, as the virus continues to mutate, evaluating and comparing the varying levels of protection amongst both vaccinated and previously infected populations are required so as to determine whether immunity against SARS-CoV-2 is waning and whether additional vaccine doses are necessary in order to regain immunity [8]. This study, therefore, seeks to understand the immune responses and their endurance against the virus by detecting anti-SARS-CoV-2 nucleocapsid (N) protein in samples from convalescent patients and vaccinated individuals during the three months following infection and vaccination, respectively.
Methods
Study ethical considerations
This research was approved by the Institute of Genetic Engineering and Biotechnology for the Postgraduate Studies Committee, as well as the Iraqi Ministry of Health Research Committee (form number 01/2021). Participant consent was obtained prior to enrolment in this study.
Subjects
In order to examine the way in which IgG antibody levels and seroprevalence change over time, samples were collected from individuals, hospitals, i.e. Dar Al-Salaam 1 Field Hospital and Al Shifa Specialised Centre, and private laboratories, i.e. Istishari Medical Laboratory, Diqat Al Rawaa and Al-Safa Private Laboratories, between December 2021 and June 2022. A total of 200 individuals participated and were divided into the following three categories: (i) convalescent patients (
Molecular diagnosis of SARS-CoV-2 infected participants
Comparison of the IgG titers between studied groups and control
Comparison of the IgG titers between studied groups and control
Non-significant relationship of the IgG titers with sex in convalescent and vaccinated group.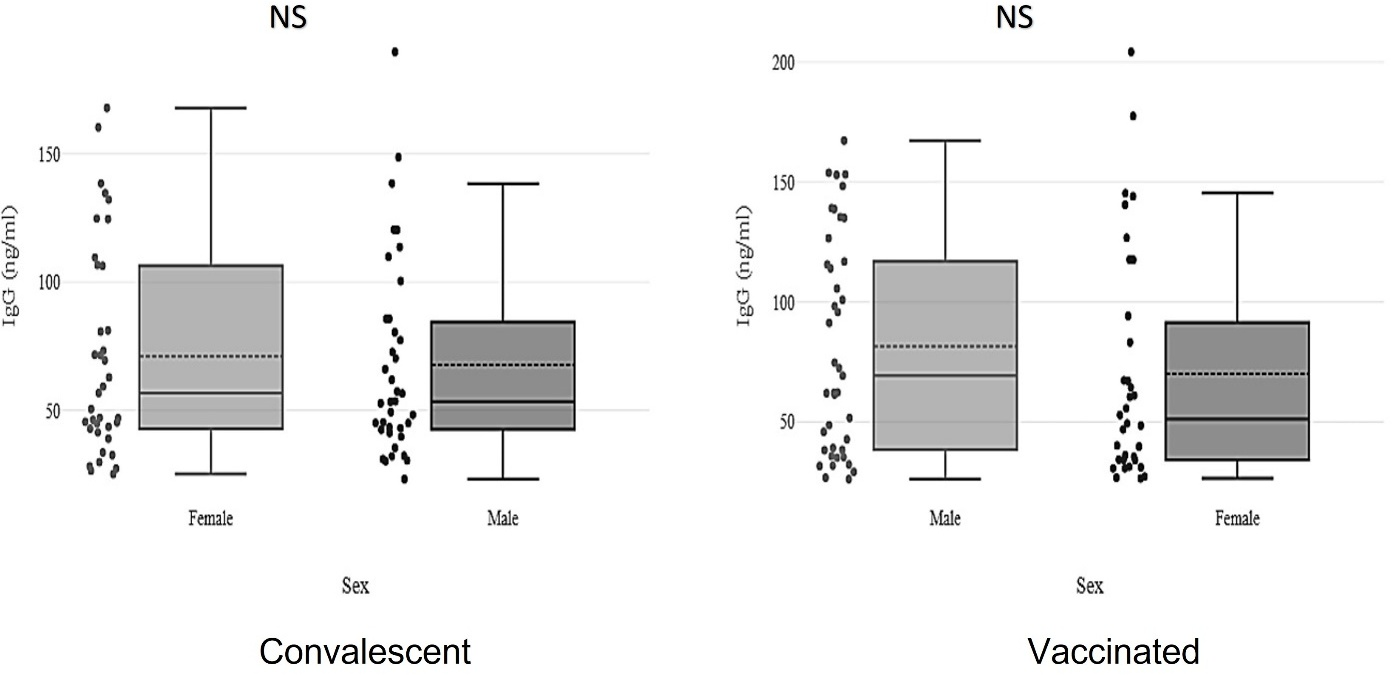
All previously infected participants (
The target antigen, the anti-SARS-CoV-2 (N) protein (catalogue no. MBS7608188), was assessed in order to determine the seroprevalence and antibody responses to SARS-CoV-2 infection and vaccination in serum samples using the human anti-SARS-CoV-2(N) IgG coronavirus enzyme-linked immunosorbent assay (ELISA) kit (BioSource, USA). The anti-SARS-CoV-2 IgG antibody response was present in 100% of samples after setting the cut-off value to 30.21 ng/ml in accordance with the manufacturer’s manual. The indirect ELISA technique used to detect and to quantify IgG comprised a two-step process during which the specific primary antibody binds to the intended antigen, and a secondary antibody targets the host species of the primary antibody for detection. The absorbed IgG concentration was recorded at a wavelength of 450 nm.
Statistical analysis
Statistical analysis was performed using the IBM Statistical Package for Social Sciences software, version 28.0 (SPSS, Chicago, IL, USA). T-tests were utilised to compare two means, and one-way analysis of variance was used to determine the differences between demographic variables and multiple comparisons. A Pearson correlation test was employed for the assessment of any correlations between study parameters and age.
Results
IgG antibody detection in SARS-CoV-2 convalescent and vaccinated groups
The gradual decline in IgG titers in each month of the follow-up.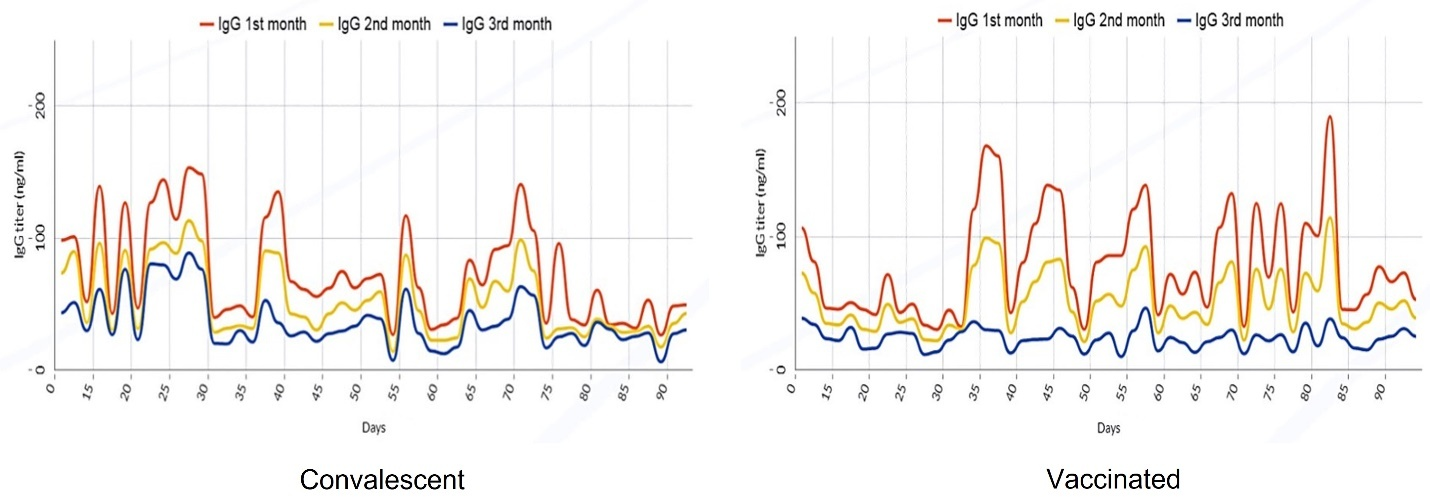
The IgG titers relationship with the type of vaccine for each month of the follow-up.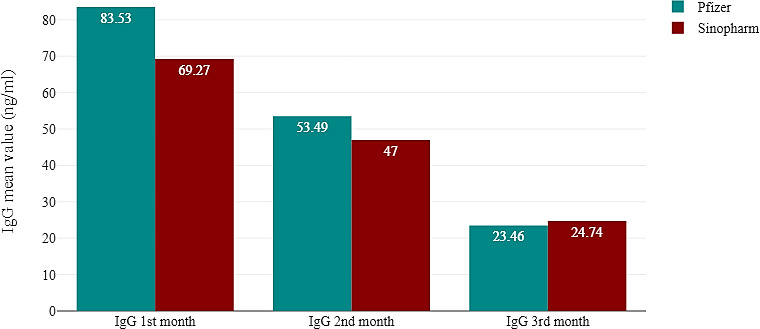
Mean IgG titres were higher in the convalescent (79.17 ng/ml) than in the vaccinated (69.33 ng/ml) group; the lowest mean IgG value (24.75 ng/ml) was observed in the control group. As expected, the findings revealed a highly significant difference between the convalescent and vaccinated groups compared to the control cohort (
Although Fig. 1 appears to show that changes in IgG levels corresponded to participants’ sex, no significance differences between IgG titres in male or female participants were identified in either the convalescent (
IgG follow-up data from SARS-CoV-2 convalescent and vaccinated groups
IgG antibody levels in the convalescent group reached their peak after one month of infection and gradually declined over the three-month follow-up period (Fig. 2). A highly significant (
In keeping with the IgG titres observed in the convalescent group, IgG antibody levels in the vaccinated group (Fig. 2) were at their highest (189.74 ng/ml) during the first month after the two Pfizer or Sinopharm doses. However, the titres observed over the three-month follow-up period plummeted much more quickly, with the lowest IgG value reaching 9.97 ng/ml.
Notably, samples collected from participants who received the Sinopharm vaccines revealed lower mean values for each of the follow-up months compared to samples from those who were administered the Pfizer vaccines, indicating that IgG titres decayed at a faster rate with the former make of vaccine (Fig. 3).
Discussion
The detection of IgG molecules has been a vital aspect in SARS-CoV-2 research as they offer a measure of the humoral immune defence responses against infections and their harmful metabolites. This makes it possible to confirm past infections, especially amongst symptomatic convalescents, and to assess the longevity and endurance of antibody-mediated protective immunity [9, 10]. In keeping with research carried out since the beginning of the COVID-19 pandemic, this study confirms that IgG antibodies remain high in the three-month period following infection [11, 12].
Interestingly, although the immune response to the mRNA vaccines is based on the (S) sequence of the SARS-CoV-2 as an immunogen, which means that it will only be directed against the spike receptor binding domain RBD, this study showed detectable and relatively high titres of anti-SARS-CoV-2 (N) protein in participants who had received the Pfizer vaccine. Dobaño et al. (2022) evaluated the humoral response induced by mRNA vaccination and observed a highly significant IgG antibody response to the (N) proteins, and correlated the increase in antibody response to the (N) antigen with the cross-reactivity between the (N) and (S) epitopes. The cross-reactivity of the SARS-CoV-2 structural proteins was described by Bates et al. (2021). These researchers identified a significant anti-SARS-CoV antibody level which exhibited strong cross-reactivity with anti-SARS-CoV-2 antibodies and specifically, with the alignment the (N) C-terminal region primary amino acid sequence and (S) protein. These results provide evidence for the presence of cross-reactivity between (N) and (S) proteins.
The current study’s comparisons of IgG levels across the demographic categories were supported by previous studies. Firstly, females who received the SARS-CoV-2 vaccinations demonstrated greater immune responses and thus, higher antibody levels compared to males. This discrepancy has been attributed to various biological differences, including sex hormones and the expression of X-linked genes which have been shown to induce sex-based disparities in immune responses to vaccines [13, 14, 15]. Secondly, age is a widely recognised cause of immune dysfunction as the immune functions of elderly individuals alter through the process of immunosenescence [16]. This study substantiates the findings of Ueno et al. [17], confirming that the IgG antibodies in samples collected from elderly convalescents had a much longer clearance period and were of a higher titre due to virus shedding than those in samples from younger patients. Conversely, samples collected from elderly vaccinated individuals demonstrated a lower immunity response compared to those from younger and middle-aged vaccination recipients. Pellini et al. [18] first studied the relationship between age and antibody response and found that immunosenescence can lead to a decrease in vaccination effectiveness.
The findings of this follow-up study were supported by the majority of existing studies, which presented the gradual decline and waning endurance of IgG antibody levels following infection and natural antigen clearance processes [19, 20, 21]. However, some literature spanning a similar post-infection time period suggests that the humoral immune responses sustained antibody levels through and for months following the three-month observation range evaluated in this study [22, 23].
It was recognised in the current study that although a decline in antibody levels was evident, immunity responses to vaccination were extensive and effective. Studies by Favresse et al. [24] and Xu et al. [25] indicated similar outcomes, in that the decline of anti-SARS-CoV-2 antibody levels, after mRNA and inactivated vaccinations, exhibited strong and significant correlations with vaccine success [24, 25]. Additionally, follow-up records of IgG antibody attenuation in vaccinated individuals indicated a similar fall in antibody levels to that seen following natural infection, consistent with the findings of Dou et al. [26].
Researchers described the reduction in IgG antibody levels as the waning of immunity after the vaccines had been administered, regardless of the type of vaccines used. Shrotri et al. [27] studied immune responses after two doses of either Pfizer or AstraZeneca vaccines and found a noticeable decrease in IgG antibody levels at ten weeks following the second dose, regardless of the vaccine type. Similarly, Addo et al. [28] found antibody levels became attenuated as early as one month after a complete double-dose vaccination administration, a process which continued for sixth months until the antibody levels were deemed too low to provide sufficient protection against SARS-CoV-2. Nevertheless, although antibody levels are proven to decrease over time, mRNA vaccines, specifically the Pfizer-BioNTech vaccine, are more effective in preventing COVID-19 than inactive vaccines, such as Sinopharm [29, 30].
Conclusions
Despite the fact that both natural infection with SARS-CoV-2 and vaccination are equivalent in inducing the host immune system response, IgG titres were higher in the convalescent group than in the vaccinated group one month after infection and vaccination, respectively. This might indicate that natural infection conveys a higher degree of immunity and durability than the vaccination. For individuals who have received the SARS-CoV-2 vaccines, detectable and relatively high titres of anti-SARS-CoV-2 (N) protein successfully targeted the (S) protein, indicating the presence of cross-reactivity between (N) and (S) proteins. However, although IgG immune response levels have been proven to provide effective protection against SARS-CoV-2 initially, the benefit of humoral immunity noticeably wanes in some individuals during the first three months, resulting in insufficient protection against COVID-19 after the follow-up period. Thus, individuals who have been vaccinated or have previously tested positive for coronavirus may experience reinfection over time. This study has significant implications for the control of the COVID-19 pandemic, with respect to the use of IgG testing for the monitoring of infection outbreaks against SARS-CoV-2 and the subsequent reduction of reinfections.
Author contributions
Conception: Fadia M. Maki and Amina N. AL-Thwani.
Interpretation/analysis of data: Fadia M. Maki and Amina N. AL-Thwani.
Preparation of the manuscript: Fadia M. Maki and Karar N.J. Musafer.
Revision for important intellectual content: Amina N. AL-Thwani and Kareem S. Jiad.
Supervision: Amina N. AL-Thwani and Kareem S. Jiad.
Funds
None.
Footnotes
Acknowledgments
No funding was received for this research. The authors thank all the nurses, laboratory technicians and convalescent patients who participated in this research and assisted with blood sample collection.
Conflict of interest
The authors declare that they have no conflict of interest.