
Abstract
BACKGROUND:
It is unknown whether a session of isometric handgrip (IHG) exercise can influence the blood pressure of hypertensive and normotensive individuals.
OBJECTIVE:
To compare post exercise hypotension among groups with different resting blood pressure (BP) levels.
METHODS:
56 Malay male volunteers (12 normotensive, 14 pre-hypertensive, 19 hypertensive stage 1, and 11 hypertensive stage 2) completed four sets of 2-minute isometric handgrip exercises at 30% of their maximum handgrip contraction with a one-minute break between the sets. Systolic BP (SBP), diastolic BP (DBP), pulse pressure (PP), mean arterial pressure (MAP), resting heart rate (RHR), and handgrip strength (HGS) were measured before and after an hour of IHG exercise. A paired sample
RESULTS:
All parameters, except RHR and PP, were significantly changed following the exercise across the BP groups. The SBP, MAP, and HGS were greatly reduced among hypertensive stage 1 (SBP
CONCLUSIONS:
The current study discovered a significant reduction in BP among hypertensive stage 1 and 2 individuals after a session of IHG exercise.
Introduction
Hypertension is one of the most important risk indicators for serious illnesses such as heart disease and stroke [1]. While antihypertensive medicine is effective in the treatment of hypertension, it can occasionally cause side effects if consumed over a long period [2]. Therefore, other non-pharmacological approaches such as dietary modifications, limiting sodium intake, or exercise are much safer and more effective in preventing hypertension. It is undeniable that conducting dynamic workouts such as walking, and swimming regularly can help lower or avoid high blood pressure (BP) in hypertensive or normotensive individuals. However, many people may not be able to tailor to this type of exercise due to unavailability of time or restricted by other medical conditions [3]. Research also reported approximately 50% less adherence to a dynamic exercise program and less than 20% of adults were found to be discontinued in aerobic exercise programs within 3 to 6 months [4].
Recently, the isometric exercise done at lower intensity such as at 25% or moderate intensity, such as 50% of maximal voluntary contraction (MVC) helps to reduce resting BP [5]. It has been reported that an isometric exercise training undertaken by less than one hour per week over a period of less than 10 weeks reduces by about 10 mmHg and 7 mmHg in systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively [5]. Given the above-mentioned findings, isometric exercise may enable increased adherence to treatment compared with another approach in BP management as it is easy to execute and involves the use of fewer muscle groups with less time consuming. In addition, isometric exercise can be a promising, safe, and efficient BP-lowering approach due to the findings of several studies that reported no overload in cardiovascular changes and hemodynamic parameters immediately after the end of the first isometric exercise training session [6, 7, 8].
A single exercise session can cause post-exercise hypotension, or a drop in BP [9]. Chronic adaptations that may postpone or prevent the onset of hypertension are significantly influenced by repeated acute exercise episodes [9]. According to a previous study, acute isometric exercise can be used to gauge the severity of a chronic response before beginning an exercise training program [10]. Given its ability to forecast how much BP will drop after long-term training treatments, acute exercise would have significant therapeutic implications for the treatment of pre-hypertension and hypertension. A little drop in BP during acute exercise may serve as an indicator for people who are less sensitive to long-term exercise training. People who are not receptive to this sort of exercise may thus be recommended different forms of exercise or approach.
The current body of research reveals the dearth of data on the immediate effects of a single bout of isometric handgrip (IHG) exercise on BP measures in hypertensive people [8, 11, 12]. In contrast to IHG exercise with a lower overload of work at 3% MVC, Souza et al. [13]’s study found that IHG exercise with a larger overload of work at 30% of MVC caused post-isometric exercise hypotension in hypertensive elderly people. SBP was considerably lower following IHG training during everyday activities compared to the control session in research including fifteen healthy persons with pre- or stage 1 hypertension [11]. In contrast, Farah et al. [8] found single session of IHG exercise performed with different intensities and volumes did not reduce the BP of hypertensive. The study by Farah et al. [8], however, included both men and women, with sample size was small, making it impossible to rule out the impact of sex differences on the processes driving cardiovascular responses to exercise. Several possible constraints, such as the lack of standardisation in exercise programmes, the assessment of exercise, and inter-individual variations, have hindered a definite conclusion on the utility of isometric exercise in the management of hypertension.
The reductions in BP induced by isometric exercise training are assumed to differ among individuals who are having a different level of the BP value. A study conducted by Queiroz et al. [14] addressed this question but have focused on dynamic resistance exercise and found a similar response on post-exercising hypotension (PEH) for both normotensive and hypertensive populations. A comparison between normotensive and hypertensive subjects may clarify the variation in BP response following IHG exercise. There is also a need to know whether the PEH following an isometric exercise session reported mostly for Caucasian populations [13, 15] also appears for other populations, particularly among the Malay population because genetic diversity may also occur in different ethnicity. It is yet uncertain if isometric exercise-related hypotensive effects exist in the Malay population, even though a single session of aerobic exercise did not significantly lower BP right away in the African and Asian group [16]. Given that Malaysia still has a hypertension prevalence of over 30%, higher than that of other countries like China (25.2%) and Singapore (23.5%) [17, 18], it is important to identify hypotensive consequences due to a single session of isometric exercise in both normotensive and hypertensive Malay population in order to support the idea of isometric exercise as primary intervention for the prevention and management of hypertension.
Therefore, the purpose of this study was to examine whether a session of IHG exercise would elicit greater BP reduction for Malay individuals with different levels of BP. We predicted that those with higher BP values would see a greater drop in BP after only one session of IHG exercise. In addition, since muscular strength affects how the BP responds to acute isometric exercise in which that higher BP was found to be associated with greater handgrip strength [19], we also hypothesized that individuals with high resting BP would exhibit reduced muscle strength compared to those with normal BP after a single of isometric exercise session. With aim to further support previous findings on the recommendation of isometric exercise for preventing or controlling hypertension, the results of the present study might offer early insights about the potential use of this form exercise in Malay population.
Methods
Participants
Given that the magnitude of the BP response following isometric exercise was reported differed by gender [20], in which was much lower in women, and a changed autonomic response causes the size of the BP response to be more prominent in senior people than in young ones [21], the present study recruited a total of 56 adults males participants classified as untrained, aged 34.5
Based on guideline released by The American College of Cardiology (ACC) and the American Heart Association (AHA) [22], 12 participants are healthy and categorized as normotensive (SBP
The sample size was calculated using the GPower 3.1 in which the study’s statistical power was set at 0.80 with 95 % of the interval of confidence and 0.25 impact size [Calculated sample size
Protocol
Before the exercise testing, the anthropometrical data, including body weight, body height, body mass index (BMI), and body fat were collected from the participants. A handheld stadiometer was used to assess the body height of the subject (Seca 213, Seca Company, United States). Meanwhile, an Omron KARADA Scan Body Composition & Scale (HBF-362, Omron Company, Japan) was used to measure the participants’ body weight, body mass index, and body fat. Before evaluating research factors, participants were asked to withdraw from physical exercise and consume caffeinated drinks within 24 hours of examination. A hand dynamometer (Takei A5401, Scientific Instruments Co. Ltd., Japan) was used for IHG tests, while a non-invasive, passive brachial oscillometer measured BP values (Omron HEM907XL, Omron Healthcare, Inc., USA). We selected the Takei dynamometer because it can be adjustable rectified and complacent handle shape, electromechanical system and a digital or analog display. Previous research has also proven that Takei dynamometer is more accurate and valid than other tools for evaluating strength [23, 24].
The SBP, DBP, mean arterial pressure (MAP), pulse pressure (PP), and resting heart rate (RHR) variables had been determined before starting the IHG exercise. MAP and PP were calculated as MAP
Flowchart of research.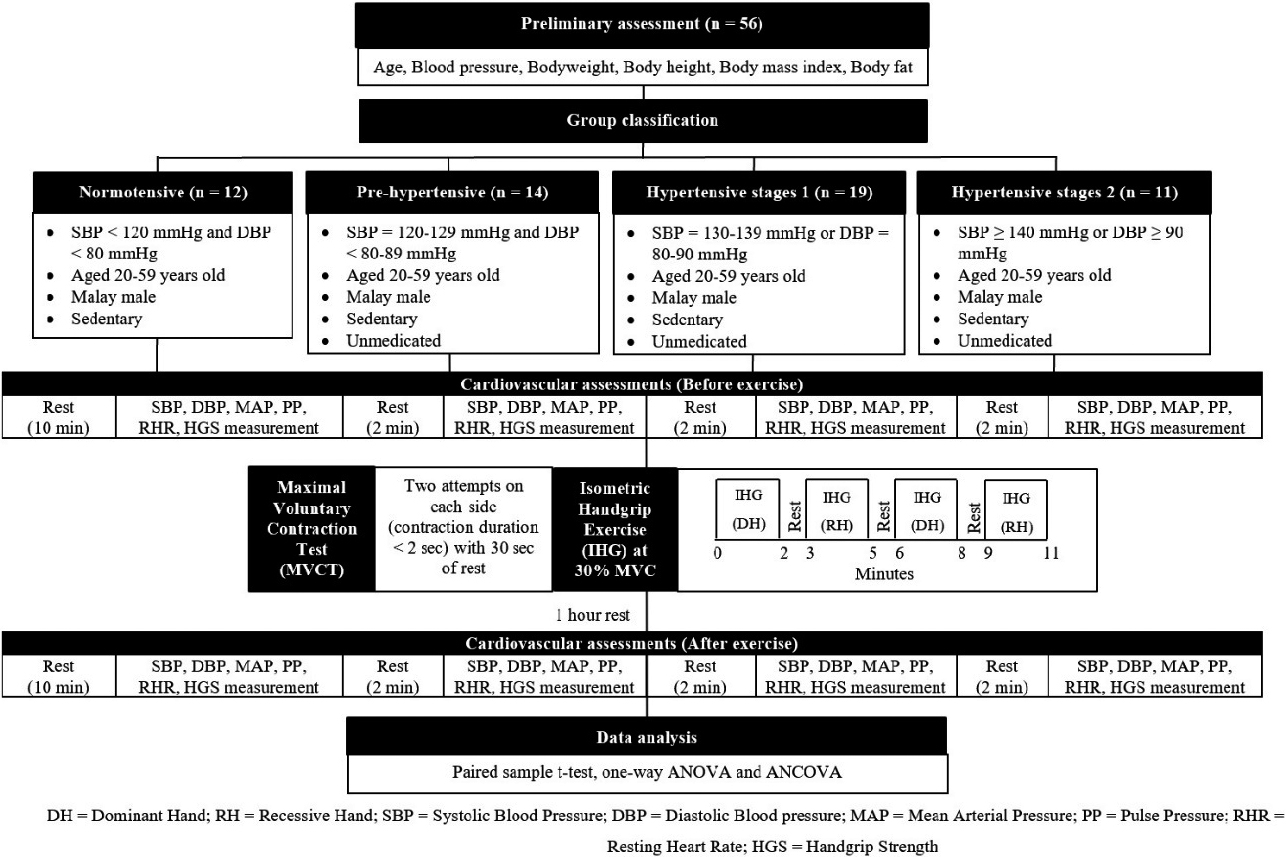
The protocol of IHG exercise used in this study was based on positive findings obtained by Millar et al.’s [26] experiment. Before the exercise session, the left and right MVC values of participants were calculated with two attempts at contractions of less than 2 seconds on each side and separated by 30 seconds of rest. If the gap from both recordings was less than five percent, the highest MVC was taken for the participant’s hand. When measurements were different by more than 5 percent, further attempts were made within 1 minute to achieve a stable limit. All participants performed unilateral alternate IHG exercises with the working arm reaching towards the front starting with the dominant hand in a sitting position. The participants completed four trials of IHG exercise for 2 minutes at 30 percent of their MVC with a break of 1-minutes between each session. The total time of the IHG exercise is 11 minutes only. Figure 1 depicts a flowchart of the research design.
The descriptive information is defined as a mean
Descriptive characteristic of participants according to BP category
Descriptive characteristic of participants according to BP category
Note. Data are shown as mean
Acute changes after a session of IHG exercise in all participants
Note. Data are shown as mean
Participant’s characteristic
Table 1 shows the demographic characteristics of participants according to their BP category. A one-way ANOVA revealed that there were no statistically significant differences in age (F (3, 52)
For DBP, the homogeneity of variance was met (
The acute effect of an IHG exercise
Table 2 shows the BP and handgrip strength responses in the whole sample (regardless of their BP category) following a single session of IHG exercise. The paired sample
Two-way repeated measure ANCOVA on cardiovascular and handgrip strength responses to a session of IHG exercise according to BP category with controlling age
Two-way repeated measure ANCOVA on cardiovascular and handgrip strength responses to a session of IHG exercise according to BP category with controlling age
Note. Data pre-exercise and post-exercise are shown as mean
Table 3 reporting two-way repeated measure ANCOVA results on the effectiveness of IHG exercise on studied variables between four groups whilst controlling for age. Levene’s test and normality checks were carried out and the assumptions were met. The analyses revealed that there was a statistically significant difference between the BP groups on the combined dependent variables after controlling for age (F (15, 130.148)
After adjusting for age, there was a significant difference in mean changes of SBP value [F (3, 51)
Estimated marginal means of changes in SBP in four BP category groups with controlling age.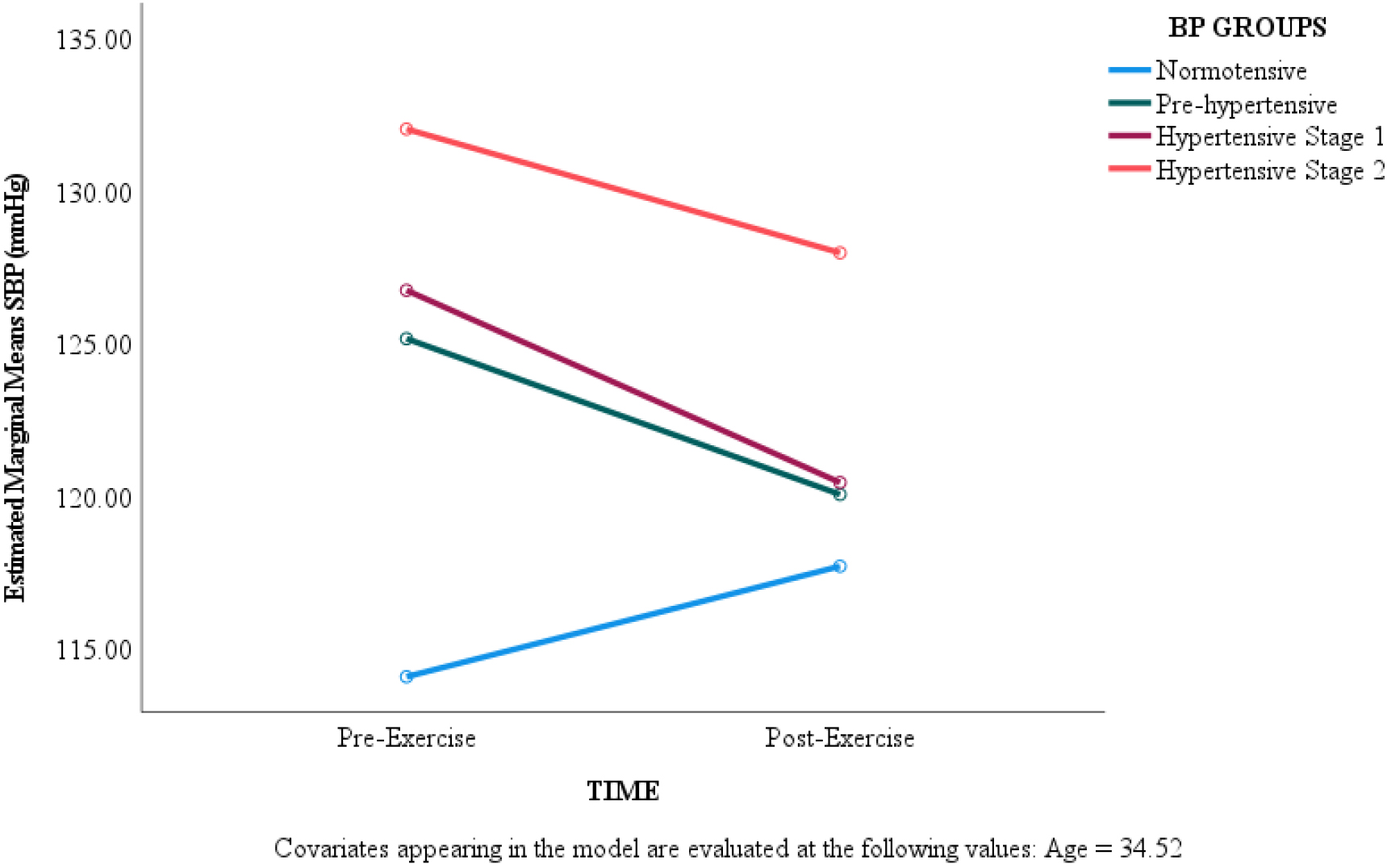
The analyses also demonstrate that there was a significant difference in mean changes of DBP value [F (3, 51)
Estimated marginal means of changes in DBP in four BP category groups with controlling age.
The results also show that the mean changes in MAP value across the BP groups were significantly different [F (3, 51)
Estimated marginal means of changes in MAP in four BP category groups with controlling age.
For HGS values, there was a significant difference across the BP groups [F (3, 51)
Estimated marginal means of changes in HGS in four BP category groups with controlling age.
This study has shown two things: (i) a single session of IHG exercise reduces SBP, DBP, MAP, and HGS in Malay individuals; and (ii) the degree of IHG effect on SBP, DBP, MAP, and HGS appear to differ between four BP groups. Regardless of BP status (normotensive or hypertensive), the analysis demonstrates that a session of IHG exercises can elicit a reduction in cardiovascular parameters except PP and RHR. Our finding contradicts to study by Silva et al. [27] who found that an IHG session does not elicit a reduction in cardiovascular variables (SBP and DBP) in medicated hypertensives although the same exercise protocol was implemented in both studies. However, this discrepancy could be that our study includes unmedicated hypertensive whilst Silva et al. [27] implemented the study among the medicated hypertensive and mixture of gender. According to reports, the BP response to isometric exercise varied by gender [20]. As a result, findings from missing [27] should be interpreted with caution. It was also thought that medications will increase the autonomic function of hypertensive patients thus the ability of medicated patients to respond to the IHG training stimulus may have been reduced and may require a high intensity or longer muscle contraction and the number of contractions of IHG stimulation. In other study by Ash et al. [28], IHG exercise did not also lower ambulatory SBP and DBP over 24 hours. Disparities between our findings and those of Ash et al. [28] may potentially have been caused by variations in the research populations’ demographic characteristics and protocol. While our study solely focused on one racial group, Ash et al. [28]’s study participants were mixed or multiracial.
Our findings indicate that IHG exercise will typically have a consistent, immediate effect on patients’ cardiovascular variables, independent of their conditions. Regardless of different baseline BP levels, the BP and heart rate parameters returned to or below the resting level after the IHG exercise session. IHG exercise in those with normal or high BP as a treatment or lifestyle modification has the potential to reduce other cardiovascular events since the reduction of 2 mmHg in BP reduced the risk of cardiovascular disease and stroke mortality [29]. Our investigation demonstrates that the IHG exercise stimulus which is simpler at low intensity (30% of MVC) contracted for two minutes repeated four times in a total of 11 minutes able to elicit the anticipated responses in both healthy and clinical populations, to markedly shows that this simple exercise regime could be able recognized as one of the lifestyle modifications for managing health, particularly to BP.
Such findings indicated that exercise with IHG can be important to a person, especially patients with hypertension, in reducing the rest of BP for certain occasions. Our study supports that arm isometric exercise such as handgrip which is simpler to perform and less muscle involved was effective as a leg isometric exercise in eliciting reduction in the BP [30] as a reduction in SBP, DBP, and MAP was noted after the exercise session. It is thought that if the isometric exercise been practiced for longer time, it can ensure long-term adherence as it is safe, easy to perform, and does not require a higher intensity of training or more total exercise time in aid to reducing BP as well as to increase muscle strength.
A systematic review conducted by Farah et al. [8] found that there were limited studies have been focused on the acute effect of IHG. In addition, there is variability in the findings where a previous study among normotensive people found that SBP remained unchanged immediately after exercise [31, 32]. Meanwhile, it increased in another study after 60 minutes among hypertensive individuals [6]. The variety in the experimental design and exercise modes might be responsible for this distinction findings. The function of different baseline BP between hypertensive and normotensive individuals in post-exercise effect on cardiovascular variables is not well described, and there are limited studies involving unmedicated hypertensive patients. Some studies have suggested that those with higher baseline BP will have a greater reaction on their cardiovascular status following the exercise although Fisher [33] discovered that BP categorization does not affect the magnitude of reduction of BP after a different type of resistance exercise. It is necessary to examine the extent to which normotensives and hypertensives experience PEH after IHG exercise to evaluate whether these people benefit from this exercise regime.
The higher SBP reduction among hypertensive could partly be explained by their higher baseline BP values. It illustrates the observations by Millar et al. [34] which indicates that normotensive people with higher baseline SBP values have a more marked decline following IHG exercise than those with lower baseline values. This scenario is likely to have similar findings to those found by Wiley et al. [35] in which they reported a greater reduction in hypertensive patients’ BP following isometric exercise compared with normotensive individuals. This can, in theory, give rise to the idea created by Badrov et al. [36], who had previously suggested that individuals with higher baseline BP values may have a greater capacity to reduce BP after IHG exercise compared to those with lower baseline BP. Those with higher resting BP, such as hypertensive patients, are thought to have greater sympathetic activity at rest which could lead to a greater hemodynamic reaction to sympathetic activation [37]. Because normotensive participants in this study had already reposing BP within the normal range, the magnitude of BP drops was not obvious and for those with the highest BP was seen as being expected.
In this present study, we found that the reduction in resting SBP after an IHG exercise session was significantly greater among the hypertensive stage 1 group by 6.3 mmHg. The reduction in SBP observed in this study was similar to the results reported by Cleroux et al. [38] who examined the acute effect of aerobic exercise with cycle ergometry at 50% VO
As expected, we found that those with high BP value exhibit reduced muscle strength compared to those with normal BP after a single of isometric exercise session. This finding indicates that baseline handgrip strength mediates the BP response to isometric handgrip exercise between individual with different level of resting BP as proposed by previous study [19]. Although the mechanism underlying the confounding effects of handgrip strength on BP responses were not explored in the current investigation, we assume that they may be related to variations in the physiology of arterial mechanical properties and central and peripheral BP between the normotensive and hypertensive individuals [39]. Further research is warranted to confirm the mechanism of this observation. Therefore, the current finding suggests that handgrip strength should be taken into account for future research, particularly when looking at persons with several levels of BP.
There are several limitations about the current study. The first drawback stemmed from the fact that we did not investigate the mechanism by which IHG workouts lower BP. The decrease in BP values seen in this study could be explained by several different mechanisms, including a decrease in parasympathetic nerve activity [40] or an increase in repetitive hydrogen (pH) brought on by muscle fatigue and lactate production, which acts as a metabolic stimulus during exercise [30]. Future research should consider a relevant expansion because this study did not assess the parameters. The second restriction was caused by potential interindividual variables, such as genetic profiles associated to cardiovascular regulation, which call for more investigation to confirm this proposed mechanism and may possibly affect the results of this study.
Despite the aforementioned limitations, confidence in the validity of the present findings is increased by the fact that our research has several significant benefits because the subjects were relatively homogenous with the standardization of the experiment in terms of age, gender, racial and the participants underwent familiarization approaches despite the apprehension-induced variation in baseline measurements.
Conclusions
An IHG exercise session conducted in the present study resulted in a reduction of the cardiovascular variables in both hypertensive and normotensive Malay populations. Nevertheless, a longitudinal study of IHG in Malay populations is warranted to be conducted in future to see if the dramatic effects of IHG as observed in this study can be beneficial for long term. The IHG exercise demonstrated in this study may offer a safe and efficient form of exercise, particularly for unmedicated hypertensive individuals. The different baseline resting BP was shown to describe an interindividual variance in acute BP responses where individuals with the highest resting BP appeared to have a lower resting SBP after a single session of IHG exercise than those individuals with lower BP.
Author contributions
CONCEPTION: Hazwani Ahmad Yusof.
PERFORMANCE OF WORK: Wan Mohammad Nazrin Wan Yusof and Wan Nor Syahirah Nasaruddin.
INTERPRETATION OR ANALYSIS OF DATA: Hazwani Ahmad Yusof.
PREPARATION OF THE MANUSCRIPT: Wan Mohammad Nazrin Wan Yusof and Hazwani Ahmad Yusof.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ahmad Munir Che Muhamed and Rohayu Hami.
SUPERVISION: Hazwani Ahmad Yusof.
Ethical considerations
Participants were asked about their details after participants signed and completed the consent form. Following the ethical standards of the Helsinki Declaration, the study protocol was approved by the Human Research Ethics Committee of the University (USM/JEPeM/16100399).
Funding
This article is part of UNIVERSITI SAINS MALAYSIA-funded work (304.CIPPT.6315037).
Footnotes
Acknowledgments
The authors thank the university for providing facilities and all participants which enabled this research to work.
Conflict of interest
The authors have no conflicts of interest to report.