
Abstract
BACKGROUND:
Physical exercise has been proposed as a new alternative to chemical adjuvants.
OBJECTIVE:
To investigate the relationship between regular exercise and post-vaccination antibody response in the elderly.
METHODS:
The study was conducted with the elderly over the age of 65. 30 participants we randomized into 2 groups and divided into exercise and control groups. The experimental group received a 12-week exercise program. The control group was followed up without any exercise. The day on which the second dose of the vaccine was administered to all participants was considered day 0. The antibody level in the serum samples was taken 15 days and 12 weeks after the vaccination. The antibody concentration was measured after the second dose of vaccination.
RESULTS:
The mean antibody level in the control group was 69.4 U/ml and 56.4 U/ml 15 days and 12 weeks after the second vaccination. The mean antibody level in the exercise group was 74 U/ml and 71.6 U/ml 15 days and 12 weeks after the second vaccination.
CONCLUSIONS:
Regular exercise of light to moderate intensity may increase post-vaccination antibody response in the elderly. Therefore, exercise can be used as a behavioral adjuvant to improve the vaccine efficacy in the elderly.
Introduction
Physical inactivity accounts for 4% of global mortality [1]. Sedentary life has been limited to non-exercise physical activities in daily life with the coronavirus disease 2019 (COVID-19). Unfortunately, approximately 33% of the adult population worldwide is physically inactive. The decrease in physical activity became even more pronounced with the pandemic and resulted in physical inactivity or pandemic sedentariness [2]. According to current studies, COVID-19 should be entitled a “gerolavic” (from Greek, géros “old man” and epilavís, “detrimental”) disease [3]. Global statistics have shown that in the elderly aged 60 years and older, COVID-19 causes more severe symptoms and mortality [4]. The recent studies confirmed that there has been a dramatic decrease in their engagement in physical activity due to the pandemic therefore, there has recently been more concern for the elderly [5]. Therefore, several restrictions aimed at reducing social and physical contact have been especially risky for older patients prescribed therapeutic exercise programs.
Vaccination is a crucial precaution in decreasing the death and morbidity rates of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). However, the immune response elicited by the vaccine varies widely among individuals. Older individuals generally have lower immunogenicity against SARS-CoV-2 vaccines due to low immunity. This may be a reason for the immune response that varies between individuals. With age, immune function declines, and a process called immunosenescence. In this process, the function of dendritic and natural killer cells and the diversity and memory of B and T cells decline in adaptive and innate immune systems. In this context, immunosenescence increases the morbidity and mortality caused by viral and other infections in the elderly [6]. Ensuring the efficacy and safety of vaccination is crucial, especially for the most vulnerable population segment, such as the elderly. Higher doses of vaccines have been recommended to further enhance the immune response in older individuals [7]. Several COVID-19 vaccines have been reported to have over 90% efficacy in most adults (
Consort participant flow diagram.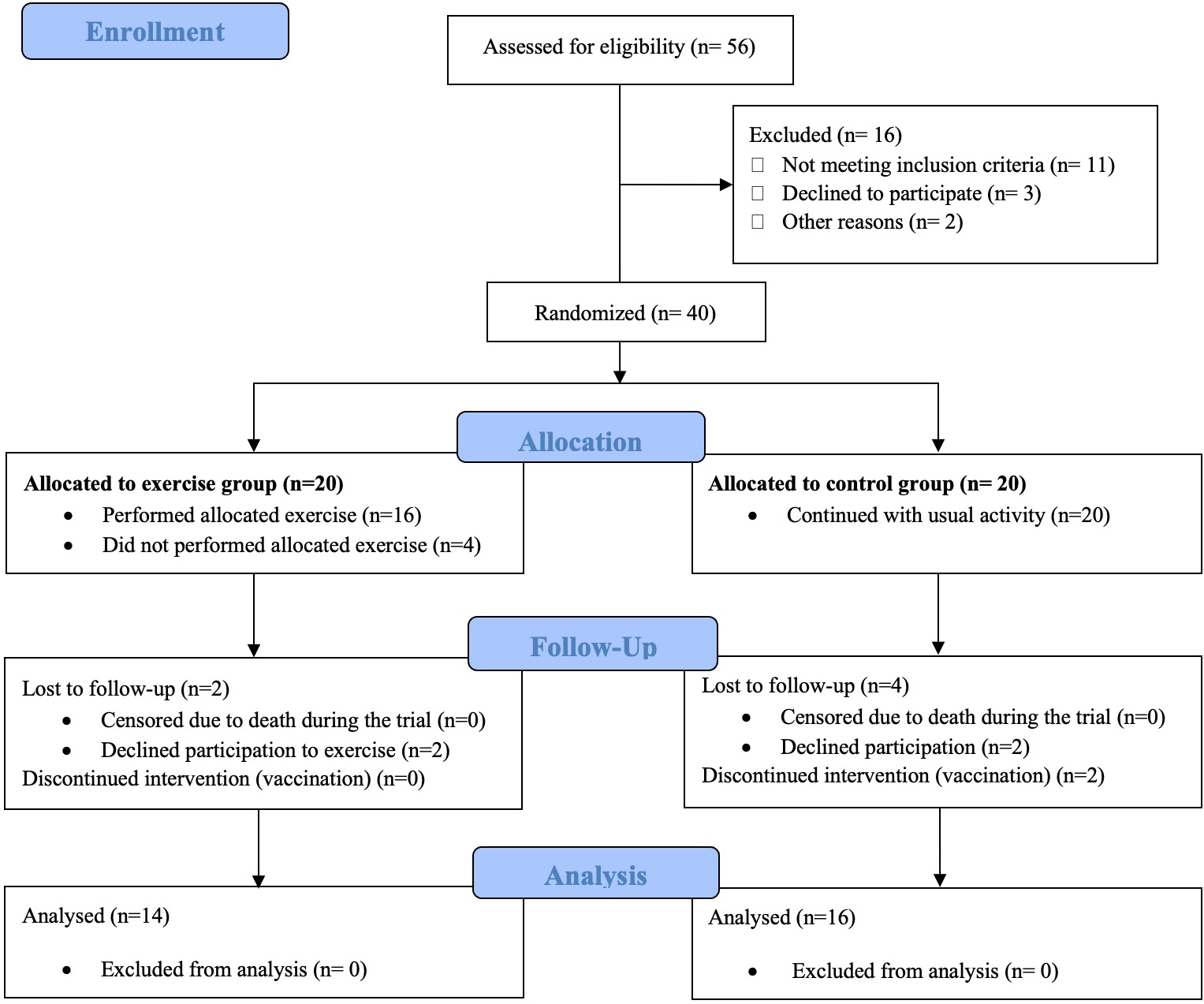
Enhancement of response to vaccines is provided by adjuvants. The addition of traditional exogenous adjuvants to the vaccine formulation remains important but carries the risk of side effects. In recent years, physical exercise has been proposed as a new alternative to chemical adjuvants. In the literature, physical exercise; as a “behavioral adjuvant” with low potential for side effects and low cost; has been suggested to strengthen the immune response [9]. Since the vaccination effectiveness varies between individuals, this inter-individual diversity of induced immune responses can be modified by physical exercise [10]. In recent years, randomized studies have been conducted on the efficacy of influenza, tetanus, meningitis, diphtheria, meningococcal or pneumococcal vaccines, and physical exercise. These studies showed that exercise before and after vaccination increased the titer of antibodies to the administered antigen [11, 12, 13].
Most of the studies presented in the literature have been conducted on young individuals who have a relatively stronger antibody response to the vaccine immunization. While physical activity does not contribute to an increase in antibody levels in young individuals, the effectiveness of vaccination in preventing hospitalization has been reported as 75% in young adults and 30–45% in the elderly. These results suggest that the older age population with reduced antibody response to vaccination may benefit more from physical exercise than the younger population with higher immunity [14]. In another study examining the immune response to physical exercise and vaccine in the elderly population, it was reported that immunoglobulin M (IgM) and immunoglobulin G (IgG) antibody levels and immune response to influenza vaccine were higher in physically active individuals [15]. In addition, 12 weeks of cardiovascular exercise has been shown to amplify influenza vaccine seroprotection in physically inactive the elderly population [16]. Studies focusing on the impact of physical exercise training on the immune response in the elderly have often been demonstrated with longitudinal randomized controlled trials (RCTs) to document immune response changes, or with a cross-sectional model to distinguish between physically active and inactive individuals. The most commonly used exercise protocols are aerobic or resistance training (or a combination of both, i.e., simultaneous strength and endurance exercises) ranging from 8 weeks to 12 months. Nevertheless, there is still a gap in studies examining the impact of cognitive exercise on the immune system in the elderly population [3].
In this exploratory study, regular aerobic physical exercise for the elderly was proposed as a potential “behavioral” adjuvant in COVID-19 vaccination [17]. This possibility was evaluated after the phase 2 vaccination trial of the elderly population. A stressor administered after vaccination has been shown to increase the antibody response to the vaccine [18]. Therefore, unlike other studies focusing on pre-vaccine exercise, we tested whether regular exercise after the second dose of an inactivated COVID-19 vaccine could enhance immunogenicity in the elderly.
The study was conducted at the private MEVA nursing home and Medical Biochemistry department of NP Istanbul Brain Hospital, from May to July 2021. A total of 40 individuals who received the inactivated COVID-19 vaccine were enrolled and 30 participants were included in the final analysis as depicted in the CONSORT diagram (Fig. 1). G*Power software version 3.1.9.4 was used to determine the number of subjects before conducting the study. The power analysis revealed that the minimum number of subjects required in this study to find a statistically significant difference between the two groups was 14 participants for each group (A type I statistical error is 0.05 and power is 0.80) [19]. Informed consent was obtained from all individual participants included in the study. The project was approved by the Uskudar University, Clinical Research Ethics Committee (no: E-99102440-/2021-13) Inclusion criteria were defined as being 65 years of age or older, accepting and signing the voluntary consent form, and receiving the COVID-19 vaccine. Exclusion criteria were having an immune system disease, having any medical condition that may directly affect immune outcomes, including autoimmune disorders, and being unable to exercise for any reason. After consent, all participants were randomly assigned to one of two groups: no exercise, or 45 min of exercise. To ensure unbiased randomization, participants who met the inclusion criteria voluntarily were listed on slips of paper and placed into a container. The slips were then picked at random by an evaluator using a lottery system to form groups. The experimental group received a 12-week exercise program. The control group was followed up without any exercise. The exercises were performed daily in the form of sessions of 45 minutes on average accompanied by a physiotherapist. The day on which the second dose of the vaccine was administered to all participants was considered day 0. All participants were instructed to go about their daily routine but avoid exercise on the day of the second vaccination.
Exercise program applied to the participants
Exercise program applied to the participants
[min:minutes].
The exercise task was performed in sets of 5 minutes of warm-up, 35 minutes of exercise, followed by 5 minutes of cool-down exercises. Participants performed four exercise movements sequentially; calisthenic, walking, balance, and stretching exercises. Each movement was performed with instruction and encouragement to perform “as many as you can”. The exercise program applied to the participants is indicated in Table 1.
Blood was collected in a 10 ml plain vacutainer 15 days and 12 weeks after the second dose of vaccination. Samples were stored on ice until centrifugation (3000 rpm, 10 min, 4
Demographic statistics, mean
The adaptive humoral immune response level was detected semi-quantitatively in plasma samples. During electrochemiluminescence immunoassay (ECLIA) the measurements, and standard procedures suitable for the kits (09289267190, Roche Diagnostics, Rotkreuz, Switzerland) were followed. The results were measured with cobas e411 analyzer (Roche, Mannheim, Germany). All samples were evaluated according to the manufacturer’s instructions. The results were given in U/ml. The cut-off point was determined as 0.80 U/ml to distinguish sample reactivity. The samples above
SPSS 25.0 (Statistical Package for the Social Sciences) program was used in the analysis of the data. The distribution of variables was analyzed using the Shapiro-Wilk test. The comparison of groups was examined using an independent
Participants had a mean (SD) age of 78.5 (9.3) years, and a BMI of 23.3 (2.61) kg/m2. 22 of the participants were female and 8 were male as shown in Table 2. Antibody levels (including IgG) raised against the SARS-Cov-2 spike (S) protein receptor binding site in plasma samples were detected after immunization. The mean antibody level in the control group was 69.4 U/ml 15 days after the vaccination, but 56.4 U/ml 12 weeks after the second vaccination. The mean antibody level in the exercise group was 74 U/ml 15 days after the vaccination, but 71.6 U/ml 12 weeks after the second vaccination (Fig. 2).
Mean antibody levels at 15 days and 12 weeks after vaccination in the exercise and control groups.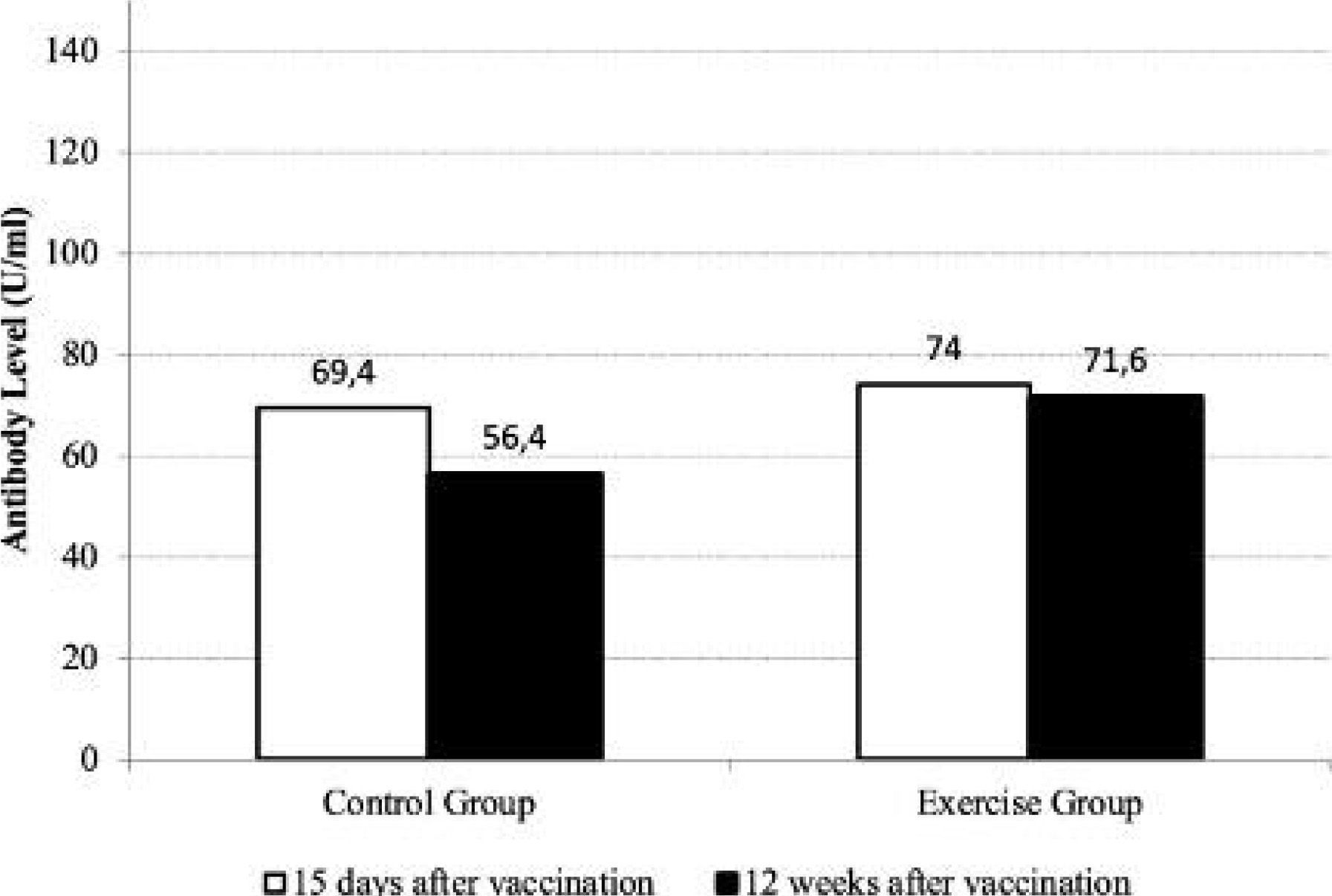
Aging is associated with high morbidity and mortality rates for various infections and a significant decrease in vaccine efficacy due to a decrease in pathogen immunity [20]. Physical exercise has been proposed as a “behavioral adjuvant” to strengthen the immune response [9]. Therefore, the potential “behavioral adjuvant” role of physical exercise in increasing the efficacy of the COVID-19 vaccine in the elderly was tested in this study. This randomized controlled study aimed to investigate whether an exercise after the second dose of a SARS-CoV-2 inactivated vaccine could enhance the immune response in the elderly.
Most of the previous studies have examined the effect of pre-vaccine exercise on antibody response [21, 22]. In this study, the effect of standard aerobic exercise applied after vaccination was evaluated, unlike other studies. In the stress and immunity literature, it has been shown that a stressor administered after vaccination increases the antibody response to vaccination [18]. Therefore, we evaluated the effect of exercise on antibody response when administered after immunization. We evaluated 45 min of exercise since the aged adults may be more readily able to complete 45 min of light-intensity exercise instead of 90 min [23]. The automated, high throughput Anti-SARS-CoV-2 S (ACOV2S) assay detects and quantifies antibodies against the receptor binding domain (RBD) of the S protein. We studied the antibody concentration, as measured by the automated, high throughput ACOV2S assay over time over time after the second dose of the inactivated COVID-19 vaccine [24].
Scientific data show that regular exercise, a low-cost and non-pharmacological treatment approach, induces cell rejuvenation mechanisms in the elderly. It has been observed that physical exercise has a telo-protective effect, affects telomere length dynamics, regulates short- and long-term anti-inflammatory response, and stimulates the adaptive immune system. It has also been suggested that physical exercise inhibits the immunosenescence process, enhances post-vaccination immune responses, and possibly extends both health and lifespan. On the other hand, it has been shown that exercise does not provide benefits for boosting the immune response [25]. In another study, a positive effect of exercise was observed in the formation of an immune response against an antigen in the vaccine, while no effect was observed on the response to other antigens in the same vaccine [26]. Considering the inconsistencies between studies, it has been suggested that the effect of exercise can only be observed in conditions where the antigen dose is low or when participants have a decreased antibody response [27]. Current findings suggest that the effect of exercise is smaller compared to the immune stimulus produced by the vaccine. Therefore, it may be difficult to determine the effect of exercise on the antibody response. Although no statistically significant difference was found in this study, it was observed that exercise protected the level of antibodies developed in the body against the COVID-19 vaccine. Antibody response, which was expected to decrease over time, was better preserved in the exercise group compared to the control group. This showed that exercise may preserve the antibody response developed after vaccination for a longer period of time. Also, the effectiveness of the exercise-induced antibody response may depend on the physiological variables that develop in the elderly. Therefore, it is crucial to identify exercise parameters that improves the antibody response to advance the concept of exercise as a vaccine “behavioral adjuvant” from a public health perspective. In the future, classification of physical activity prescription in terms of dose and intensity will be important in determining age-related diseases in which physical activity may be effective.
There were some limitations in this study. In the current study, we also did not experimentally control pre-vaccination antibody levels. We did not perform a detailed immunological assessment; therefore, we were unable to address the basic modulations and mechanisms of the immune system after regular moderate-intensity aerobic exercise in the elderly.
Conclusion
Existing literature reports that physical activity is applicable as an adjuvant to immunotherapies such as immune cell therapy and vaccination. In this study, we suggest that regular exercise of light to moderate intensity may extend post-vaccination antibody response in the elderly. Exercise programming in the sedentary elderly population may enhance the vaccine seroprotection.
Footnotes
Acknowledgments
This study was supported by Üsküdar University Scientific Research Projects Unit (ÜÜBAP-YP-2021-003).
Conflict of interest
None.
Author contributions
Conception: Ö. Ş.
Methodology: Ö. Ş, S.Ö.
Data collection: Ö. Ş, S.Ö.
Interpretation or analysis of data: Ö. Ş.
Preparation of the manuscript: Ö. Ş.
Supervision: Ö. Ş.