
Abstract
BACKGROUND:
The ergogenic effect of ischemic preconditioning (IPC) has been widely approved, but the mechanisms underlying the beneficial effects are still not fully clarified.
OBJECTIVE:
The aim of this study was to examine the effects of IPC on human isokinetic muscular function and hemodynamics during exercise.
METHODS:
In a counterbalanced, crossover study, 14 healthy non-athletic males (26.0
RESULTS:
Resting total hemoglobin significantly increased after IPC (
CONCLUSION:
IPC improves the local oxygenation status without altering maximal muscle strength and endurance in young non-athletic males.
Introduction
Ischemic preconditioning (IPC), which consists of non-lethal episodes of ischemia and reperfusion via a pressure cuff on skeletal muscles, provides protection of muscle cells in the heart and other organs against ischemia-reperfusion injury [1]. Notably, this technique is different from intermittent pneumatic compression, which applies a non-ischemic pressure to facilitate lymphatic and venous return [2]. Previous studies have reported that IPC enhances the maximal and whole-body performance by improving peripheral muscle function and central cardiovascular adaptation [3, 4, 5, 6, 7]. Moreover, IPC enhances cycling, swimming and running performance in people who are either physically active or non-athletes [8, 9, 10]. Nevertheless, a meta-analysis study [11] concluded that IPC has beneficial effect on aerobic (ES
Despite the reported ergogenic effect, the mechanisms underlying the beneficial effects are still not fully clarified. Animal studies indicated that IPC might increase intramuscular adenosine triphosphate-sensi-tive potassium channels and adenosine levels for a protective effect on circulation and improved blood flow in muscle [13, 14]. Studies also indicated that IPC might affect muscle metabolism during reperfusion by increasing phosphocreatine production and improving muscle function after reperfusion in both humans and rats [15, 16, 17, 18]. Furthermore, IPC optimizes local blood flow and muscle contraction in humans [10, 19, 20]. The increased blood flow could contribute to the removal of lactate metabolites [21, 22]. Enhanced blood flow could also improve muscle contraction efficiency by increasing oxygen delivery and excitation-contraction coupling [23]. Muscle perfusion, oxygen uptake, and repeated force capacity have been shown to increase in strength-trained athletes after IPC [20].
Oxidative metabolism is a crucial determinant of exercise [10]. Ischemic preconditioning could reduce the oxygen saturation of the arm during muscle ischemia and increase oxygen saturation during reperfusion. Previous studies indicated that oxygen consumption at the muscle level increases after IPC [10, 15, 20]. However, oxygen saturation was found unchanged in the other arm and the thigh of the same side during IPC [7]. Similar results were found for IPC applied on bilateral thighs [8] or unilateral upper arm [9]. Briefly, IPC may affect oxygen saturation and accelerate the oxygen uptake only in the intermittent ischemia limb.
Accordingly, it is important to identify the hemodynamics during exercise and muscular functions following IPC. Although recent works attempted to determine the relationship between the ergogenic effect of IPC and muscle function, limited data are available on the role of muscular deoxygenation status during exercise after IPC [10, 20, 24]. In the present study, we aimed to examine the effects of IPC applied to bilateral thighs on isokinetic muscular strength and endurance of lower limbs in young non-athletic males and use near-infrared spectrometer (NIRS) to keep monitoring blood flow and oxygenation status during exercise. We hypothesized that IPC would enhance local muscular function by improving blood flow and oxygenation in lower limbs.
Protocol of this study. IPC (ischemic preconditioning): 3 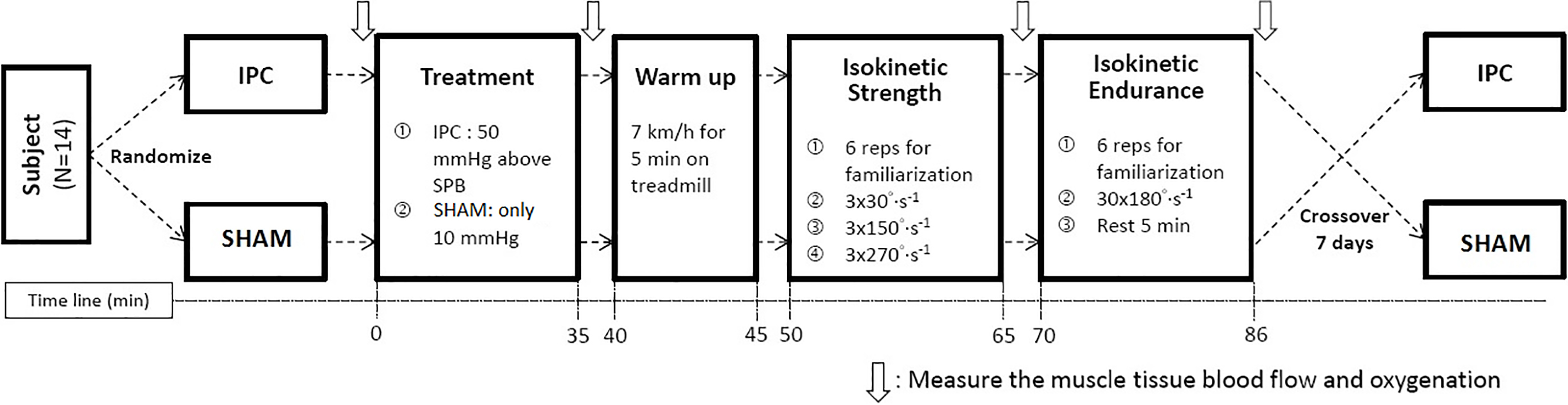
Participants
Based on the results of deoxygenated hemoglobin from the previous study [19], a sample size of 13 is required for detecting a difference between groups for a two-sided analysis with
Experimental design of the study
All participants refrained from consuming alcohol, caffeine, and additional nutritional supplements 24 hours before testing and strenuous exercise three days before testing. A counterbalanced, crossover study was designed. Since the participants were healthy non-athletic adults, the experimental procedures were modified by reducing the intensity of warm-up from the generally employed protocol designed for athletes [19, 20]. Participants reported to the laboratory twice and performed the same tests on both days. Before the intervention, systolic blood pressure was measured. Participants sat on chairs with the arms supported horizontally, palms turned upward and both the cubital fossa and the upper arm at the level of the mid-sternum. After IPC or SHAM intervention, participants rested for 5 min and then performed a 5-min warm-up on a treadmill at a velocity of 7 km
Ischemic preconditioning and SHAM interventions
IPC technique was modified from previous studies that induced the exercise performance benefits with the application of the lowest pressure in non-athletic adults [4]. Briefly, IPC was performed with the participants in the supine position to block the blood of the femoral artery. The occlusion cuffs (14.2 cm wide, Spirit
Isokinetic muscular strength after IPC or SHAM interventions at the angular velocities of (A) 30
A Biodex isokinetic dynamometer (Biodex System Pro 3, USA) was used to assess the knee-joint isokinetic peak torque according to the operating manual. The dynamometer was corrected for gravity before each test. Participants were placed in the dynamometer seat at an angle of 90
Tissue oxygenation
A frequency-domain tissue NIRS (Oxiplex TS Oximete ISS, Champaign, IL, USA) was used to detect blood perfusion of the exercising muscle. The sensor of the NIRS was applied over the vastus lateralis muscle of the dominant leg in the supine and sitting positions before and after IPC or SHAM interventions and during continuous 30-repetition knee flexions and extensions, respectively. Oxygenated hemoglobin (O
Statistical analysis
Data were analyzed using SPSS 17.0 software (SPSS, Chicago, IL, USA). Shapiro-Wilk test was performed to examine the distribution normality. Paired t-tests or Wilcoxon signed-rank test were used to assess differences in NIRS variables (O
Results
Except for
Isokinetic muscular strength and endurance
Figure 2 presents data for isokinetic muscle strength in healthy males after IPC or SHAM interventions at the test velocities. Isokinetic muscular strength did not differ between IPC and SHAM interventions for the three angular velocities. The mean power, total work, and endurance index with 30 repetitions of extension at 180
Isokinetic muscular endurance performance of (A) total work, (B) mean power, and (C) endurance index after IPC or SHAM interventions.
NIRS parameters before and after IPC or SHAM interventions. *: significantly changed compared with before intervention (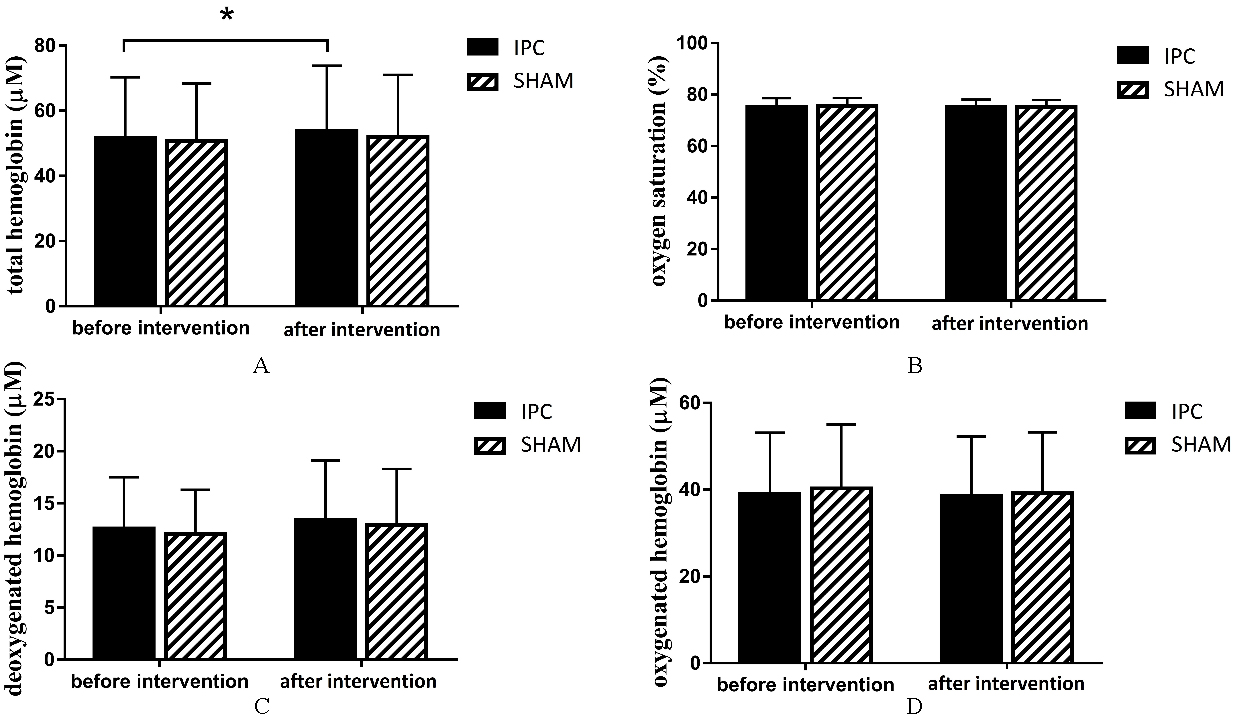
NIRS parameters during continuous 30-repetition knee flexions and extensions after IPC or SHAM interventions.
Change in NIRS parameters during continuous 30-repetition knee flexions and extensions after IPC or SHAM interventions. *: significantly different compared with IPC intervention (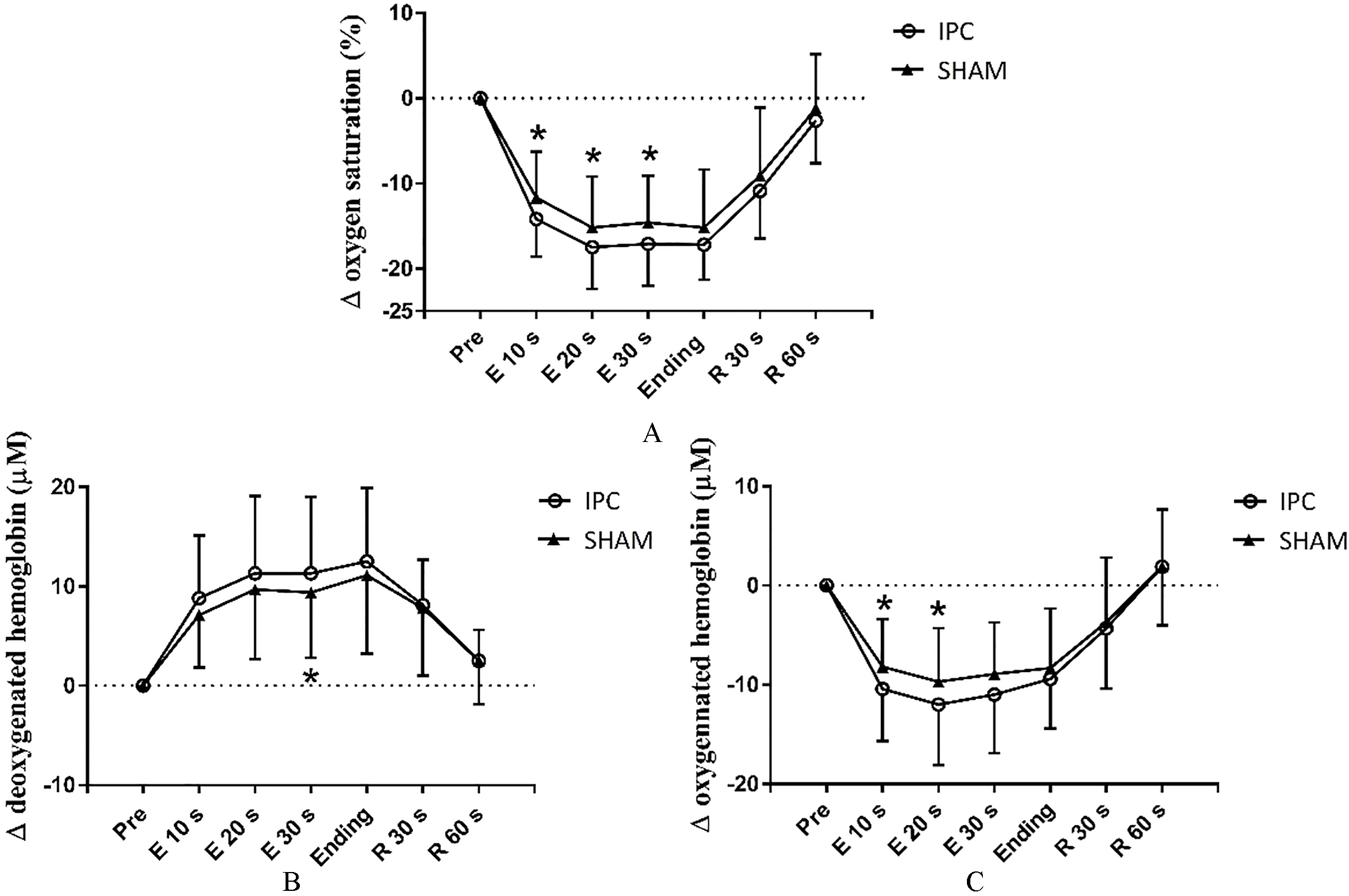
The tHb significantly increased after IPC intervention (57.6
Discussion
The present study focuses on the isokinetic muscular function of lower extremity and local hemodynamics after IPC in healthy non-athletic male, excluding peripheral muscle function from whole-body performance and minimizes the impact of central cardiovascular adaptation. Our results showed that acute IPC with pressure of 170 mmHg before isokinetic knee extension and flexion stimulated the local oxygenation status without influencing local muscular function.
In accordance with previous studies, we observed higher blood perfusion and faster oxygen consumption locally after IPC [10, 20, 24, 30]. One study demonstrated that the blood levels of nitric oxide (NO) metabolites are elevated after IPC [31]. Because NO is secreted by endothelial cells following shear str-ess [32], which occurs with reperfusion of IPC, the beneficial effect of IPC on vascular function appears to be regulated by NO. Notably, since ischemic preconditioning does not alter cardiac performance [3, 4, 5, 10], vascular adaptation is considered to occur peripherally but not systemically.
Previous studies indicated that IPC alters oxygen saturation of the treated arm during muscle ischemia and reperfusion and suggested that IPC is an important element in warm-up procedures in preparation for maximal exercise [7, 9]. Correspondingly, the peak and average force of maximum voluntary knee extension tend to increase after IPC [20]. Furthermore, ischemic preconditioning also improves endurance performance. Time to exhaustion in severe-intensity cycling exercise enhanced during the work-to-work test after IPC [10], and the time to task failure was longer in local muscular endurance [24]. Exercise economy and time-trial performance are also improved in endurance athletes [33]. In contrast, although IPC was found to improve performance in both aerobic and anaerobic exercises with a large metabolic requirement [11], we did not find any improvement in isokinetic muscular strength or endurance. Since the beneficial effects of IPC may depend on the intensity, duration, and type of exercise, which is not clarified, and individual variation may exist [34], the mode of exercise test, i.e., isokinetic exercise, in our study may not fully represent the ergogenic effect of IPC. Besides, although the type of warm-up intervention and exercise testing that we chose were different from the conventionally employed IPC procedures [19, 20] and, may have led to different experimental results, this process is indispensable before performing a maximum exercise testing [27]. Specifically, in this study, we applied a relatively low-intensity walking warm-up, which may reduce such bias.
In addition, the circumference of the thigh, limb composition, and limb mass may affect the pressure applied to the underlying soft tissue [23]. In our study, we measured the systolic blood pressure of the arm with participants in a seated position and then applied IPC to the thigh with participants in a supine position. Although the systolic blood pressure is significantly higher in the supine than sitting position [35, 36], the pressure in the legs is also higher than that in the arms [37]. Therefore, we considered individual differences in systolic blood pressure to modify IPC protocol [4]. Previous studies showed that full femoral occlusion would not occur [17] and the effects of IPC could be induced in relative hypoxia with systolic blood pressure plus 15 mmHg [9]. Although the resting concentration of tHb is elevated in our study, which indicates the validity of IPC, we still suggest that occlusion pressure with IPC should be based on femoral blood pressure in the supine position when applied to the lower limbs in a future study to decrease the systematic error. Besides, as a plateau of HHb is a sign of occlusion, we also suggest future researchers to keep monitoring the hemodynamics during IPC.
Furthermore, the minimal pressure of IPC to obtain the ergogenic effect is still equivocal. Our finding is accompanied with the emerging evidence that ischemia pressure should be set from 200 to 220 mmHg to obtain ergogenic effects. The present study also suggests that applying 50 mmHg greater than systolic blood pressure (i.e.
Conclusion
In summary, the present study argues against the effect of ischemic preconditioning on isokinetic muscular function, which revealed that muscular strength and endurance do not reflect the beneficial efficacy of IPC on the local muscle perfusion and oxygen uptake. Our results provide further insight into the underlying mechanism of the ergogenic effect. However, the benefits of IPC on different muscular functions and the empirical mechanism should be investigated in the future.
Footnotes
Acknowledgments
The authors would like to thank all subjects for participating and helping in this study.
Conflict of interest
The authors have no conflict of interest to declare. No funding was received for this study.