
Abstract
Most common asymptomatic arrhythmia that significantly leads to death and morbidity is Atrial Fibrillation (AF). It has the ability to extract valuable features is necessary for AF identification. Still, many existing studies have relied on weak frequencies that, are Time-Frequency Energy (TFE) and shallow time features. It requires lengthy ECG data to confine the information and is unable to confine the slight variation affected by the previous AF. The interfering noise signals focus primarily on separating AF from signals with a Sinus Rhythm (SR). Thus, this study would explore the detection of AF with heuristic-assisted deep learning approaches. Initially, the ECG Signals are gathered from the standard resources. Next, these gathered signals are pre-processed to perform denoising and artifact removal for enhancing the quality of data for further processes. Then, the deep feature extraction is done in two phases. In the first phase, the RR interval is extracted from the pre-processing ECG signals and the deep features are removed utilizing a Convolutional Neural Network (CNN). In contrast, deep features are employed to extract the features from the pre-processed ECG signals using the same CNN in the second phase. Then, these gathered in-depth features are fused and fed to the newly suggested heuristic algorithm called Enhanced Average and Subtraction-Based Optimizer (E-ASBO) for selecting the optimal fused features for reducing the redundancy in the signals. Finally, the chosen optimal fused features are fed to the new Adaptive Ensemble Neural Network (AENN) with heuristic adoption with the techniques such as Elma Neural Network, Deep Neural Network (DNN), and Recurrent Neural Network (RNN). This model focuses on increasing the accuracy of detecting AF. These proposed networks have more significant potential in future AF screening or clinical computer-aided AF diagnosis in wearable devices. It has superior performance and intuitive nature compared to the existing works.
Keywords
Introduction
A fast-growing arrhythmia, AF, is usually caused by an abnormal heartbeat [1]. Identifying AF earlier is paroxysmal because if AF occurs for more than one week, it is converted to constant AF. If it happens for a year, then it is converted to permanent AF, which causes heart failure, and stroke directly [2]. Still, one-third of the patients have AF, which is unidentified and symptomless, which highly enhances the risk of stroke and leads to the death of patients. To overcome this, earlier treatment and accurate diagnosis are essential, which help to prevent the risk of stroke [3]. However, it is symptomless because it depends on the identifiable hospital outside the scope, leading to danger. General AF detection contains ECG, oscillometric blood pressure, pulse palpation, and photoplethysmography. AF also causes stroke in cardiac irregularities [4]. Simultaneously, the combined mortality gets enhanced in the future decades [5]. AF is predicted by evaluating the ECG with extreme interest because the ECG recording has a lower cost and is non-persistent [6].
Various studies have involved analyzing the ECG to identify the AF automatically. The AF has some characteristics: absence of p waves, presence of fibrillatory waves, and abnormal R-R intervals [7]. Recently, these studies focused on the automatic detection of AF, where the ECG has been used increasingly [8]. Automatic AF detection has two significant challenges. It has distinguished AF accurately from other rhythms. The variation between the AF and normal sinus is evident, and the abnormal rhythms are difficult to find in detecting AF. The occurrence of cardiac arrhythmias is frequent, especially for patients with cardiovascular co-morbidities or grown-up patients [9].
The only approach to consistently serve is a 12-lead standard ECG recording as a standard tool to validate the AF among patients. Due to its low cost and ease of use, the ECG is a primary detecting tool often utilized in clinical practices [10]. Other approaches are sufficiently sensitive or specific for a precise diagnosis of AF. It is attached to the patient’s body with electrodes for a while and offers valuable information regarding the heart’s electrical activity [11]. The frequency domain, time domain, and some characteristics of ECG signals are seen in the human body [12]. Many algorithms are built on ECG features, which had considerable success recently for improving the efficiency of ECG signal analysis. Many of them currently rely on machine learning methods [13]. The critical component of the algorithmic structure is feature extraction. The Morphological Variant P-Wave (MVP)-Net deep learning model finds multiple perturbations between p-wave beats [14]. Deep learning classifiers are viewed as "black boxes" because they have difficulty presenting the predictive information to explain the diagnosis [15]. Conversely, arrhythmia identification utilized a new CNN algorithm, which has produced outstanding results with the help of ECG [16]. Only a tiny number of research studies have attempted to forecast AF events. The Post-Operative (Po) AF report is seen after cardiac surgery in patients with stroke, which is even more critical in identifying early AF in these difficult ECGs [17]. Hence, this paper presents a new goal concerning AF identification using the ECG and deep learning concepts for all those implanted techniques.
The significant contributions of this study are described as follows.
To build up a new AF detection model to find and detect AF in patients at an earlier stage with deep learning technology and provide appropriate treatment to protect the ordinary life of patients. To perform the optimal feature fusion by involving the weight optimization using the implemented E-ASBO to get the optimized fusion weighted feature to enhance the developed AF detection model. To set up the AENN-based AF detection with a group of classifier techniques such as DNN, ENN, and RNN for detecting the AF precisely with the parameter optimization using recommended E-ASBO. To establish a novel optimization algorithm named E-ASBO for tuning the parameters like many epochs in RNN and DNN, hidden neurons in DNN and ENN, a Learning rate of RNN, and weight in optimal feature fusion for increasing the performance of the suggested AF detection model. To observe and evaluate the suggested AF detection model by comparing it with the standard techniques and algorithms to validate the superior performance of the developed AF model.
The research work of this paper consists of many sections that are explained as follows. Section 2 described the related works and faced challenges in previous works. Section 3 presents the proposed AF’s architecture, dataset description of ECG signals, and artifact techniques. Section 4 describes the extraction feature of two phases of CNN and RR-Interval techniques and fused optimal feature selection method. Section 5 describes the novel E-ASBO model and the developed AENN model. Section 6 explains the result and discussions, and Section 7 explains the conclusion.
Related works
In 2022, Wesselius et al. [18] have suggested large datasets of actual ECGs, which were utilized to build a classifier for identifying AF. Two phases of semi-supervised learning were used semi-automated training phase and the pre-training phase. Segments were either automatically included in the training dataset or manually validated, depending on the level of assurance. The process was then repeated after the classifier had been retrained. The F1-score changed slightly during the semiautomated training phase, while the enlarged training dataset boosted the number of segments automatically identified during the training. The total F1 score have enhanced concurrently. Semi-supervised learning with human validation reduced training time without sacrificing accuracy. As a result, this technique could automatically detect AF in real-world ECGs.
In 2021, Wu et al. [19] have recommended the hybrid – CNN-Long Short Term Memory(LSTM )model and utilized a brief ECG signal from the dataset for examining and comparing the increasing performance of three deep learning architectures. The results demonstrated that the Hybrid CNN-LSTM model outperformed other benchmarked algorithms with correct design and tuning. Deep learning models could generally be utilized for automatic AF detection with exemplary architecture and implementation. The work was performed as a black box by most network models, which was challenging to identify the properties in the signal that were essential for analysis.
In 2021, Tzou et al. [20] have designed a deep learning technique for predicting AF risk and implemented a new Morphological Variant P-Wave (MVP)-Net for forecasting the awaiting paroxysmal AF beginning stage. A deep learning classifier and wavelet-based feature extraction were combined in MVP-Net. MVP-Net examined the pattern to identify the onset of AF. They evaluated the precision of AF prediction using neuECG versus conventional ECG. The MVP-Net successfully predicted the start of AF episodes. With fewer computational resources than previous models, the suggested deep learning model, MVP-Net, has outperformed in inference speed and precision. NeuECG recording could be a more accurate AF risk prediction, according to the gradient activation map. The SKNA, P-wave, and MVP parameters were integrated to increase the analysis. The suggested MVP-New was based on the new ECG and outperformed the current AF risk assessments, increasing effectiveness and dependability. For continuous, real-time AF prediction, the approach could be utilized in clinical scenarios.
In 2022, Jagdeep and Dev [21] have suggested a 1-D ECG signal was utilized to diagnose the AF. Before the signal was applied to AI-based models for classification, it underwent preprocessing by a least-square filter and a 2-stage median filter, followed by normalization. A bidirectional LSTM was trained and optimized to achieve greater accuracy. This method was suited for an automated, trustworthy, and earlier identification of AF since it utilized short-duration ECG signals rather than the existing methods and has higher accuracy.
In 2022, Geweid and Chen [22] have designed a novel Hybrid Approach of Dual Support Vector Machine (HA-DSVM) technique to find AF. The cross-entropy loss function is utilized in it. The technique was evaluated based on training results. These methods have yielded better accuracy and F1 score. One benefit of the suggested approach is that its reliability and accuracy were higher, which made removing hand-made features, identifying ECG signal fiducial points, and the extraction process more straightforward. To detect AF, this offered screening for a sizable population. The suggested methods have been used on a large population of people with AF symptoms, increasing the diagnostic precision and helping to identify the necessary treatment.
In 2019, Cai et al. [23] have suggested a unique method of deep learning with great accuracy for detecting the AF. The recommended way to identify AF in ECG waveforms provided a new 1-D deep Densely Connected Neural network (DDNN). ECG devices obtained a sizable collection of ECG recordings.DDNN dataset has performed well in accuracy, sensitivity, and specificity. The suggested networks have much potential for future AF screening or clinical computer-aided AF diagnosis in patients due to their excellent performance and intuitive nature.
In 2020, Wu et al. [24] have designed a novel three deep features that have captured the correct slight differences in brief ECG segments caused during the early AF. It analyzed noisy signals and presented a unique feature set for identifying the AF earlier. The performance is tested for determining the AF earlier, which utilized six well-known classifiers and the efficiency of the features, compared to the feature extraction by two traditional time-frequency approaches of time frequency. Extreme Gradient Boosting (XGBoost) produces the more significant results for categorizing four signal classes, with an overall F1 score.
In 2020, Wang [25] have suggested a unique model mechanism of 11-layer network architecture, which was utilized automatically classifying AFL and AF signals. The Improved ENN and CNN were primarily constructed in this method. In addition, it deliberately created two relative models as control subjects confirming the suggested model’s ability to data classifying. According to the results, the model’s specificity, sensitivity, and accuracy on the AFDB database were superior to the MITDB database. Therefore, it showed that the model mechanism performed better than some complicated algorithms and in two related models, which was taken as an efficient detection system and made more consistent for supporting surgeons to save the life of patients.
Model overview
Features and challenges of enhancing AF using ensemble learning techniques
Features and challenges of enhancing AF using ensemble learning techniques
This existing approach to AF was unable to achieve accuracy for AF detection. It faces some problems, especially with different types of data sets, unrobustness, and a lower ability for generalization. Therefore, deep learning is utilized to overcome the above issues, and some features and challenges have been overviewed in Table 1. Human-controlled semi-supervised algorithm [18] has accuracy and efficient time without satisfying the categorization. Hence, it does not consider more valuable when developing the classifier of real-life ECG data. LSTM [19] achieves better accuracy and robustness. It has been acquired with an enormous error rate for the parameters like learning rate, output, and input bias. MVP-Net [20] recommended that the analysis, combined with deep learning, provides excellent work on prediction and accuracy. It is affordable and easy to be used. This method also has the ability to identify patients with imminent AF with non-invasive and low-cost screening to maintain patients with unknown causes of stroke. But improving the MVNet methodology for the multi-scale vector space regarding the data augmentation was limited in this method. 1-D electrocardiogram [21] method provides better accuracy and utilizes short-duration ECG signals and reliable, automated, and timely detection methods. But the non-established data examines the clinical impact, inaccuracy, or higher cost. HA-DSVM [22] method has more reliability and high accuracy that make the extraction procedure, as well as the removal of detecting ECG signals, significantly more accessible, and it enhances the reliability of the AF diagnosis. But this method has not been executed well when the data set has more sound. DDNN [23] has shown the capability of the strong generalization of multi-center data. It is suitable for identifying the AF automatically and accurately. However, detecting hundreds of cardiac diseases on a single lead ECG is impossible. RF [24] technique has been effectively capturing the slight variations in AF signals earlier, and it improves the outcomes by utilizing good classifiers to identify the AF earlier. But it suffers from extracting the features that have characterized the ‘Other’ type that was limited in this method. 11-layers network architecture [25] is an end-to-end detection model and achieves superior outcomes than the other algorithms. But this technique still needs a significant and different database source for developing the model.
Proposed fibrillation detection
Increased risks of heart failure, stroke, and death are associated with AF. Additionally, AF typically lowers the patient’s Quality Of Life (QoL) frequently compared with those who have recently experienced heart failure or myocardial infarction. Consequently, more treatment choices for AF are made to enhance the patient’s QoL. The abnormal heartbeat indicates the symptoms of unintentional strokes, which can lead to ultimate heart failure and causes more severe disease. Therefore, earlier treatment is necessary to identify AF. The primary variation of heart rate is to confirm the existence of P-wave, and RR intervals are the emphasis of AF detection techniques. The performance of the ECG models has significantly improved the advancements in ECG data and the development of Dynamic Neural Networks (DNNs). The application of algorithms like CNN and LSTM can be directly trained on the large-scale dataset that meets the RR Intervals and the ECG signal requirements. However, CNN is more sophisticated and can determine the prediction using a tiny, straightforward pattern. The primary advantage of utilizing a CNN classifier is detecting the significant automatic features without human interaction. But machine learning can examine and combine unrelated information to predict outcomes with enhanced artificial intelligence technology and quick accumulation of digital healthcare data. Machine learning algorithms may be able to include and analyze vast volumes of clinical data as well as novel clinical patterns and concepts. They can help in obtaining electrocardiographic data or in processing images. The CNN and LSTM performance is combined throughout the training stage. The ensemble learning is required to increase accuracy. Hence, the suggested model developed an AF detection model using an ECG signal based on the ensemble learning strategy shown below in Fig. 1.
Suggested AF detection model utilizing deep learning techniques with ECG signals.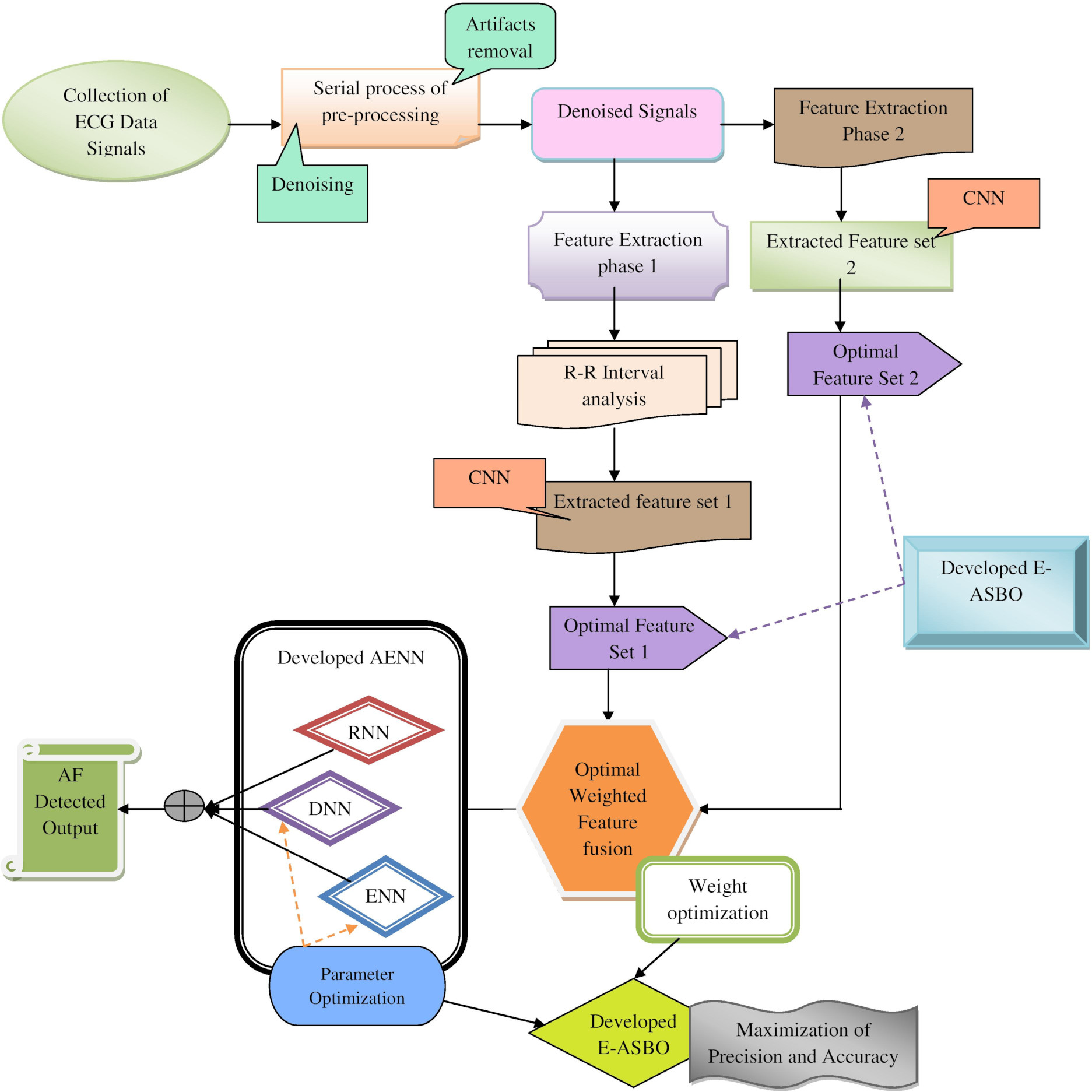
A recommended novel AF detection model employs ensemble learning techniques and optimization algorithms for supporting clinical practices like patient portals and hospital software applications. At first, the ECG signals are collected from the standard dataset. Then, the preprocessing technique is utilized to remove the artifact removal and denoising to get the denoised signal data. Next, there are two phases to extract the features: the feature extraction phase1 and the feature extraction phase 2. In feature extraction phase 1, the RR-Interval and CNN techniques are employed. The RR-Interval is utilized to get the RR-Interval data. After that, CNN extracts the feature set1 by processing the RR-Interval data In feature extraction phase 2, CNN is again utilized but extracts feature set 2 directly from the denoised signal data. At last, feature sets 1 and 2 are employed in the optimal featureweighted fusion phase, where the weight optimization takes place using developed E-ASBO. Here, the optimal features are selected from both the feature sets and selected features are given to the RNN DNN and ENN techniques for AF detection. These techniques are fused to develop the AENN by optimizing the constraints like hidden neurons of both DNN and ENN, the total epochs of DNN and RNN and the learning rate of RNN techniques utilized by the developed E-ASBO. The primary aim of this suggested model is to attain higher precision and accuracy in the developed AENN-based AF detection using the developed E-ASBO. Hence, the developed method has achieved superior performance than the traditional techniques verified through several experiments.
The recommended AF detection model includes the artifact removal phase and denoising process as the serial process in preprocessing that are mentioned as follows.
Artifact Removal Phase (ARP)[26]: In ARP, the suggested AF detection model utilized artifact removal as a preprocessing method, where the raw signal data
Denoising[27]: Here, the recommended AF detection model utilized denoising as the preprocessing method, where artifact removal
Experimented ECG data description
The suggested AF detection model utilized the standard datasets like MIT-BIH Arrhythmia Database and MIT-BIH Normal Sinus Rhythm Database, which are as follows.
Dataset 1 (MIT-BIH Arrhythmia Database): The necessary ECG signals are gathered from the link “
Dataset 2 (MIT-BIH Normal Sinus Rhythm Database): The necessary ECG signals are collected from the link “
The ECG signals are gathered from the standard datasets indicated by
Sample dataset for both normal and abnormal AF of ECG signals.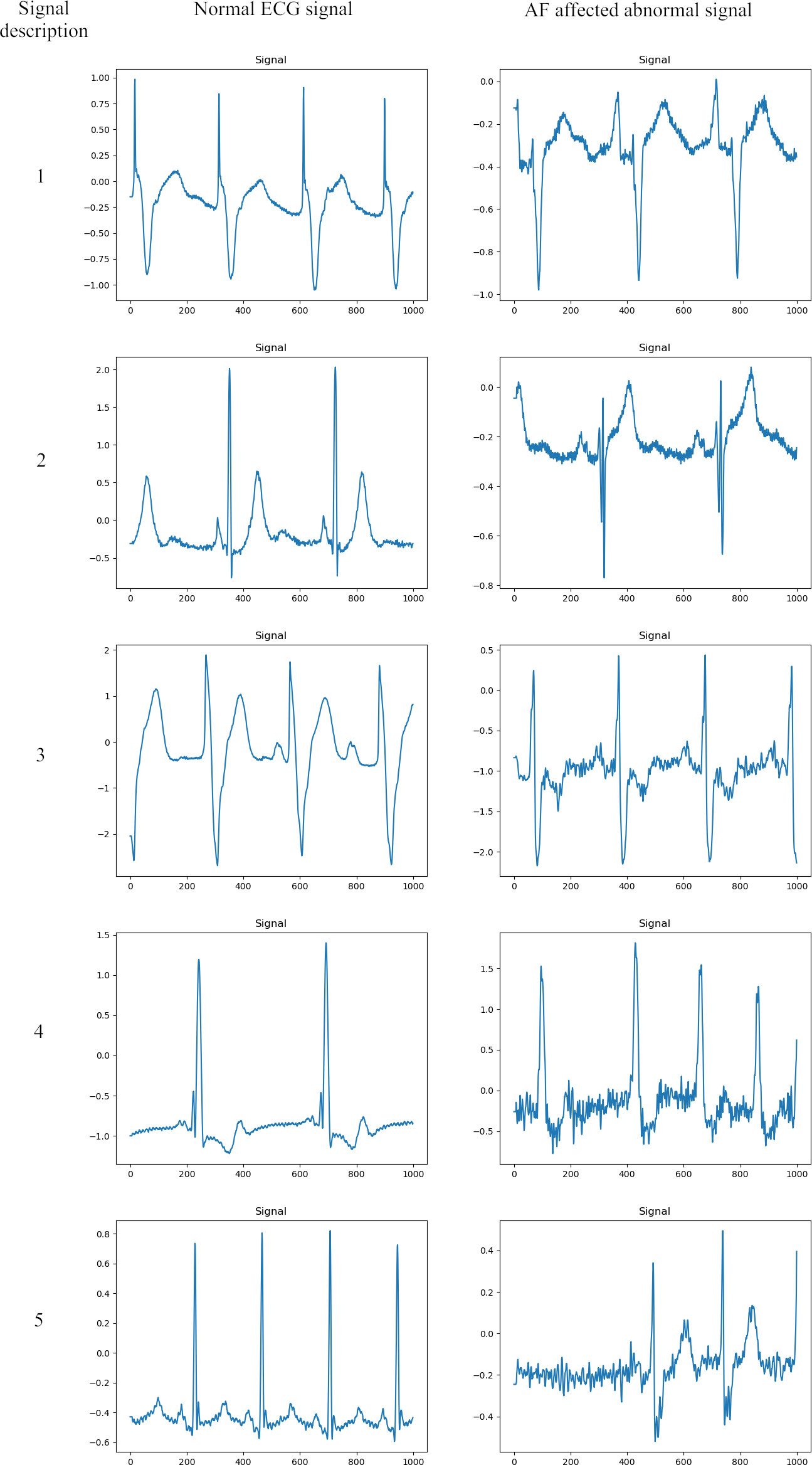
Feature extraction phase 1
The suggested AF detection model employs the RR-Interval and CNN as the feature extraction method in phase 1, which is explained as follows.
RR-Interval[28]: Here, the recommended AF detection model utilized the RR-Interval as the feature extraction method, where the denoised signal data
CNN[29]: Here, the recommended AF detection model utilized CNN as the feature extraction method, where the RR-Interval extracted data
Input layer: In this layer, the input layer is the primary input that upholds the information.
Convolutional layer: CNN’s fundamental core structure layer is the Convolutional layer. In this layer, the input data are convolved using convolution kernels, and the stride controls the kernels and verifies how long the input data kernels are convolved. The feature map is the alternative name for the related output. The input data is minimized, and this process is automatically extracted the valuable features from the original data.
Pooling Layer: It is a significant layer in CNN architecture. It is also referred to as the sub-sampling layer. It mainly consists of average and maximum pooling layers. The objective of passing input data to minimize the network’s computational cost while maintaining the necessary features by compressing the number of parameters. Additionally, the structure of this layer successfully resolves the over-fitting issue. Hence the output of CNN-based feature extraction is attained and represented by
In phase 2, the suggested AF detection model utilized CNN as the feature extraction method, where the denoised signal data
Optimal fused feature selection
The recommended AF detection model employs feature sets 1 and 2 as the feature selection process utilizing the developed E-ASBO. The recommended AF detection model uses E-ASBO to select the optimal features from feature set 1
At this time, the term
Dual feature extraction-based optimal weighted feature selection model for AF detection.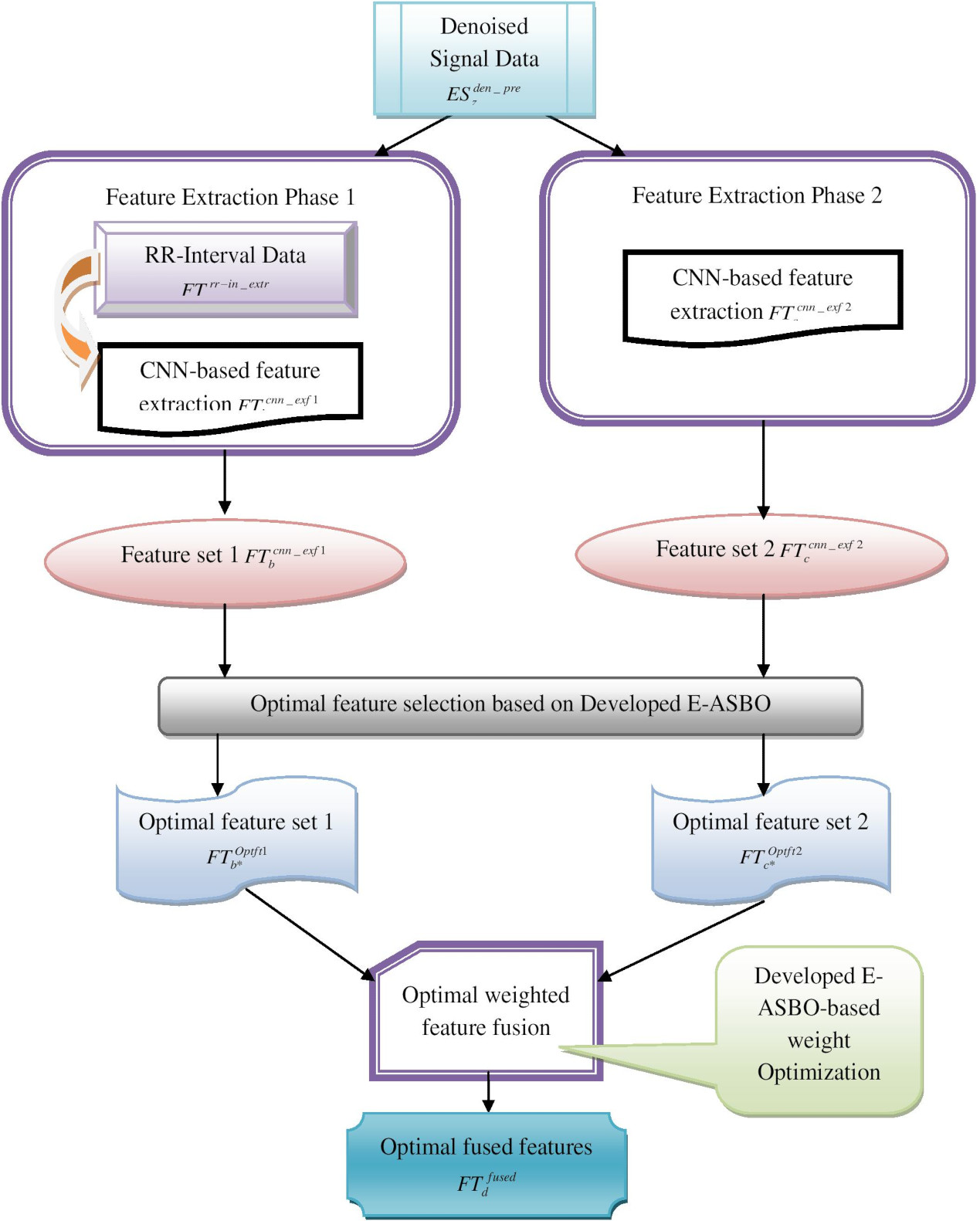
Proposed E-ASBO
The recommended AF detection model with ECG signals develops E-ASBO for tuning the parameters like weight optimization in optimal feature fusion, the learning rate of RNN, total epochs of RNN and DNN, and hidden neurons in DNN and ENN techniques for improving the precision and accuracy rate of AF detection. ASBO [30] is employed in this suggested model since it has some merits. It solves different optimization problems and maintains an accurate balance between exploitation and exploration to provide the optimal solution. However, it has particular disadvantages, and it is difficult to solve complex real-time problems. So, the new ensemble algorithm named AENN is developed. In this proposed E-ASBO, the random number is adaptively computed with the fitness-based concept represented by the term
Here, the maximum iteration is denoted by
In ASBO, the members based on the population are moving to the optimal areas based on an iterative process. The primary objective of this suggested ASBO algorithm is upgraded the position based on the members of the population. Every population member has a possible result for the optimization problem in ASBO. In ASBO, total elements are similar to the total decision variables. Every component defines the variable value to which it is assigned. In ASBO, the members are denoted in Eq. (3).
Here, the candidate solution of the ASBO is denoted by
Every search member of ASBO is the possible result to resolve the stated crisis. The function objective is assessed by including every clarification in the decision variables in the difficulty formulation. It yields a value for the function objective respective to each ASBO member. A vector is used to model the collection of these values following Eq. (4).
Here, the function objective value respective to the
ASBO goes through three stages for upgrading the algorithm population, in which the target is to enhance the candidate solutions. A best and worst members of ASBO, in which the ASBO population has updated by population members. The ASBO phases are given as follows.
Here, the term
The second phase is upgraded with the position of the population members using data from the worst and best population members of subtraction. The ASBO in phase 2 is denoted in Eq. (8).
Here, the term
At last, the best member is attained in the third phase of ASBO to guide the population towards better solutions. The updated process step in ASBO is indicated in Eqs (11) and (12).
Here, the objective function is denoted by
Flowchart for the developed E-ASBO.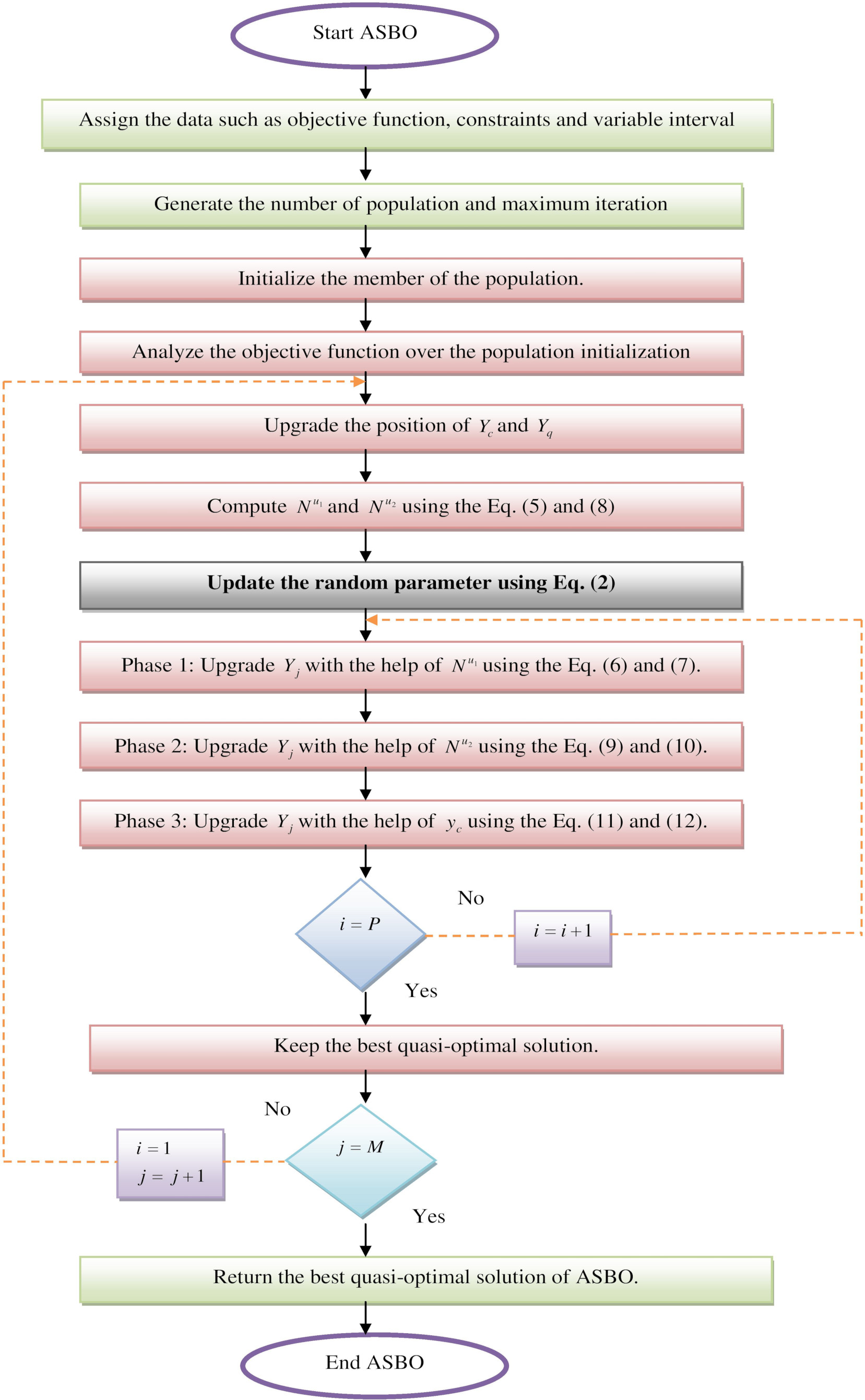
The flowchart for the designed E-ASBO is given in Fig. 4.
The suggested AF detection model employs three ensemble neural network techniques for the developed E-ASBO with the input optimal fused features
ENN[31]: ENN is suited accurately to handle time sequences and has many precise non-linear mapping functions. Its network structure is divided into four sections: an input layer, a context layer, an output layer, and a hidden layer. In conventional BP feedforward networks (FFN), units of context are added in it to allow the outcome of the current hidden layer moment that is used to store and provide feedback to the present moment. Thus, the model has a temporary memory function and is highly sensitive to previous data. The formation of the Conventional ENN model is represented under the equations.
Now, the term
RNN: RNN [32] is developed for utilizing a time-series data model. The RNN is the same as FFN, which are enhanced recurring loops. Information is transferred from one place to the other place. It is calculated based on the before and current value. RNNs can learn temporal patterns, typically accept the input sequence
Now, the term
DNN[33]: There are three main components in the architecture of the DNN framework: an input layer, an output layer, and hidden layers. The DNN has upgraded the node weight in the hidden layer during the training phase. The training iterations are enhanced because the neural network is fitted frequently in the labeled information. It built to increase the accurateness and performance of the DNN. The whole hidden layer nodes are analyzed by using Eq. (18).
Here, the term
Here, the term
Here, the term
The recommended AF detection model with ECG signals utilizes the ensemble technique called AENN to identify the AF to save the life of AF-affected patients. In developed AENN, DNN, RNN, and ENN are the techniques employed in detecting AF. DNN [33] is used to learn complicated features and perform computational tasks. The cost is lower when compared to the other techniques. It needs more data to enhance the performance, and it is challenging to train many data. RNN [32] is suitable for temporal and sequential data. It is utilized in the prediction of time series. Since it also faces some vanishing gradient problems, it is challenging to train the data. ENN [31] can produce dynamic time features and has more robust global stability. However, it has a low convergence speed and a fixed learning rate. Hence, a novel ensemble technique named AENN is developed to detect the AF by tuning the parameters like the learning rate of RNN, hidden count in DNN and ENN and the total epochs in RNN and DNN for increasing the detection rate. The function objective of the AF detection is given in Eq. (21).
Here, the DNN hidden count is represented by
Now, the term PQ and RS denotes true positive and negative values, respectively. At the same time, the term HJ and HI denotes the false negative and positive values, respectively. The precision
The architectural representation of the developed AENN for the AF detection model is shown in Fig. 5.
Developed AENN-based AF detection architecture.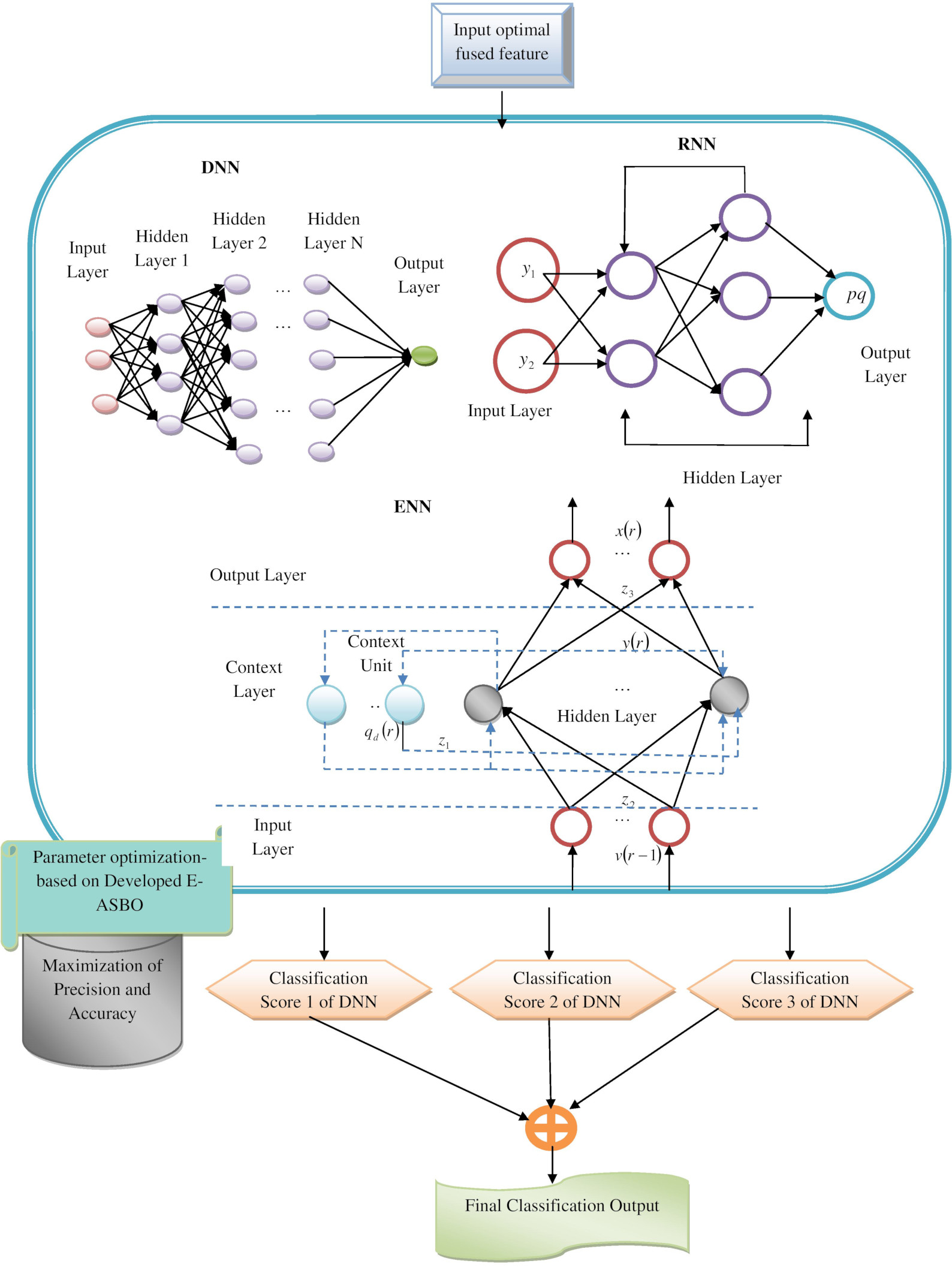
Experimental setup
Diverse experimental evaluations have been conducted for the recommended AF detection model, performed with Python. The population length and the enhanced iteration length are 10. The total length of the chromosome was 27. From 27 chromosomes, the first twenty were used as features, one as a weight, and six as parameters. The evaluation was performed with different existing detection methods. The algorithms such as Deer Hunting Optimization Algorithm (DHOA)-AENN [34], JAYA-AENN [35], Butterfly Optimization Algorithm (BOA)-AENN [36], Advanced Backtracking Search Optimization Algorithm (ABSA)-AENN [37] and the developed E-ASBO-AENN were measured with the previous algorithms such as RNN-DNN [38], RNN [32], DNN [33], Gated Recurrent Unit (GRU) [39], and LSTM [40]. Different analyzes employed for both dataset 1 and dataset 2 are described in the below sections.
Performance metrics
The suggested AF detection model is measured under various performance metrics shown below.
(a) F1-scoure
(b) NPV npv that is indicated in Eq. (25).
(c) FPR fpr that is denoted in Eq. (26).
(d) FNR fnr that is indicated in Eq. (27).
(e) MCC mcc that is represented in Eq. (28).
(f) Specificity spe that is depicted in Eq. (29).
(g) Sensitivity sensi that is represented in Eq. (30).
(h) FDR fdr that is depicted in Eq. (31).
Performance evaluation on suggested AF detection model over diverse algorithms for dataset 1 for (a) Sensitivity, (b) NPV, (c) FPR, (d) FDR, (e) Accuracy, (f) Specificity, (g) Precision, (h) MCC, (i) F1-Score and (j) FNR.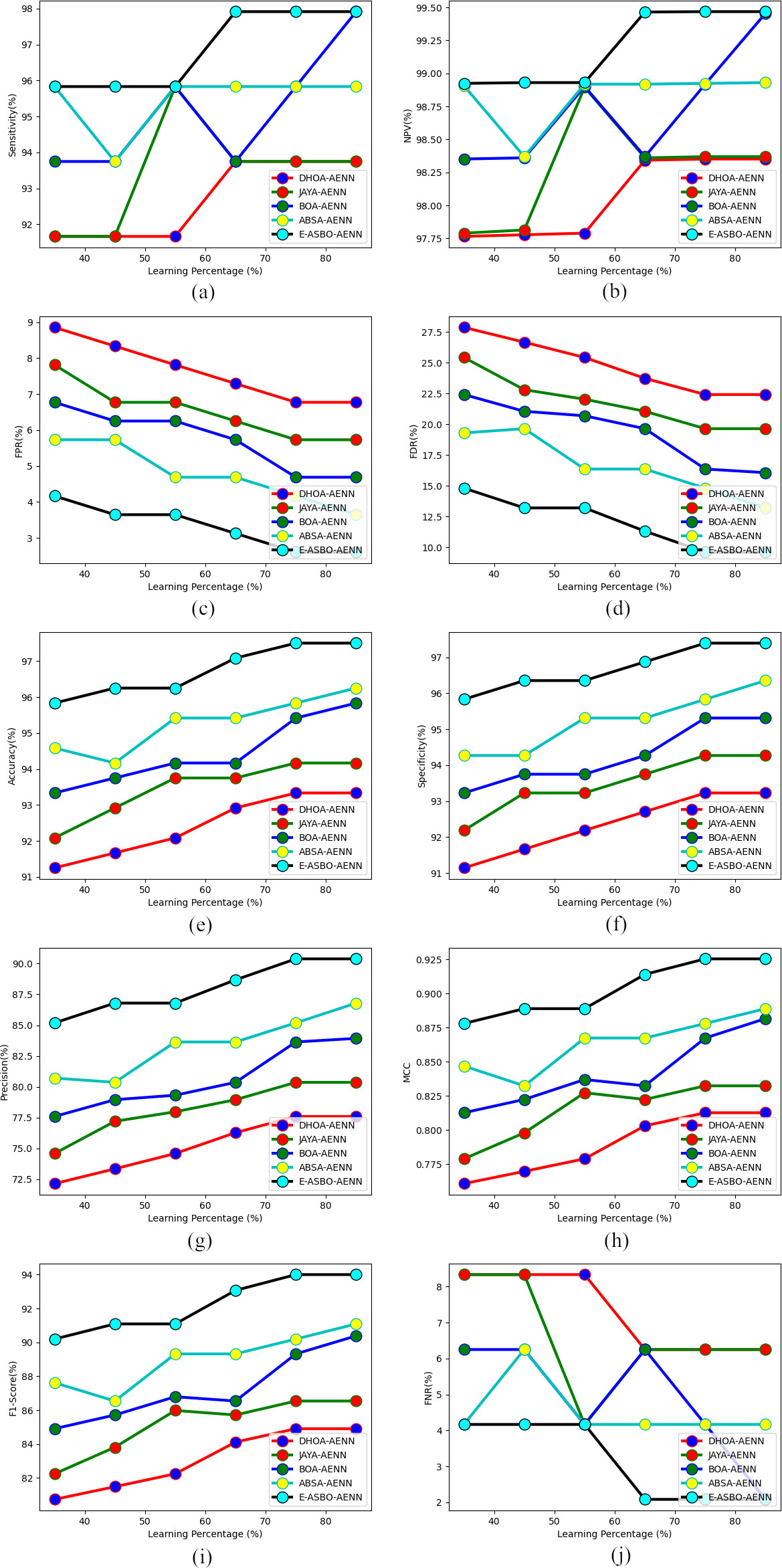
Performance evaluation on the recommended AF detection over diverse algorithms for dataset 2 for (a) Sensitivity, (b) NPV, (c) FPR, (d) FDR, (e) Accuracy, (f) Specificity, (g) Precision, (h) MCC, (i) FNR and (j) F1-Score.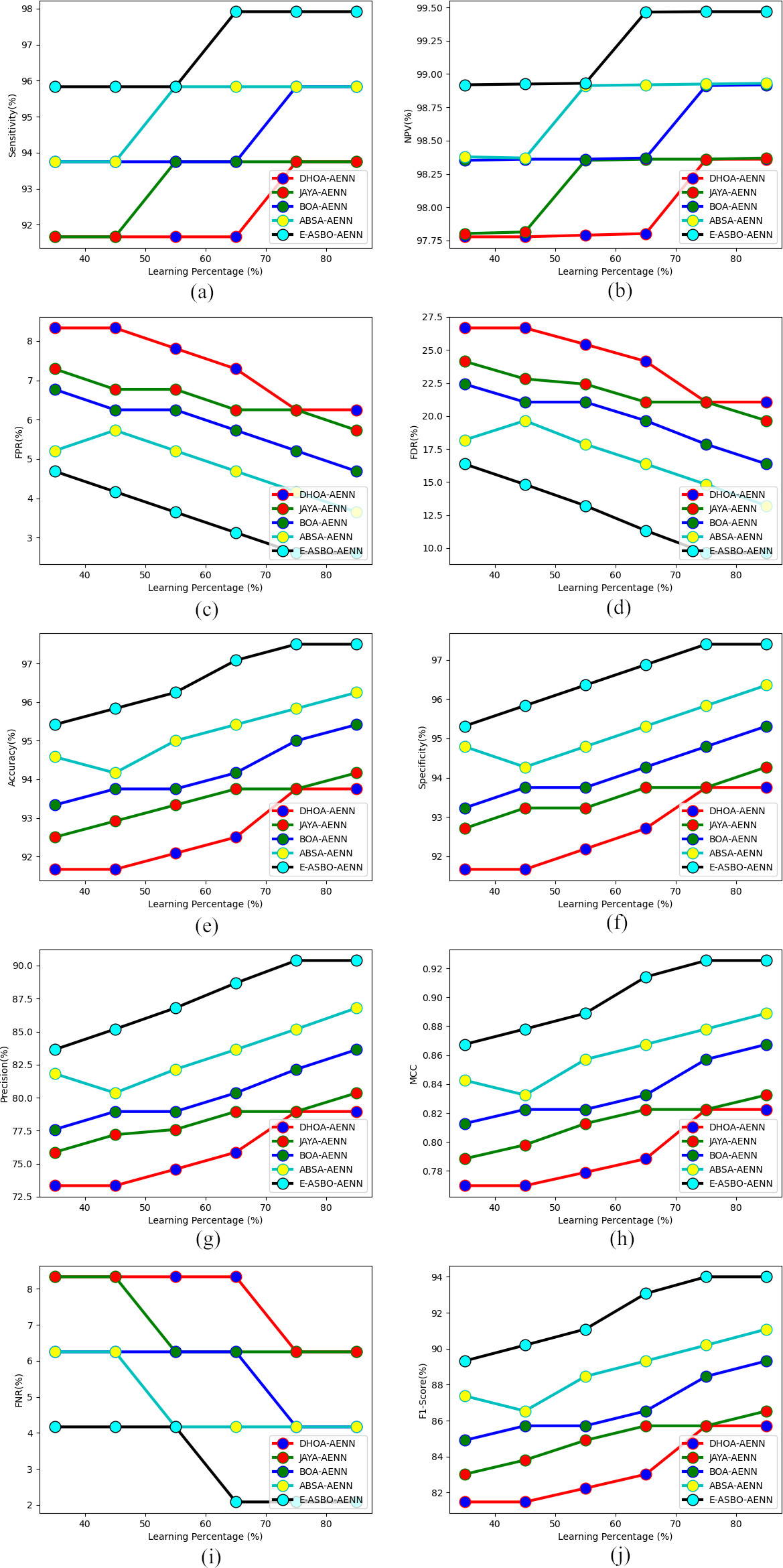
The suggested AF detection model is performed with diverse heuristic algorithms for both dataset 1 and dataset 2, that is shown in Figs 6 and 7. The developed E-ASBO is higher than the traditional algorithms observed in positive and negative measures. The sensitivity performance of the developed E-ASBO has 12%, 5%, 12%, and 5% superior performance compared to the previous algorithms. In dataset 1, the developed E-ASBO detects AF more accurately than the DHOA-AENN, JAYA-AENN, BOA-AENN, and ABSA-AENN. At the same time, in dataset 2, the suggested model has higher accuracy. As a result, the suggested model attains better performance compared to the previous methods over the different algorithms for AF detection.
Performance evaluation on the recommended AF detection model over diverse classifiers for dataset 1 for (a) Specificity, (c) Precision, (d) NPV, (e) MCC, (f) FPR, (g) FNR, (h) FDR (i) F1-Score and (j) Accuracy.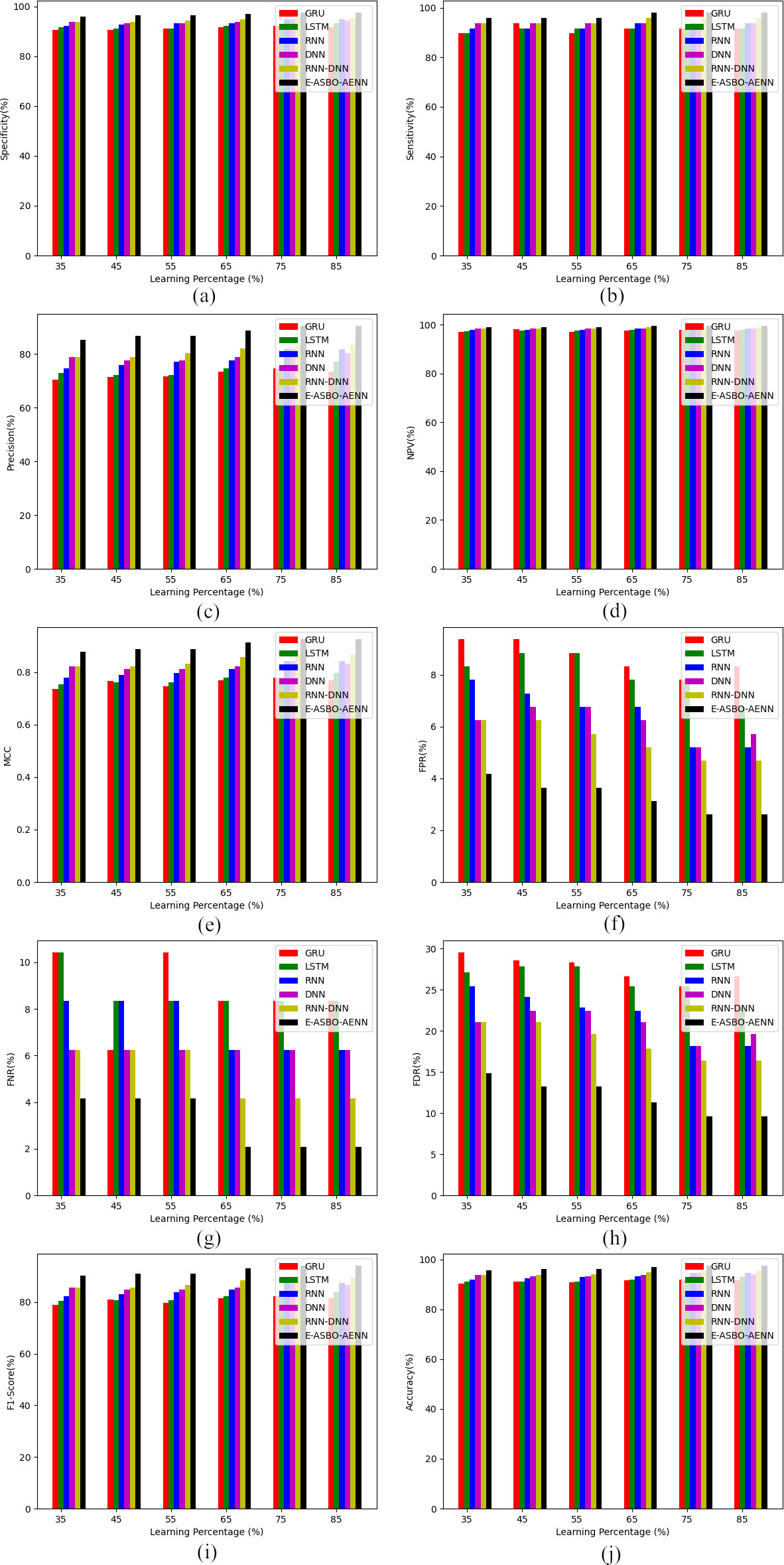
Performance analysis on the recommended AF detection over diverse classifiers for dataset 2 for (a) Specificity, (c) Precision, (d) NPV, (e) MCC, (f) FPR, (g) FNR, (h) FDR (i) F1-Score and (j) Accuracy.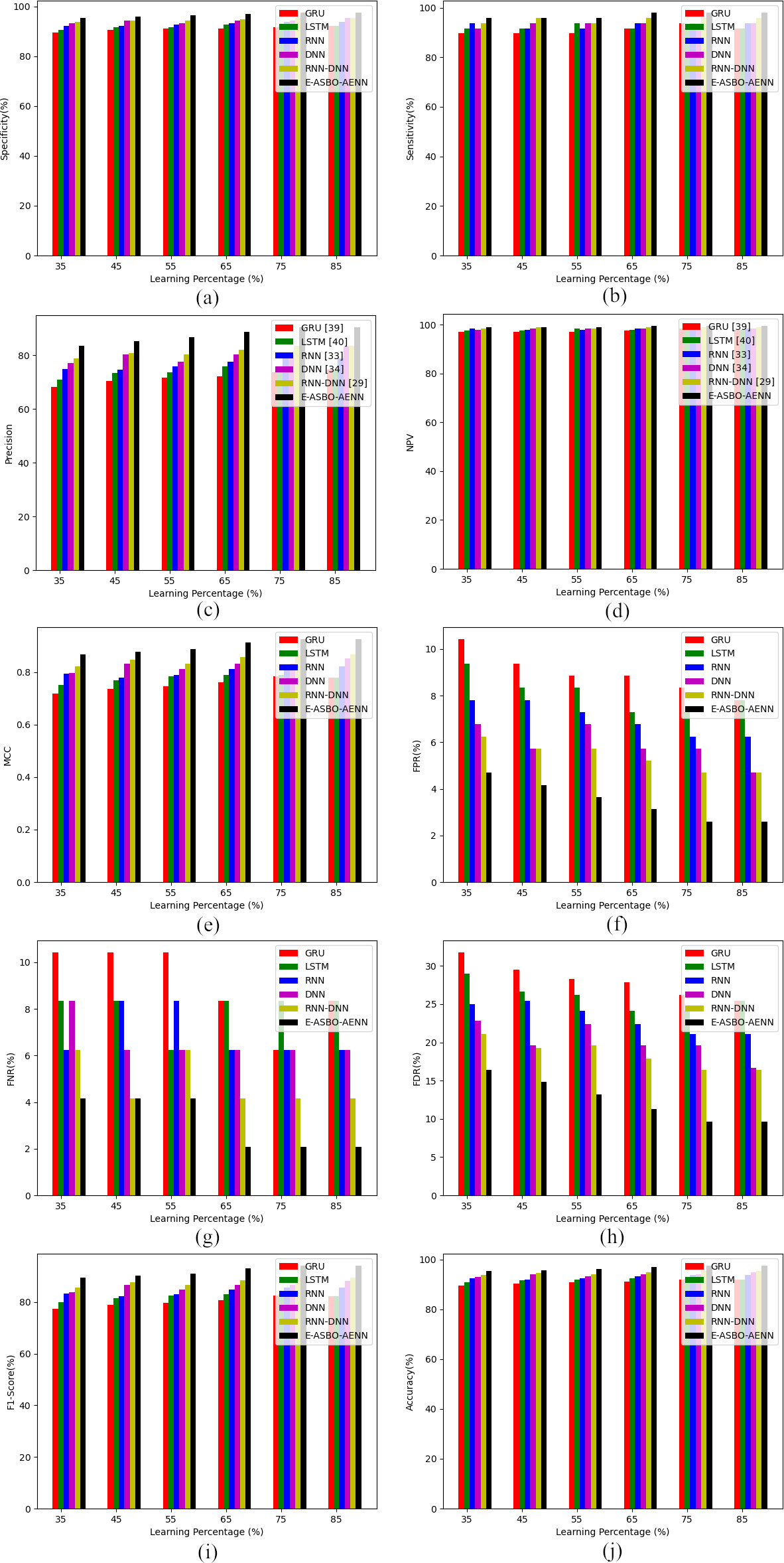
The suggested AF detection model is analyzed with various classifiers for both dataset 1 and dataset 2, that is given in Figs 8 and 9. The developed E-ASBO is greater than the other classifier techniques observed in both positive and negative measures. The MCC of developed E-ASBO has 10.4%, 10.5%, 10.6%, and 10.7% better performance compared to the existing methods. In dataset 1, the developed E-ASBO is more accurate than the RNN-DNN, RNN, DNN, GRU, and LSTM classifier techniques. In dataset 2, the MCC of the suggested E-ASBO is better than the RNN-DNN, RNN, DNN, GRU, and LSTM classifier techniques. As a result, the proposed model attains superior performance compared to the previous AF detection methods.
Overall performance evaluation of the suggested AF detection model over diverse algorithms for both datasets 1 and 2
Overall performance evaluation of the suggested AF detection model over diverse algorithms for both datasets 1 and 2
Overall performance evaluation of the suggested AF detection model over diverse classifiers for both datasets 1 and 2
The overall efficiency of the enhanced AF detection model is observed with dataset 1 and dataset 2, shown in Table 2 for algorithm analysis. Similarly, classifier analysis is shown in Table 3. In dataset 1, the proposed E-ASBO-AENN outperforms better sensitivity of 4%, 2%, 4%, and 2% than the DHOA-AENN, JAYA-AENN, BOA-AENN, and ABSA-AENN algorithms. Similarly, the accuracy of the developed E-ASBO-AENN outperforms 3.4%, 2.6%, 3.4%, and 2.6% of the RNN-DNN, RNN, DNN, GRU, and LSTM in the accuracy analysis by considering dataset 2. Hence, the suggested AF detection model is analyzed and achieves superior performance compared to the earlier techniques utilized by E-ASBO-AENN for AF detection.
Computational time of the offered model using algorithms
Computational time of the offered model using algorithms
Computational time of the offered model using classifiers
Validation of training vs epochs of the designed AF detection model.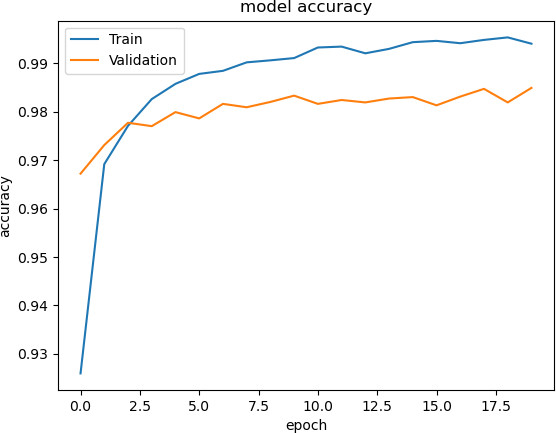
The performance of the designed AF detection model is validated based on training accuracy vs epochs, and it is shown in Fig. 10. Here, the graph analysis of training accuracy vs epochs is validated to show the effectiveness of the designed model.
The computational time of the recommended AF detection model regarding algorithms and classifiers is tabulated in Tables 4 and 5. Throughout the analysis, the developed AF detection model shows better performance than the other existing approaches.
Conclusion
Thus, this paper has employed a novel AF detection model with heuristic-assisted deep learning approaches. Initially, the ECG Signals were gathered from the standard resources. Next, these gathered signals were pre-processed for performing denoising and artifact removal for enhancing the quality of data for further processes. Then, the deep feature extraction was done in two phases, wherein the first phase, the RR interval, was extracted from the ECG signals pre-processed data, and the deep features were extracting CNN. In contrast, deep features were removed from the ECG signals using the same CNN in the second phase. Then, these gathered deep features were fused and fed to E-ASBO to select the optimal fused features to reduce the signals’ redundancy. Finally, the chosen optimal fused features have been provided to the new AENN with heuristic adoption, where the hyperparameters of DNN, ENN, and RNN techniques to develop E-ASBO. The performance analysis has attained 4% better than DHOA-AENN, 2% improved than the JAYA-AENN, 4% enhanced than the BOA-AENN, and 2% improved than the ABSA-AENN when comparing with dataset 1. Hence, the suggested AF detection model has achieved better precision and accuracy using the developed AENN with utilized recommended E-ASBO algorithm.